
Abstract
Introduction
A
As a result of pain, and stiffness, children with JRA are less dynamic than their peers. Decreased mobility may prompt generalized muscle weakness, diminished adaptability, reduced cardiovascular endurance, and a limited ability to exercise. 6 In this manner, neurodevelopmental approaches should be included in the treatment. 7
Joint pain and irritation trigger an endless loop that regularly results in joint harm and constant distortions. A far-reaching restoration program must begin promptly to reestablish loss of function and forestall perpetual incapacity. 8 A suitable restoration program is without a doubt as critical as starting proper and opportune medical treatment. The basic goal is to protect the practical limit and self-governance of the child. 9
Standard exercise-based recuperation modalities include alternative use of heat and/or cold, soft tissue massage, ultrasound, and electrical stimulation. 10 The available modalities are aimed to prepare the patient for exercises by relieving pain and stiffness, and reduce contractures. 10 Children with JRA were encouraged to constrain strain on arthritic joints for fear it might bother joint torment or swelling, expanding danger of injury. 11 They experience issues with endurance sports. 12 Greater submaximal energy consumptions are accounted for, recommending expanded metabolic requests for routine physical movement. 13
Recently, high-intensity laser therapy (HILT) was considered a noninvasive approach for treating musculoskeletal impairments. 14 Among the laser application modalities, pulsed neodymium-doped yttrium aluminum garnet (Nd:YAG) lasers are an alternative physical therapy modality that provides the HILT used for the treatment of arthropathy. 11,12 The utilization of HILT has been expanding, and patients have reported significant improvement in function and reduction of pain. 13,14 Studies have noted the mitigating, hostile-to-edematous, and pain-relieving impacts of Nd:YAG lasers, and researchers have advocated using such lasers with patients with pain issues. 11 –14 The recent findings proved the efficacy of HILT to reduce pain, improve the functional capacity, and gait performance in children with hemophilic arthropathy. 15 Therefore, the purpose of this trial was to assess the long-term effect of pulsed Nd:YAG lasers in the treatment of children with JRA.
Materials and Methods
Subjects
A randomized, double-blind, placebo-controlled trial was undertaken. This study was approved by the ethics committee of the Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, Saudi Arabia.
Thirty children (18 males and 12 females) with polyarticular JRA, with ages going from 8 to 12 years, took an interest in this investigation. JRA was analyzed by a pediatric rheumatologist as indicated by the American College of Rheumatology criteria for polyarticular JRA. The members were enlisted from the Maternity and Children Hospital, Makkah, Saudi Arabia. Children with JRA were included in the study if they had arthritis in five or more joints during the first 6 months of the illness, symmetry of the arthritis, and the main signs and symptoms of the affected joints included pain, swelling, and morning stiffness. Children were excluded from this study if they had severe tightness, congenital or acquired skeletal deformities, cardiopulmonary dysfunctions, and advanced radiographic changes.
Participants were randomly allocated to either an experimental group or a control group using computer-generated random numbers. The experimental group consisted of 15 children (10 boys and 5 girls) and received active HILT plus exercises (HILT+EX); the control group consisted of 15 children (8 boys and 7 girls) and received a placebo laser plus the same exercises (PL+EX) given to the experimental group. The study design was shown as a flowchart in Fig. 1. Guardians of all the children signed a consent form before participation. Children and their parents were told about the reason, strategies, and potential dangers and advantages of the investigation. This investigation was completed as per the code of ethics of the Declaration of Helsinki for experiments involving humans.
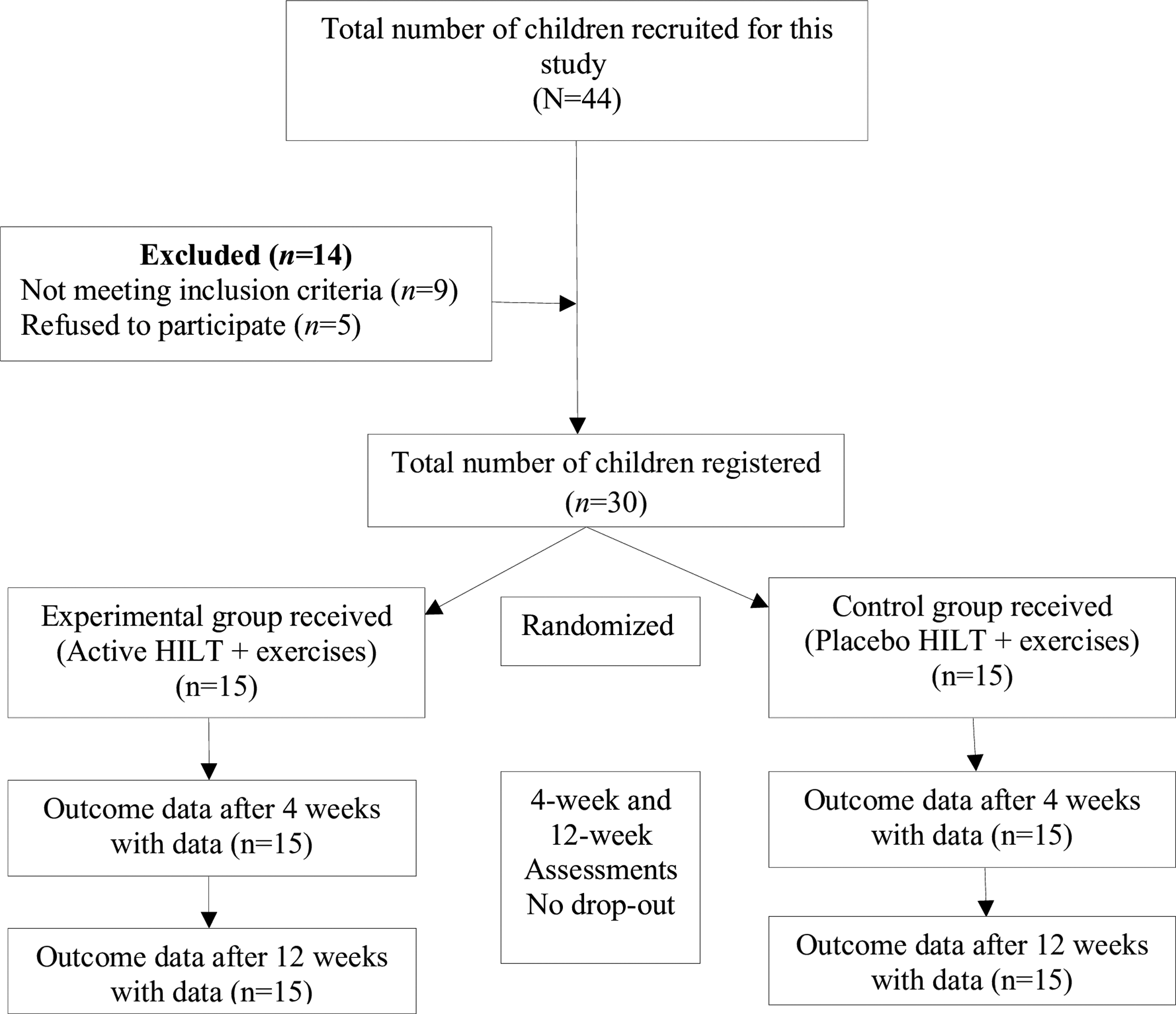
Flowchart showing the experimental design of the study.
Outcomes
Pain assessment
Assessment of the pain level was conducted using visual analog scale (VAS). 16 The VAS was an ordinal scale, utilizing a 100-mm line that reached out from no pain to the worst pain. The children were asked to assess the number comparing the pain intensity in both knee joints. Utilizing a VAS for pain evaluation is relevant in clinical trials because it is the most widely recognized and reliable type of pain scale. 17 The VAS data were gathered thrice: pretreatment (0 weeks), post-treatment following 4 weeks, and follow-up following 12 weeks.
Gait assessment
Gait parameters were estimated utilizing the GAITRite® framework (CIR Systems, Inc., Clifton, NJ). This framework comprises a 4.5-m secured electronic walkway containing 13,824 implanted weight sensors, which enroll the position and relative weight of every footfall. The GAITRite system provides a valid and reliable measurement of the spatial and temporal gait. 18 –21 In this trial, four gait parameters were chosen: stride length, step length, velocity, and cadence.
The procedures for gait evaluation at facility visits included the children walking over the walkway at their favored speed in uncovering feet. One meter of the room was given at each end of the walkway to enable the children to quicken and decelerate outside the data collection area. Every child's favored speed was utilized, rather of a constrained speed, to support the most capable walking speed for each individual. 22 Four successive steps were selected from the beginning of each walk for further analysis.
Interventions
Exercise program
The children in the PL+EX group received the placebo laser in addition to the exercise program for 1 h per session, thrice per week for 4 weeks. In the acute stage, cold packs, passive range of motion, and isometric exercises were applied. In the subacute stage, isometric and isotonic exercises were applied. In the chronic stage, hot packs, proprioceptive training, flexibility exercises (stretching of the lower limb muscles, including hip flexors, hip adductors, quadriceps, hamstrings, calf muscles, and iliotibial band), and strengthening exercises (for the hip flexors, extensors, knee flexors, extensors, ankle dorsiflexors, and plantar flexors) using weight resistance (sand bags ranging in weight from 2 to 6 kg). The children performed each strengthening exercise for three sets of 10 repetitions each. 23
Laser therapy protocol
The children in the experimental group received active HILT conveyed by a HIRO 3 device (ASA, Arcugnano, Vicenza, Italy). A pulsed Nd:YAG laser gives a wavelength (1064 nm), a high peak power (3000 W), an average power (10.5 W), fluency range (510–1780 mJ/cm2), a pulse duration less than 120 μs, a frequency range (10–30 Hz), a duty cycle of about 0.1%, a probe diameter of 0.5 cm, and a beam area of 0.2 cm2.
The laser was delivered while the child in a supine position, the knee was bent at 30° to open the joint surfaces to the laser beam. Manual scanning was performed in transverse and longitudinal directions in the anterior, medial, and lateral aspects of the knee joint. The hand piece applied the linear scanning to the joint line between the tibial and femoral epicondyles. 11,12
A total energy dose of 1500 J was delivered for both knees (750 J for each knee). Treatment was divided into three phases: initial, intermediate, and final phase. In the initial phase, fast scanning was applied with fluency set to three successive subphases of 510, 610, and 710 mJ/cm2, for a total of 300 J. In an intermediate phase, the laser was applied to fixed 10 points (Fig. 2) with a fluency of 610 mJ/cm2 and a time of 14 sec at each point, for a total of 150 J (15 J per point). The final phase was the same as the initial phase, except that slow, manual scanning was used with a total energy of 300 J. The application time for all three phases was ∼8 min. The average area of application was 60 cm2 and an energy density of scanning was 10 J/cm2. The HILT parameters used in this study are listed in Table 1. The HILT was applied day by day (three sessions per week) for four consecutive weeks (12 sessions). A pair of safety goggles should be worn during the HILT application. The HILT was calibrated for constant output throughout the study period by the manufacturer. The same visits at the same interval were arranged for children in the PL+EX group to receive exercises and the placebo laser where the HILT was the visible light beam only without any laser radiation.
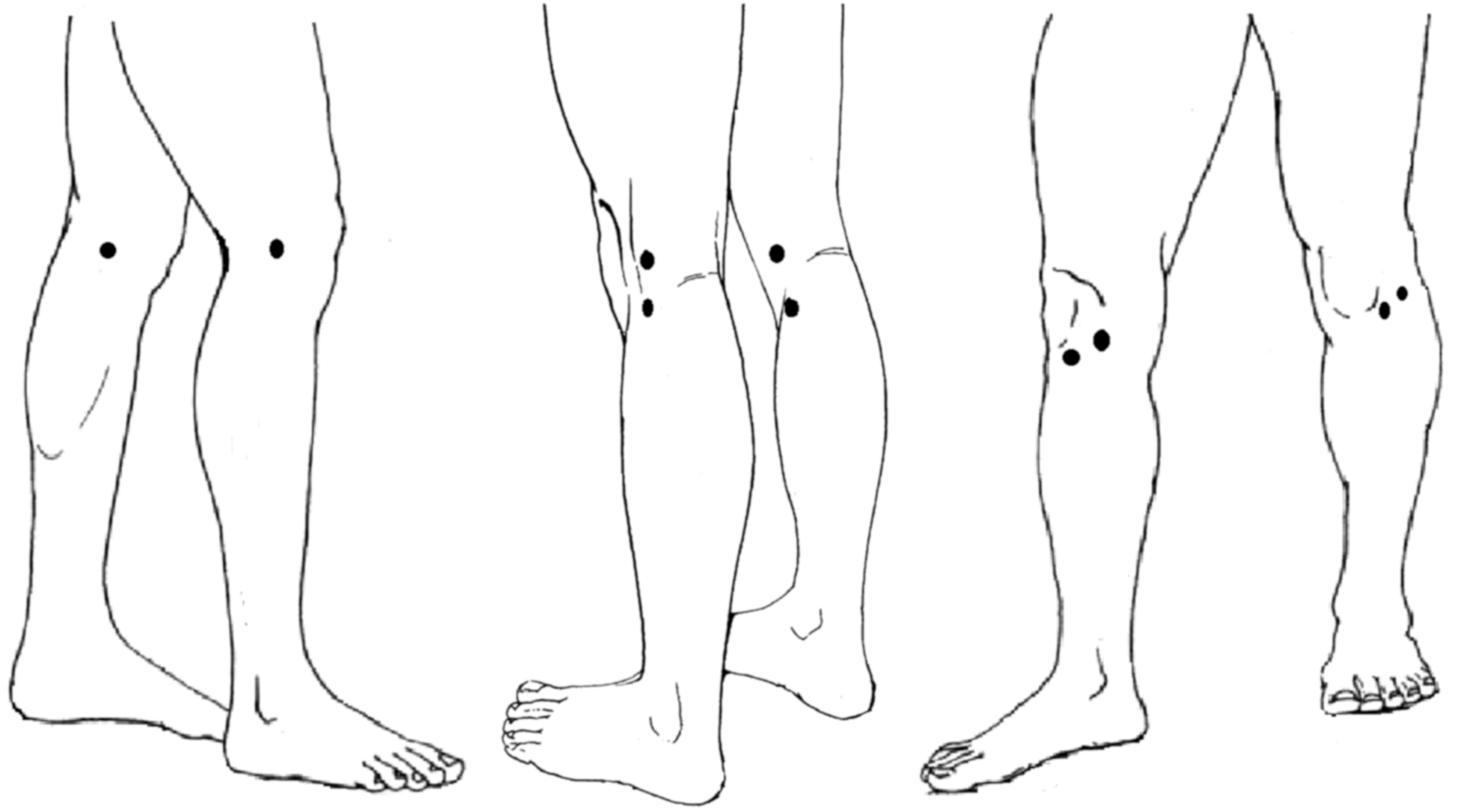
Laser points area over the anterior, medial, lateral, and posterior knee surfaces.
Data analysis
Analysis was performed using the Statistical Package for the Social Sciences (SPSS) for Windows, version 16 (SPSS, Inc., Chicago, IL), and GraphPad InStat (GraphPad Software, Inc., San Diego, CA). Unpaired t-test was used to compare the same measurement interval in both treatment groups. The repeated-measures ANOVA was used to detect the significance in the measurement intervals in each treatment group.
Results
A total of 30 patients participated in this study. Each HILT+EX and PL+EX group consisted of 15 patients. The children's mean age, weight, height, and duration of illness were 10.33 ± 1.18 years, 32.76 ± 1.83 kg, 1.35 ± 1.29 m, and 2.60 ± 0.90 years, respectively. We tested for homogeneity of variance using the two-sample Kolmogorov-Smirnov normality test, which revealed that the mean baseline values passed a normality test with a nonsignificant difference in baseline mean values (p > 0.01). Furthermore, there were no significant differences between the treatment groups in terms of their mean ages, weights, heights, and durations of illness, as listed in Table 2.
The values are in mean ± SD.
Nonsignificant difference among treatment groups (one-way ANOVA; p < 0.05).
EX, exercises; HILT, high-intensity laser therapy; p, probability value; PL, placebo laser; SD, standard deviation.
The unpaired t-test revealed nonsignificant differences between the baseline values of VAS score among the treatment groups. The VAS score as well as gait parameters showed significant differences among treatment groups after the treatment and at follow-up, as listed in Tables 3 and 4. Repeated-measured ANOVA revealed significant differences in VAS and gait parameters in both the HILT+EX and PL+EX groups after the treatment and follow-up compared with the baseline values (Tables 3 and 4).
Significant difference among the repeated measurement intervals in each treatment group (repeated-measures ANOVA; p < 0.05).
Significant difference in the same measurement interval among treatment groups (unpaired t-test; p < 0.05).
Nonsignificant difference.
Rt, right; Lt, left; p, probability value.
Significant difference in the same measurement interval among treatment groups (unpaired t-test; p < 0.05).
Significant difference among the repeated measurement intervals in each treatment group (repeated-measures ANOVA; p < 0.05).
Nonsignificant difference.
Children in the HILT+EX group exhibited a significant decrease in post-treatment VAS score and a significant increase in gait parameters compared with baseline values (Tables 3 and 4). The VAS scores significantly decreased after 4 weeks and then significantly increased after an additional 12 weeks of follow-up, although the values were still significantly lower than those at the baseline (Tables 3 and 4). Gait parameters significantly increased post-treatment, and the mean values decreased at follow-up, but failed to match the baseline values. The effect observed in the PL+EX group was similar to that seen in the HILT+EX group: VAS score decreased and gait parameters increased after 4 weeks, and these changes reversed at 12 weeks (Tables 3 and 4).
Discussion
The results of this study revealed a significant decrease in VAS scores and significant improvement in the gait parameters in both treatment groups. The combination of HILT and exercise was more effective at decreasing VAS scores and improving gait parameters than exercise alone.
Based on the available literature, no study evaluated the effects of HILT in the treatment of children with JRA. This investigation used valid outcome measures to investigate the effects of HILT in children with JRA. The results suggest that HILT may be considered an effective treatment tool for patients suffering from rheumatoid arthritis (RA), especially the juvenile type.
Studies of animals have shown that low-level laser therapy (LLLT) alters inflammation in inflammatory joint disease. 24,25 Laser radiation prevents increases in vascular permeability, which occurs in acute inflammation, 26 as well as suppresses the inflammation of the synovial membrane in RA. 25 Moreover, LLLT improves the mononuclear inflammatory cells, exudate proteins, medullary hemorrhage, hyperemia, necrosis, the distribution of fibrocartilage, and chondroblasts and osteoblasts both in the early- as well as the late-progression stages of RA. 27
Johannsen et al. reported a significant decrease in the pain score with no significant effect on sensation of morning stiffness or any motor improvement in grip strength or flexibility. 28 However, the sample size in this study was relatively small to provide more conclusive evidence. A lack of significant efficacy was also noted by Heussler et al. These authors reported 72% pain relief with no significant changes in clinical, functional, or laboratory findings. 29 Meireles et al. concluded that LLLT was not effective in treating the hands of patients with RA. 30 In these previous trials, the authors used a (Ga-Al-Ar) laser with a wavelength of either 785 or 812 nm and an energy density of 3–12 J/cm2. 29,30 The use of LLLT was effective in animals, but not in humans reflect the inadequate laser type, wavelength or energy delivered to patients with RA.
The results of this study are consistent with those of Goldman et al. 31 and Palmgren et al. 32 These authors demonstrated a significant improvement in both the metacarpophalangeal and proximal interphalangeal joints of both hands with significant increase in grip strength and finger flexibility, and significant decreases in pain, morning stiffness, and swelling of the proximal interphalangeal joints. 32 The laser yielded more significant improvement in erythema pain, swelling, and tenderness compared with the other control hand. 31
The difficulty of applying LLLT over joint surfaces and the surrounding muscles, as well as the low penetration depth of LLLT, are considered limiting factors. LLLT used a He-Ne or semiconductor laser with wavelength 632–908 nm, with class IIb or III power, which does not reach 0.5 W. Low laser power and low energy density produced allow to apply LLLT in specific points with low energy density (3 J/cm). 33
HILT is a class IV laser that provides power (3000 W) with a high-power density (150,000 W/cm2), and its elevated levels of fluency (up to 1780 mJ/cm2), which can cover a large treatment area in a short time with a wavelength of 1064 nm. This wavelength works in a therapeutic window that allows it to penetrate and spread more easily throughout tissue compared with LLLT. 17 The very short emission time and a brief duty cycle, and low frequency (10–30 Hz), can produce photochemical and photothermal effects on the target tissues without causing accumulation of heat in tissues, 34 leading to the possibility of treating deep tissues. 14
In chronic knee osteoarthritis, HILT applied 20 min daily for 10 days was effective to decrease the VAS score. 35 In another study, HILT was compared to LLLT (Ga-As, 830 nm, 800 mW). Both lasers were used to deliver 1250 J to all patients with 50 J/cm2. HILT was more effective than LLLT in decreasing VAS score and improving knee function. 12 A similar study investigated the analgesic effect of HILT in patients with chronic arthritis. The result recommended the HILT as an effective physical therapy modality to decrease pain and improve joint function. 36,37 Recently, pulsed Nd:YAG laser combined with oral glucosamine/chondroitin sulfate was effective to decrease VAS and improve knee function scores, as well as decrease the synovial thickness after 6 weeks of treatment. 11
The results of this work were consistent with those of Demartis et al. These authors investigated the efficacy of HILT in chronic hemophilic arthropathy. HILT provides a rapid pain-relieving modality that had a significant analgesic effect after 1 week of treatment. 38 El-Shamy and Abdelaal investigated the effects of HILT on pain, functional capacity, and gait in children with hemophilia. The HILT group exhibited a significant decrease in pain and an improvement in functional capacity and gait parameters compared with individuals in the placebo group. 15
It is difficult to describe the anti-inflammatory effect of HILT with a limited number of HILT studies. HILT was effective in increasing the local capillary blood flow and tissues microcirculation in patients with oligoosteoarthrosis and polyosteoarthrosis. 37,39 In addition, HILT alters the inflammatory process inside the knee joint by decreasing the synovial thickening, and subsequently decreases knee effusion. 11 Moreover, HILT preserves the connective tissue by minimizing its damage, and therefore improves the function of the affected joints. 11,39 HILT modulates the pain by working on the gate control theory and/or stimulating the regeneration of nerve fibers. 36 HILT is postulated to have photothermal and photomechanical effect, in addition to the photochemical effect. 40 –42 Although it was not measured quantitatively in the previous studies, these thermal and/or mechanical stimulations to the exposed tissue may be responsible for the reduction of pain and inducing a hemodynamic response, with its beneficial effects on edema washout and venous and lymphatic microcirculation. 11,36,37,39
Exercise therapy is considered to be an integral component of treating children with JRA. 43 Researchers have used different types of exercise (e.g., aerobics, and strengthening and stretching exercises for improving muscle strength, endurance, and motor coordination). The results of these studies showed that exercises decrease pain and disease activity, 44 and improve functional capacity, 43 walking ability, quality of life, 44 and muscle strength in patients with RA. 43 –45
Conclusions
Pulsed Nd:YAG laser combined with exercises are effective physical therapy modalities for children with JRA. Such combination has a long-lasting effect than exercise alone in decreasing pain and improving gait performance.
Limitations
Although no deficiency in doing the exercise prescription at home was reported, the exercise compliance was deemed to be a limiting factor in this study. The lack of methods for objective measuring of thermal effect of HILT, as well as the structural changes in the knee joint, may interfere with describing the exact mechanism of HILT in the treatment of RA and are considered limiting factors.
Footnotes
Acknowledgments
A special thanks to the colleagues at the Physical Therapy program, Faculty of Applied Medical Science, Umm Al-Qura University, Saudi Arabia, for their support and valuable assistance throughout the study.
Author Disclosure Statement
No competing financial interests exist.