
Abstract
Objective:
In this in vitro study, cross-polarization optical coherence tomography (CP-OCT) was used to evaluate microleakage in dental composite restorations bonded to enamel with two types of one-step self-etching (SE) adhesives.
Background data:
One-step SE adhesives were proposed to simplify bonding of composite restorations. However, bonding of these simplified adhesive to dental enamel is still questionable. OCT is a promising diagnostic tool that allows micron-scale imaging of biological tissues and structures.
Methods:
Class-V cavities (4-mm diameter × 1-mm depth) were prepared on the labial surfaces of extracted human anterior teeth with margins and floor located in enamel. The cavities were then divided into two groups (n = 5) and restored with either Tetric N-Bond Universal (Ivoclar Vivadent, Liechtenstein) or Palfique Bond (Tokuyama Dental Corporation, Japan), followed by Estelite Flow Quick flowable composite (Tokuyama Dental Corporation). After storage in 100% humidity for 24 h, specimens were immersed in ammoniacal silver nitrate solution for another 24 h. Later, they were rinsed and immersed in photo-developing solution under fluorescent light for 8 h. CP-OCT at 1310 nm center wavelength was used to scan seven two-dimensional cross-sectional images from each specimen. Each cross-sectional image was analyzed using ImageJ software to quantify interfacial microleakage at the cavity floor.
Results:
Student's t-test showed significant difference between the tested adhesives (p < 0.05). Palfique Bond adhesive presented inferior interfacial adaptation as it obtained higher values of floor microleakage compared to Tetric N-Bond Universal adhesive group.
Conclusions:
CP-OCT enabled nondestructive quantitative assessment of microleakage in enamel dental restorations.
Introduction
W
Dental adhesives are being continuously developed attempting to simplify application procedures, increase bond strength to enamel and dentin, and improve interfacial adaptation of composite restorations. 4 Contemporary dental adhesives can be classified into two main categories as follows: acid etching systems and self-etching (SE) systems. In the acid etching systems, 30–40% concentration of phosphoric acid is used to remove the smear layer and expose the collagen fibrils over a depth of 3–5 μm. 5 Generally, these systems are considered to be aggressive and technique sensitive. 6
SE dental adhesives have been introduced to the market to decrease technique sensitivity and operative chair time. Unlike acid etching systems, SE adhesives contain acidic monomers that simultaneously demineralize and infiltrate the surface, eliminating the need for phosphoric acid etching. 4,5 SE adhesives can be supplied in either two-step or one-step system, so called “all-in-one adhesive,” in which different monomers and solvents of dissimilar properties are combined in single bottle. Based on their acidity, these SE adhesives can be strongly acidic (pH ≤1), moderately strong (pH 1–2), mild (pH ≈2), or ultramild (pH >2.5). 7 Nevertheless, the acidity of SE adhesives, even the strongest ones, is considered to be much lower than 35% phosphoric acid. Previous reports have confirmed adequate bonding performance of SE to dentin. 8 –10 However, concerns remain over their capability of enamel etching and bonding. 4,5
During clinical practice, dentists usually rely on visual and radiographic examination to assess existing restorations. Visual assessment solely is subjective and bears no information from underlying structures. 11 Likewise, radiographic examination can give false negative or false positive results, as the restoration's radiopacity might mask interfacial gaps. 12 While depending on these methods, interfacial defects can be missed easily or only detected at later stages when conservative treatment approach can't be implemented. Meanwhile, experimental adhesion studies usually rely on subjective assessment under microscope. Such methods require special specimen preparation such as dye application and sectioning in addition to polishing. 7,9,13
Recently, optical coherence tomography (OCT) has become a well-established modality in many medical fields for real-time, noninvasive subsurface detection. 14 –16 Near-infrared light is utilized to generate depth-resolved images from light-scattering media almost in real time without the use of radiation or magnetic field. In 1998, OCT has been introduced to dentistry as valuable tool for diagnosis of oral diseases and conditions. 17 It has been successfully used for caries diagnosis, monitoring remineralization, vertical root fracture, and crack detection. 18,19 In addition, OCT enabled quantitative measurements of the adaptive behavior of dental restorations at micron scale in two-dimensional (2D) and three-dimensional tomograms without cutting or processing. 10,20 –23
One of the functional extensions of OCT systems is cross-polarization OCT (CP-OCT). CP-OCT can construct high-resolution images with reduced specular reflection and enhanced contrast between different structures. 24 Many previous researches reported validity of CP-OCT in monitoring enamel demineralization. 24 –26 However, the ability of CP-OCT to evaluate sealing performance of dental adhesives was not reported. Therefore, the aim of this in vitro study is to assess enamel microleakage of one-step SE adhesives using CP-OCT. The null hypothesis tested was that there was no difference between tested groups in terms of interfacial microleakage under OCT.
Materials and Methods
Specimen preparation
A schematic drawing of study design is shown in Fig. 1, while Table 1 lists the materials used. Ten sound, caries, and restoration-free extracted human anterior teeth were collected and stored in saline solution. The teeth were debrided of calculus using periodontal scaler, and roots were separated using model trimmer. Standardized class V cavities were then prepared on the labial surfaces using regular diamond burs attached to high-speed turbine handpiece under water coolant, followed by superfine finishing burs. The cavities were 4 mm in width and 1 mm in depth with all margins and floors located in enamel. Then, two groups were randomly assigned based on adhesive material used (n = 5). In group A, the cavities were bonded with Tetric N-Bond Universal (Ivoclar Vivadent, Liechtenstein), while in group B, Palfique Bond (Tokuyama Dental Corporation, Japan) was used. Both adhesives were applied according to the manufacturers' instructions and light cured for 10 sec by LED light cure unit at 380–515 mW/cm2 (Bluephase N; Ivoclar Vivadent). Finally, both groups were restored with Estelite Flow Quick flowable composite (Tokuyama Dental Corporation) and cured for 20 sec using the same light-curing unit. After restoration, specimens were stored in 100% humidity and covered with varnish (Revlon) excluding margin of the restorations by 0.5 mm.
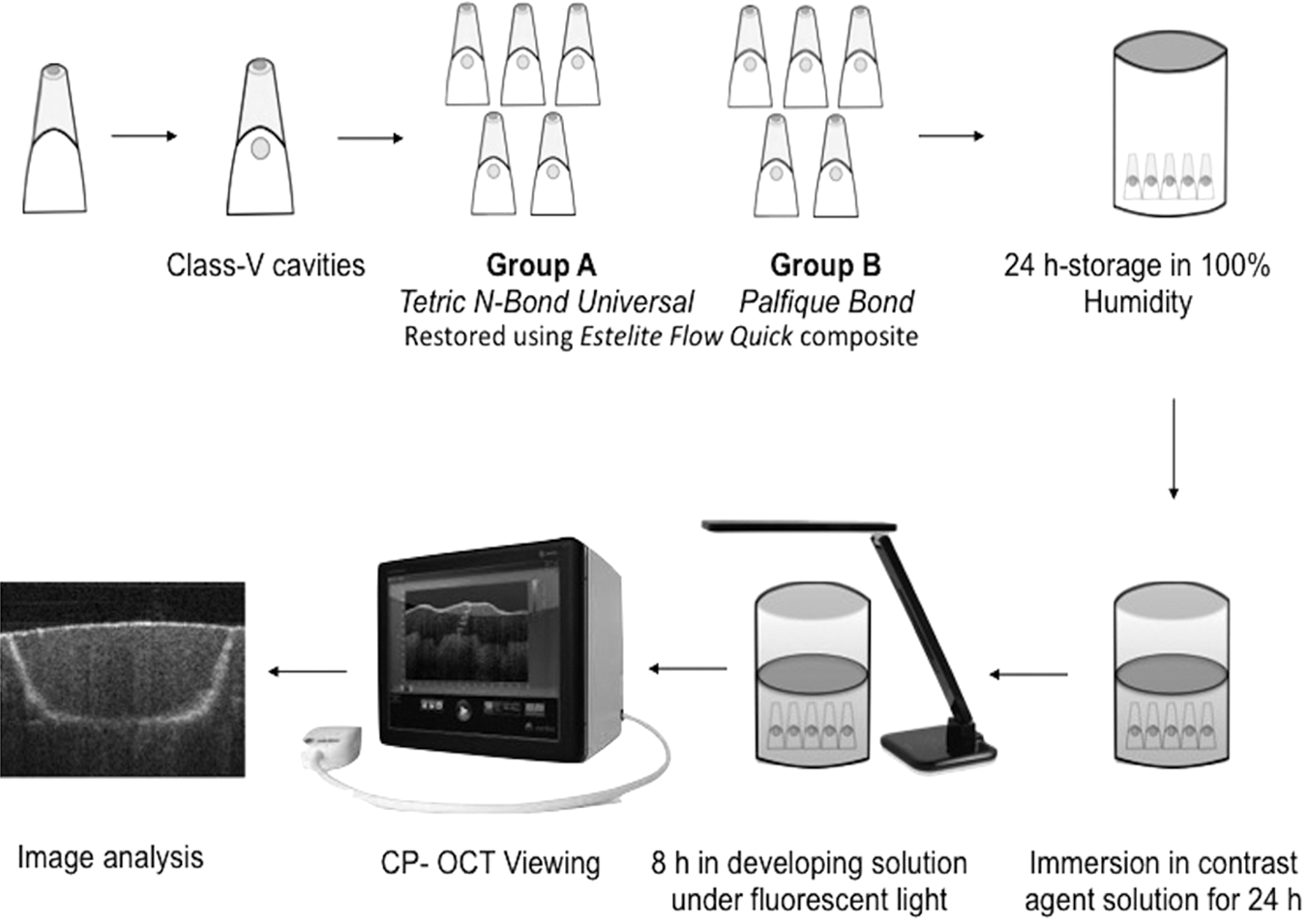
Schematic illustration of the study design.
Composition and Application Instructions of Materials Used in This Study
3D-SR, three-dimensional self-reinforcing monomer; Bis-GMA, bisphenol A glycidyl methacrylate; Bis-MPEPP, bisphenol A polyethoxy methacrylate; CQ, camphorquinone; D3MA, decandiol dimethacrylate; HEMA, 2-hydroxyethyl methacrylate; MCAP, methacrylated carboxylic acid polymer; MDP, 10-methacryloyloxydecyl dihydrogen phosphate; TEGDMA, triethylene glycol dimethacrylate; UDMA, urethane dimethacrylate.
Following Tay et al. 27 protocol, specimens were then immersed in ammoniacal silver nitrate solution for 24 h in dark environment. Afterward, they were rinsed by distilled water followed by immersion in photo-developing solution under fluorescent light for 8 h.
OCT imaging
A CP-OCT was used in this study (CP-OCT, IVS-300; Santec, Japan). This model utilizes a continuous wavelength-scanning laser with a high swept rate (30 kHz). The low coherence infrared light source is centered near 1330 nm wavelength and has a bandwidth of 100 nm. The lateral resolution of this CP-OCT is 30 μm, while axial resolution is 12 μm in air, which corresponds to 7–8 μm in tissues of 1.5 refractive index. The system sensitivity is more than 95 dB, and probe output power is within the safety limits defined by American National Standard Institute. 26
To detect microleakage, each specimen was positioned on micrometer stage, and the focused light beam was projected from OCT probe onto the specimen surface at 90°. Then, specimens were scanned in incisocervical direction where seven 2D cross-sectional images were obtained at 0.5 mm interval from each specimen. The size of each image was 500 × 924 pixels corresponding to 5 × 8.18 mm (x, z).
Image analysis
Raw OCT data were imported to ImageJ software (National Institutes of Health, Bethesda, MD). Median filter was applied (2 px radius), and images were converted to 8-bit grayscale followed by image binarization. The area of interest, cavity floor, was located on the binarized image, cropped, and gap percentage was calculated as:
where the gap is identified as the area of high intensity signals appearing as bright cluster, indicating interfacial microleakage. All bright clusters in the cavity floor were summed up and divided by total floor width. Two examiners measured gap percentage in each cross-section twice, and the mean value was calculated.
Statistical analysis
Student's t-test was used to compare between the tested groups (p < 0.05). The tested variable was the mean value of gap percentage at the cavity floor calculated by the two examiners.
Results
Representative cross-sectional images obtained from CP-OCT for both tested groups are shown in Figs. 2 –4. OCT image analysis enabled accurate measurement of the gap percentage. Voids formed due to entrapment of air during manipulation of composite during restoration were observed in some cross-sections (Fig. 4). B-scan images of group B specimens showed bright clusters at several locations along the cavity floor (Fig. 2a). In some cross-sections, these bright clusters extended throughout the cavity floor, indicating complete loss of interfacial seal (Fig. 2b). On the contrary, group A showed scant or no bright clusters, which suggest better floor adaptation (Figs. 3a and b). The mean gap percentage in group B was higher (88.68 ± 15.3) than group A (23.29 ± 28.6). Student's t-test demonstrated significant difference between the groups (p < 0.05).
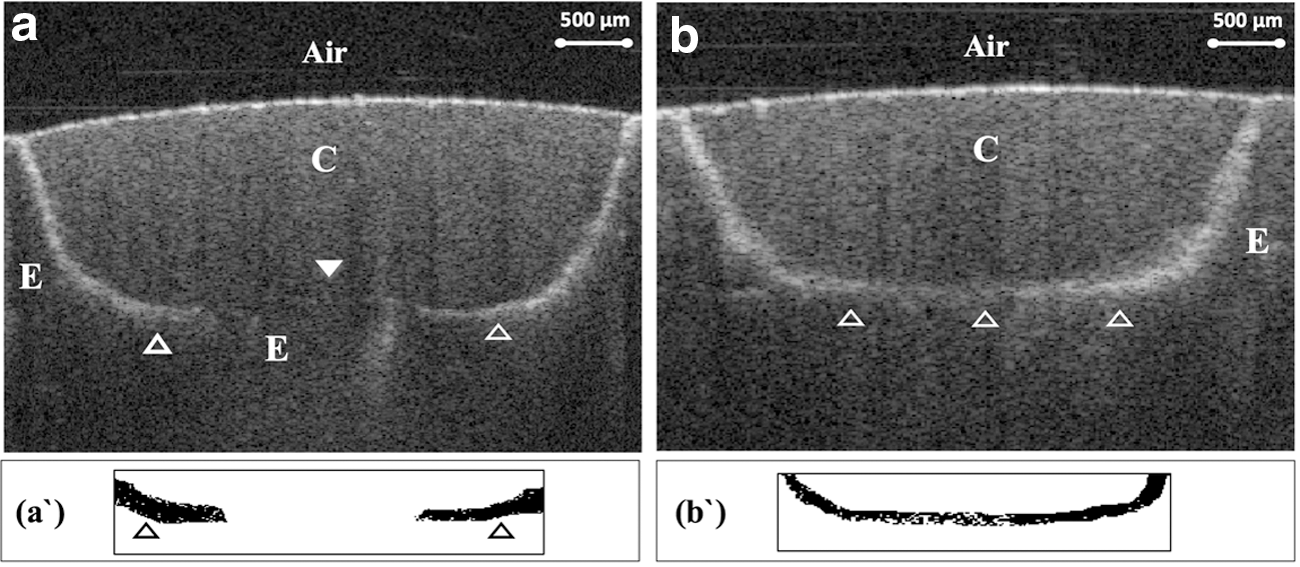
Representative cross-sectional CP-OCT images obtained from group B specimens.
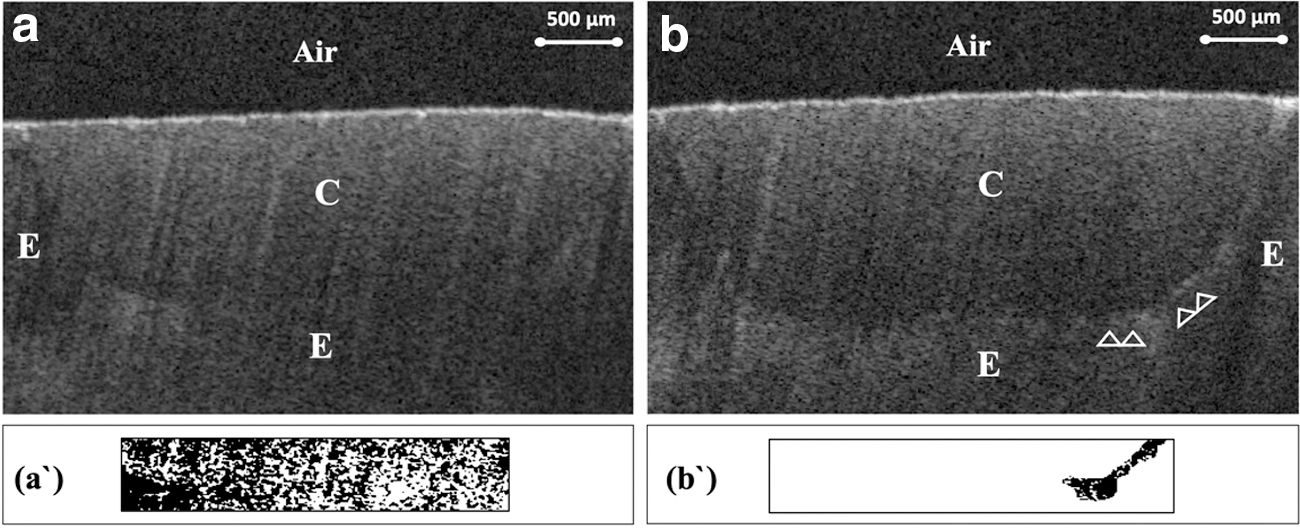
CP-OCT 2D images of selected specimens from group A.
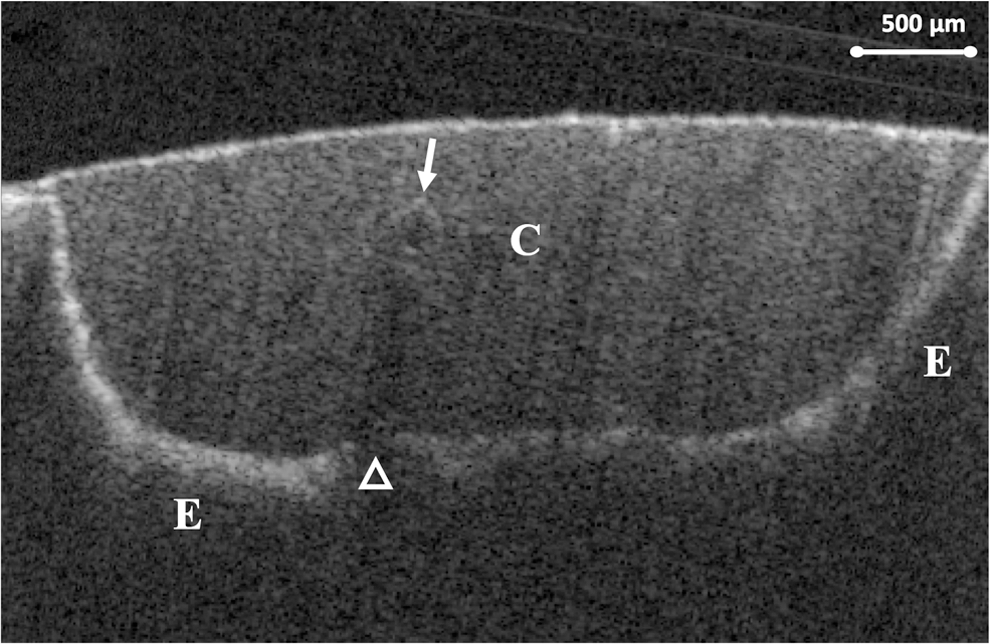
OCT B-scan obtained from group B specimen showing entrapped void (arrow). Signal intensity was lost beneath the void, masking a part of the cavity floor (blank arrowhead).
Discussion
In this in vitro study, CP-OCT was used as nondestructive objective tool to test enamel adhesion of two types of one-step SE. OCT has shown the potential for quantitative evaluation of interfacial adhesion of composite restorations in previous studies. 10,20,21 In OCT, interfacial defects can be distinguished due to optical reflectivity contrast. When the light is projected into the specimen, it passes through media with different composition and refractory indices. For example, the refractive index of teeth and composite ranges from 1.5 to 1.6 and it remarkably differs from that of air that is presumed to fill the gaps (n = 1). Such a difference in refractive index reflects the light and forms a peak in the backscatter signal, which appears as a bright area in OCT image. 20,21 In a previous study, combination of contrast agent and swept-source (SS)-OCT enabled accurate detection of interfacial microgaps. 23 Thus, silver nitrate was used in this study as a contrast agent. The presence of microgaps enhances silver granule uptake, which will highly reflect the light and provide a better contrast of interfacial gaps in the obtained CP-OCT cross-sections.
The adhesion mechanism of dental bonding systems is based upon an exchange process by which inorganic tooth structure is exchanged for synthetic resin. This process involves two phases. First phase consists of removing calcium phosphates of tooth surface creating microporosities, so called etching. The second phase involves penetration of resin monomers into these surface microporosities and their polymerization in situ, forming a layer of micromechanical interlocking with tooth structure after polymerization. 5 Previous adhesion studies reported resin penetration into enamel treated with SE adhesives comparable to phosphoric acid-etched enamel. 28 However, other studies have reported less pronounced enamel-etching pattern with the SE adhesive, because of the relatively inadequate pH. 9,13,29,30
In this study, OCT images of both one-step SE showed white clusters at the floor, indicating microleakage. This might be attributed to the fact that both tested adhesives are classified as ultramild adhesives, which could not produce adequate enamel demineralization and created less retentive microporosities. 8,9 Such bonding interface might be affected by shrinkage stresses generated during resin polymerization, inducing gap formation and subsequent microleakage especially in the absence of stress-breaking nanofiller particles in adhesive composition. 30 In addition, the photopolymerization system of Estelite Flow Quick composite used to restore the cavities employs a radical amplifier to induce rapid polymerization, which may increase the rate of modulus development and, thus, shrinkage stresses. 10
In group A, fewer white clusters were detected compared to group B. This might be attributed to the presence of the functional monomer 10-methacryloyloxydecyl dihydrogen phosphate (10-MDP). It was found that this monomer is capable of forming strong and stable MDP-Ca-salt through chemical interaction with hydroxyapatite crystals (HAp). 4 In addition, it forms thick enamel acid-base resistance zone at the adhesive interface. 31 Moreover, this group of bonding contains ethanol as solvent, which forms hydrogen bond with water leading to better water evaporation upon air-drying. 4,7,31
Palfique Bond is based on the 3D-SR (phosphoric acid monomer 3D self-reinforcing monomer), which has the potential of chemical bonding to tooth structure by forming multiple point interactions with calcium. 31 However, this adhesive presented less than optimal adaptation along the cavity floor. This might be attributed to the low-vapor pressure of the solvent isopropyl alcohol. Itoh et al reported that vapor pressure of isopropyl alcohol was 44 mm Hg at 25°C, while it was 54.1 mm Hg for ethanol. 32 This denotes that more time is needed for isopropyl alcohol evaporation than ethanol. Solvent in this group might not have been totally removed, and therefore, the adhesive layer might have contained remnants of alcohol. Indeed, these residuals will retard adhesive proper polymerization and compromise the integrity of adhesive interface. 22 Interestingly, a previous study suggested a significant decrease in microleakage of Palfique Bond after increasing the drying time to 10 sec more than the manufacturer's instruction. 33 Other studies reported that failure of Palfique Bond occurs in composite-adhesive interface, as residual solvents may hamper its copolymerization with the composite. 10,22 Nevertheless, the type of failure in adhesives with average thickness of 10 μm cannot be determined by CP-OCT.
Finally, the results of present study require rejection of the proposed null hypothesis. Further study is needed to evaluate the effect of pre-etching enamel with phosphoric acid on microleakage of tested adhesives. In addition, a long-term performance assessment with artificial aging and water storage methods is required.
Conclusions and Summary
Within the limitations of this in vitro study, CP-OCT is shown to be valid and non-destructive imaging modality for detection of microleakage in dental restorations. Tetric N-Bond Universal adhesive showed better internal adaptation compared to Palfique Bond in enamel cavities.
Footnotes
Acknowledgments
This work was partially supported by the Academy of International Medical Center, Jeddah, Saudi Arabia and partly by Saudi Dental Research Group (SDR).
Author Disclosure Statement
No competing financial interests exist.