
Abstract
Introduction
I
In addition to participating in skin injury repair, mast cells present in the skin have many biological functions. 6 Previous investigations have demonstrated that during skin injury repair, mast cells increase acute inflammation, enhance new epidermis regeneration and new blood vessel formation, and improve scarring. 6 A characteristic of mast cells is the degranulation in response to various stimuli. The process of mast cell degranulation is initiated by the influx of Ca2+. 7 Activation through IgE receptors triggers degranulation with release of inflammatory mediators, stored in abundant cytoplasmic secretory granules. This is followed by de novo synthesis and secretion of cytokines/chemokines. 8 Mast cells are very important in tissue repair and wound healing processes. Therefore, mast cells have been used in many experimental works using photobiomodulation. 8 –11
Mast cells have also been associated with aberrant healing, with a number of mast cells found in chronic wounds. 5
Many pre-clinical investigations have revealed optimistic influences of the mast cells in skin injury repair. 12 –16 Chymotrypsin and histamine in the mast cells might contribute toward skin injury repair. 8 Mast cells contribute particularly in the proliferative and remodeling steps of wound healing after a thermal damage, 13 or after a skin wound. 15 Finally, it has been recognized that wound closure requires the presence of both mast cells and fibroblasts. 16 Concerning the already mentioned studies, we hypothesized that the mast cells are the perfect cells to perform an essential role in skin injury repair and, particularly, in the remodeling step due to their location and materials released. 17
Stabilized mast cells in uninjured skin are necessary for appropriate skin injury repair and treatments, preventing mast cell degranulation that could enhance wound healing in diabetes mellitus. 3 The delayed increase of the mast cells might prevent vascular regression in the remodeling step of skin repair and damage the skin injury repair in diabetic mice. 18 Consistently, administration of propranolol enhances skin injury repair in diabetic rats by increasing the number of mast cells, decreasing the inflammatory reaction, and conducting the next steps of the repair process. 19 The administration of the biotinylated Glycyl-Histidyl-Lysyl (GHK) peptide was found to increase the synthesis of collagen, activate the fibroblasts and mast cells in diabetic rats, and hasten the repair of skin injury. 20 Nevertheless, the exact role of mast cells in diabetic skin injury repair is not clearly known. 18
In our earlier works, we found that photobiomodulation of diabetic wound with 890 nm, 80 Hz, and 0.2 J/cm2 significantly increases the tensile strength on day 15, 21 increases the macrophages, fibroblasts counts, and blood vessel sections. 22 Photobiomodulation significantly increased the total number of mast cells compared with the control type 1 diabetic rats on days 4 and 15. 23 In addition, the number of type 1 mast cells (T1MCs, stabilized) is significantly more than the degranulated mast cells for all photobiomodulation-treated mast cells compared with type 1 diabetic rats on days 4 and 15. 23
Since photobiomodulation has been established as a valuable and beneficial technique for curing skin injuries, 21 –23 it was used with stem cells and/or conditioned medium (CM) of stem cells for improving the neovascularization effect of the stem cells and accelerating the repair of skin injury in healthy and diabetic (ischemic) animal models. 24 –28 However, there is limited data on the quantity and the activation state of skin mast cells in diabetes mellitus. 3
The goal of this experiment is to examine the effect of degranulation of the mast cells and the total number of mast cells in the remodeling step of the repair of a rat model of diabetic and ischemic skin injury under the influences of photobiomodulation and human bone marrow mesenchymal stem cells CM (hBM-MSCs-CM), or CM individually, and or in combination.
Materials and Methods
Design and animals
The institutional Medical Ethics Commission of the first author approved all the procedures. Seventy-two adult male Wistar rats of 4 months of age and almost 260 g body weight were used. Rats were housed in a standard animal home and provided with standard rat pellet and water ad libitum. First, type 1 diabetes mellitus (T1DM) was induced in the entire group of rats; then after a month, one incision was made in the back of each rat. Consequently, rats were divided into four groups, harboring 18 rats each. The first group was considered as the control (placebo) group, and received vehicle of CM (Dulbecco's modified Eagle's medium). The second group received CM alone, the third group received photobiomodulation eventually, and the fourth group received photobiomodulation+CM. On days 4, 7, and 15, wound samples were extracted for histological and tensiometric examinations.
Isolation and expansion, and immunophenotyping of CM
Isolation and expansion of hBM-MSCs are reported precisely in our previous studies. 24,25 In brief, aspirated bone marrow was diluted. Mononuclear cells were isolated and cultured. Nonadherent mononuclear cells were discarded. Four cell passages were performed on attached fibroblast-like cells to detach the cells. 24,25 For immunophenotyping of cultured hBM-MSCs, briefly the MSC surface antigens were detected by incubating the samples with fluorescein isothiocyanate-conjugated mouse antihuman antibodies; cluster of differentiations (CDs) 105, 73, and 90 (FAB10971p; R&D Systems, Minneapolis, MN) were used as positive markers, and CDs 34 and 45 were used as negative markers for stem cells. Mouse Isotype antibodies (IgG1, kappa, ab18443; Abcam) were applied as negative controls.
The results were analyzed to 104 events against each antibody with a flow cytometer using WinMDI software. 24,25
Preparation of hBM-MSCs-CM
In this study, CM was prepared by culturing 106 passage-4 hBM-MSCs in a TP75-culture flask, as described in our previous works. 24,25 In brief, cells were allowed to grow until an approximate confluence of 80% was reached. CM was extracted and concentrated to about 20-fold by lyophilized drying according to the manufacturer's guidelines. 24,25
Induction of T1DM
T1DM was induced in the entire group of rats by one-time administration of streptozotocin (STZ) (40 mg/kg, I.P.). Diabetes mellitus is defined as a blood glucose concentration >250 mg/dL, 7 days after STZ injection. 29 The diabetic rats were kept for 30 days to ensure that induced diabetes mellitus was stable in rats. 21 –24
Surgery
Under general anesthesia and sterile conditions, a 12-mm full-thickness incision was made in the rat upper thoracic region with a No. 15 scalpel. The day of surgery was considered as day 0.
Photobiomodulation
The incisions in the third and fourth groups were exposed to an infrared laser (MUSTANG 2000 with LO7 pen; Technica Co., Moscow, Russia) using the following specifications: power density, 1.08 mW/cm2; wavelength, 890 nm; pulse frequency, 80 Hz; spot size, 1 cm2; pulsed duration, 180 ns; duration of exposure of each point, 200 sec; and energy density, 0.2 J/cm2.
Photobiomodulation was begun on day 0, and the surface area of the incision and the adjacent skin (Fig. 1) were subjected to 12 laser shootings, and laser pen was held vertical to the target area. Photobiomodulation was continued once daily 6 days a week for a period of 15 days. 24
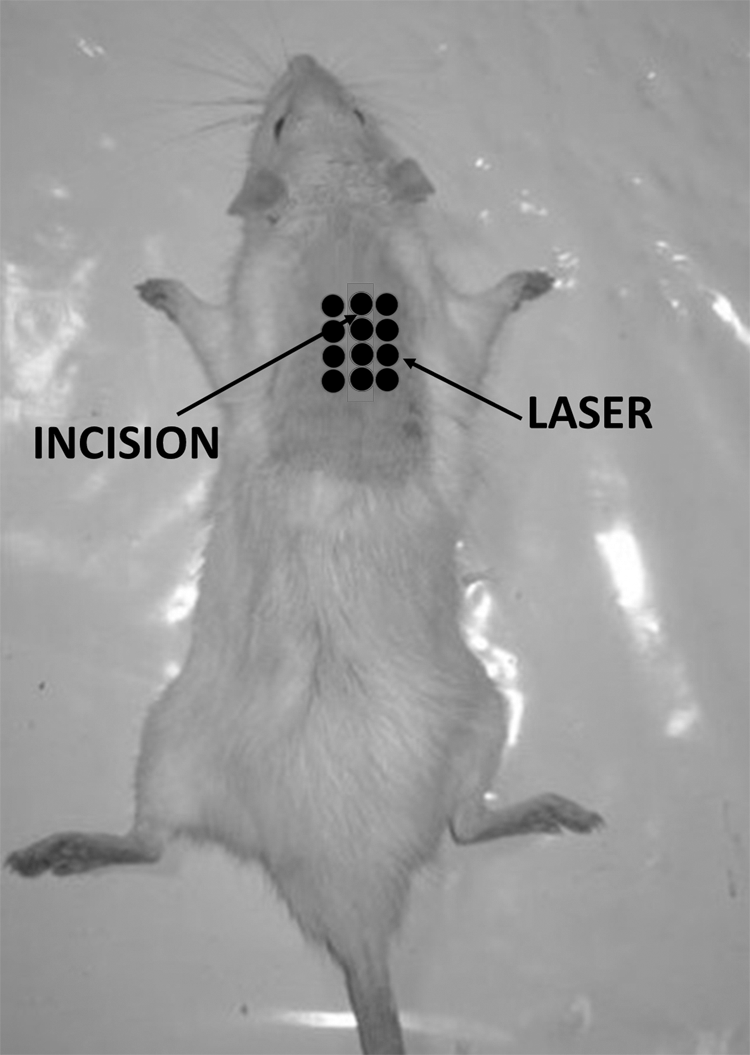
Schematic depiction of the incision and laser shooting points are shown.
CM administration
One hundred lambda of hBM-MSCs-CM were suspended in 400 λ Eagle's minimal essential medium and injected intraperitoneally in rats of groups 2 and 4 on days 0 and 1. 24
Sampling
On days 4, 7, and 15, six rats in each group were euthanized. Histological samples from wounds on the fourth and seventh days were extracted. Both histological and tensiometric samples were taken from wounds on day 15.
Clinical observations
The rats' blood glucose levels and body weights were monitored throughout the study. Eventually, the wound site was examined clinically. 24
Tensiometric examination
Tensiometric examination was performed according to our previous study. 19 In brief, one standardized rectangular skin specimen (5 × 50 mm strip) was cut from the wound bed and adjacent skin from each rat. Specimens were mounted in a material testing machine (SANTAM Engineering Design Co., Ltd., Iran). The load–deformation curve was recorded. Deformation rate was kept constant at 10 mm/min. The bending stiffness (MPa) and high stress load (N/mm2) are reported.
Stereological examination
Primarily, the samples, including wound and adjacent skin, were subjected to the light microscopy procedure, and serial sections (5 and 20 μm thicknesses) were cut using a microtome. About 10 sections of each rat were collected in a systematic random mode. The sections were stained with 1% toluidine blue.
Identifying mast cell degranulation and estimating number of mast cells
The sections were used to determine the number of mast cells and the degranulation by stereological methods using the optical dissector method. The degree of degranulation in the mast cells allowed identification of three types of mast cells by light microscopy, representing the three steps of mast cell degranulation: T1MCs (intact mast cells), T2MCs (mast cells from which several granules were released; nonetheless, the cells retained a mainly intact mast cell border, T2MCs), and T3MCs (enormous degranulation with complete or partial disintegration of the mast cell border, T3MCs) (Fig. 2). The position of microscopic fields was determined by an equal displacement of stage of microscope and systematic, uniform sampling of slides.
23,30,31
Microcator was used to measure Z-axis movement of the microscope stage. An unbiased counting frame with inclusion and exclusion borders was superimposed on the images of the sections, which is viewed on the monitor. A nucleus was counted if it was placed completely or partially within the counting frame and did not reach the exclusion line. Numerical density (Nv) was calculated using the following formula:
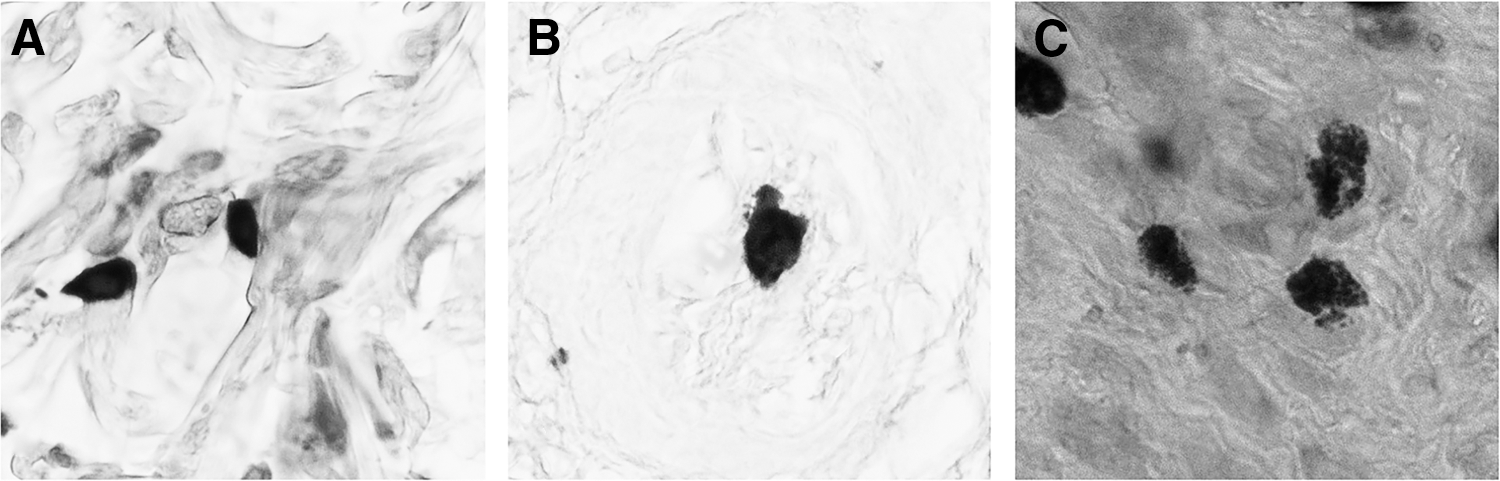
Three steps of MC degranulation in a rat skin sample. Tissue sections were stained with toluidine blue.
where “ΣQ-” is the number of the nuclei, “h” is the height of the dissector, “a/f” is the frame area, “Σp” is the total number of the unbiased counting frames in all fields, “t” is the real section thickness measured in every field using the microcator; and BA is the block advance of the microtome set at 20 μm. The total number of mast cells was estimated by multiplying the numerical density (Nv) by the total volume (V).
31
Statistical analysis
Data are expressed as mean ± standard deviation of the mean. Wilcoxon test was used for comparing body weight. For analyzing tensiometric and mast cell data, with a normal distribution, one-way analysis of variance (ANOVA) and two-way ANOVA were used. The following is a short explanation about ANOVA test:
A one-way ANOVA shows that at least the groups were different from the others. However, it does not reveal which groups were different. If a test returns a significant F-statistic, we may need to run an ad hoc [e.g., the least significant difference (LSD)] test to reveal exactly which groups had a difference in means.
A two-way ANOVA is an extension of the one-way ANOVA. With a one-way ANOVA, there is one factor: mast cells of different types (e.g., types, 1, 2, and 3). With a two-way ANOVA, there are two factors: mast cells of different types (e.g., types 1, 2, and 3) and day at some time points (e.g., days 4, 7 and 15). In other words, if an experiment has two variables, a two-way ANOVA is appropriate.
The results from a two-way ANOVA calculate a main effect (the effect of mast cells types and the effect of the day separately) and an interaction effect (mast cells and day). The main effect is similar to a one-way ANOVA: each factor's effect is considered separately. With the interaction effect, all factors are considered at the same time. Interaction effects between factors show whether the effect of the laser changes with increasing number of treatment days (day).
A p value of <0.05 was considered statistically significant.
Results
Based on the flow cytometry examination, passage-4 stem cells expressed stem cell CD markers, including CD105 (82.64%), CD90 (87.53%), and CD73 (87.38%); nevertheless, CD34 and CD45 markers were not expressed in the cells. 19
General and clinical observations
There were no exudates in the wounds of study groups. All diabetic rats developed clinical evidence of diabetes mellitus a week after STZ injection. The Wilcoxon test showed a significant decrease in body weight on the day of surgery compared with that in the beginning of our experiment (265.3 ± 40.8 vs. 240 ± 29.3 g; p = 0.000). Blood glucose level at the beginning of the experiment was 93.7 ± 11.6 mg/dL. Blood glucose level increased significantly to 388.3 ± 85.8 mg/dL at the time of tensiometric examination. Figure 3 shows photographs of wounds in the study groups on day 15.
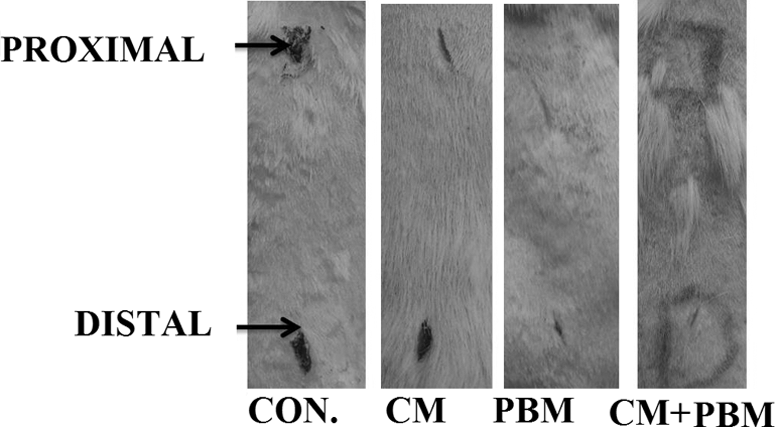
Photographs of wounds in study groups on day 15: the control group (CON), second group (CM), third group (PBM), and fourth group (CM+PBM). CM, conditioned medium; CON, control; PBM, photobiomodulation.
Tensiometric results
The results for bending stiffness and high stress load are shown in Figs. 4 and 5, respectively.
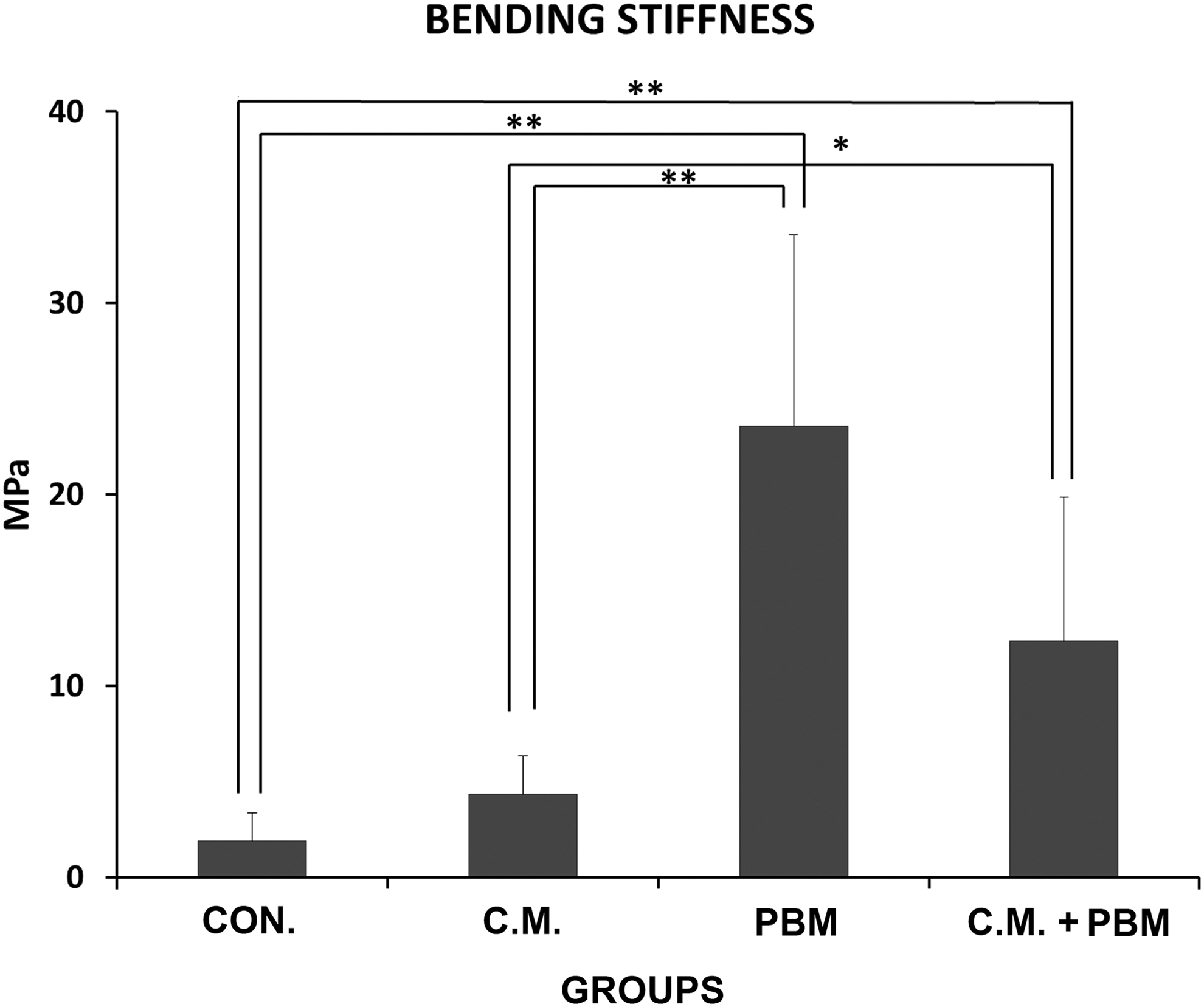
Mean ± standard deviation of bending stiffness in the study groups compared by ANOVA and LSD tests; *p < 0.05, **p < 0.01. ANOVA, analysis of variance; LSD, least significant difference.

Mean ± standard deviation of high stress load in the study groups compared by ANOVA and LSD tests. *p < 0.05.
Bending stiffness
Apparently, photobiomodulation, photobiomodulation+CM, and CM groups demonstrated a significant increase in bending stiffness compared with the control group (the least significant difference test, p = 0.004, p = 0.006, and p = 0.032, respectively). In addition, photobiomodulation-treated rats demonstrated a significant increase in bending stiffness compared with the CM and CM+photobiomodulation-treated groups (the least significant difference test, p = 0.007, p = 0.012, respectively) (Fig. 4).
High stress load
Photobiomodulation+CM, photobiomodulation, and CM groups showed a significant increase in high stress load compared with the control group (the least significant difference test, p = 0.011, p = 0.016, and p = 0.044, respectively) (Fig. 5).
Results of number of mast cells and degranulation
The results for the number of T1MCs, T2MCs, T3MCs, and the total number of mast cells on days 4, 7, and 15 are shown in Figs. 6, 7, 8, and 9, respectively.
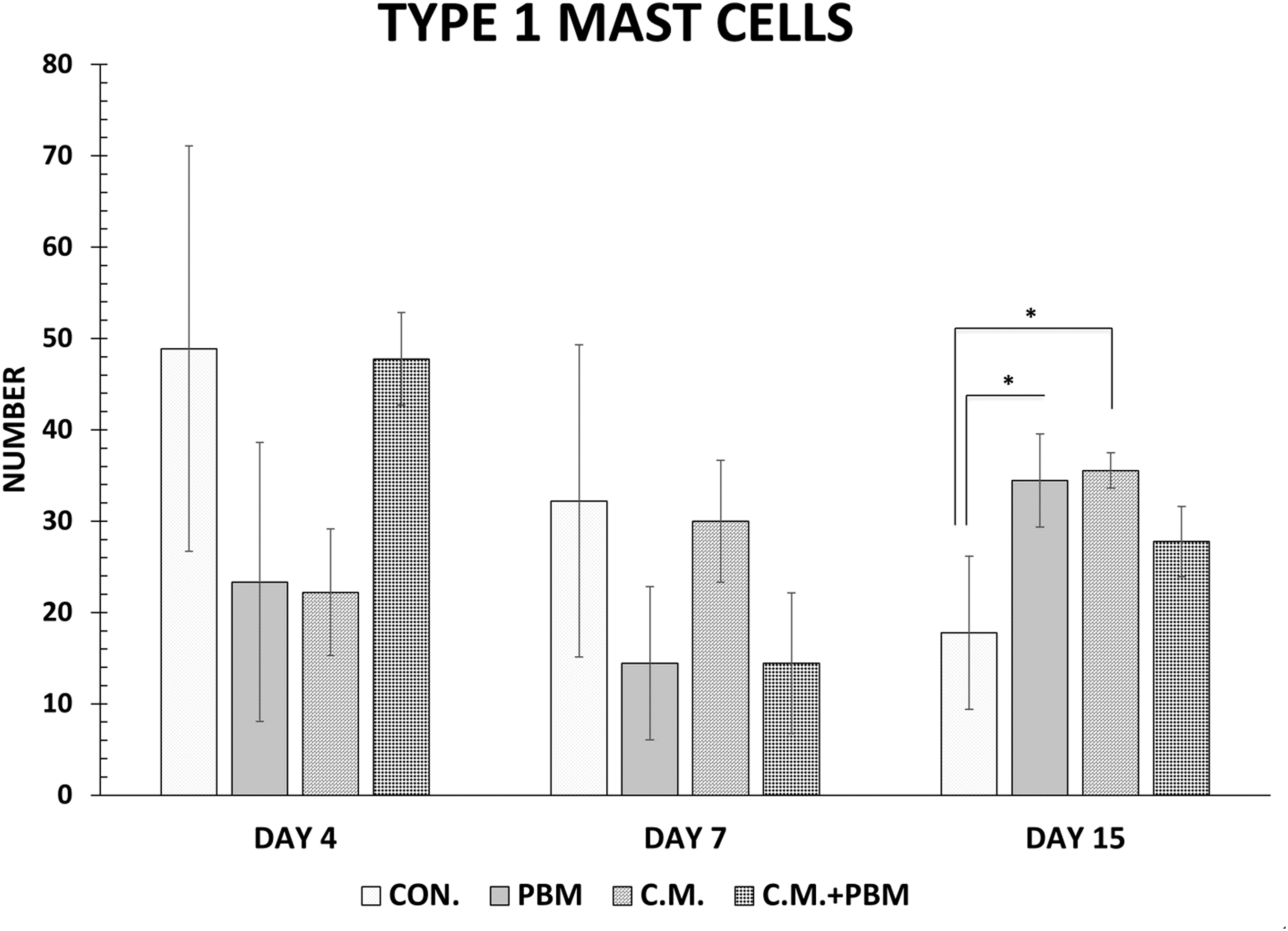
Mean ± standard deviation of number of T1MCs in the study group compared by ANOVA and LSD tests. *p < 0.05.
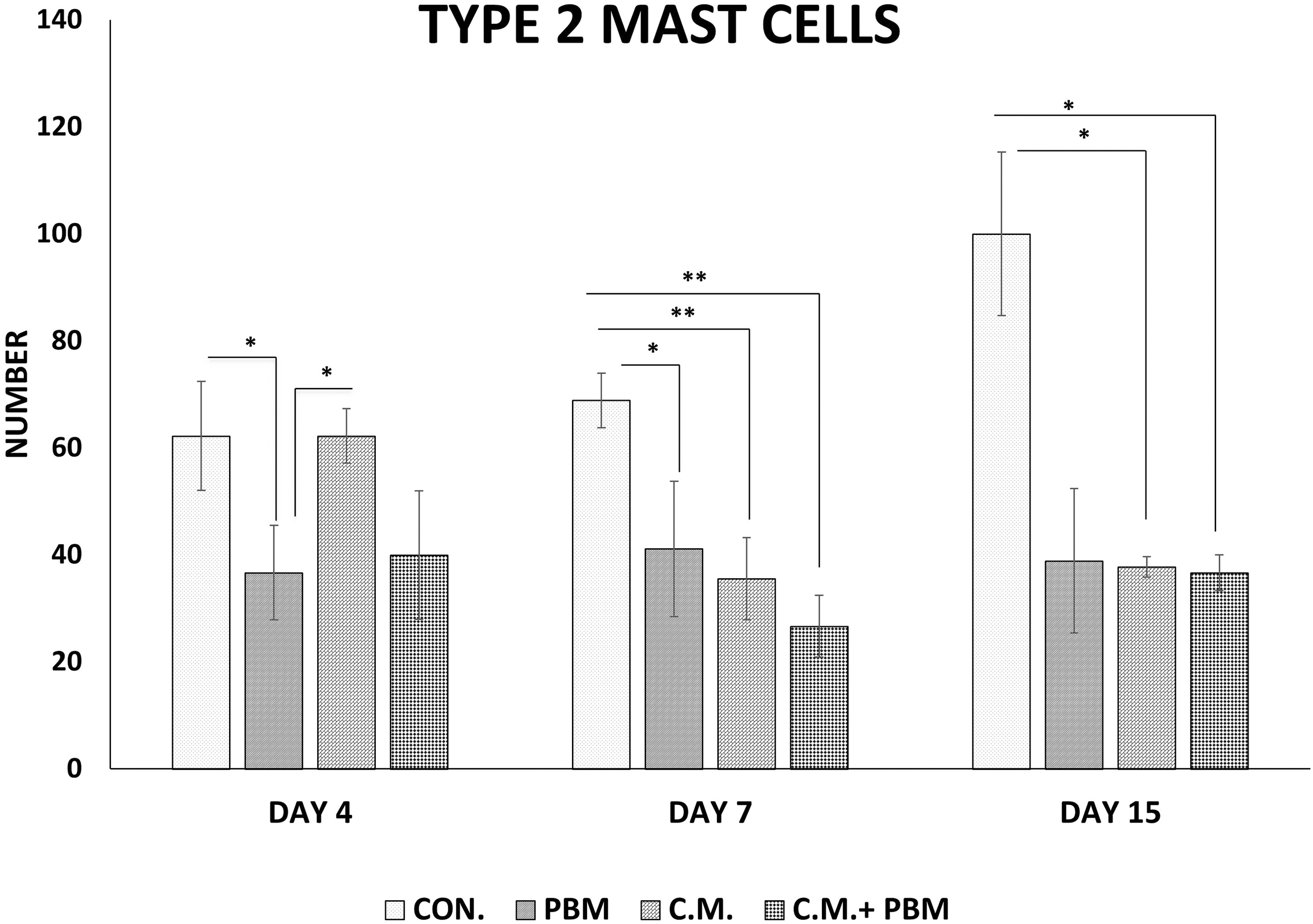
Mean ± standard deviation of number of T2MCs in the study group compared by ANOVA and LSD tests. *p < 0.05, **p < 0.01.
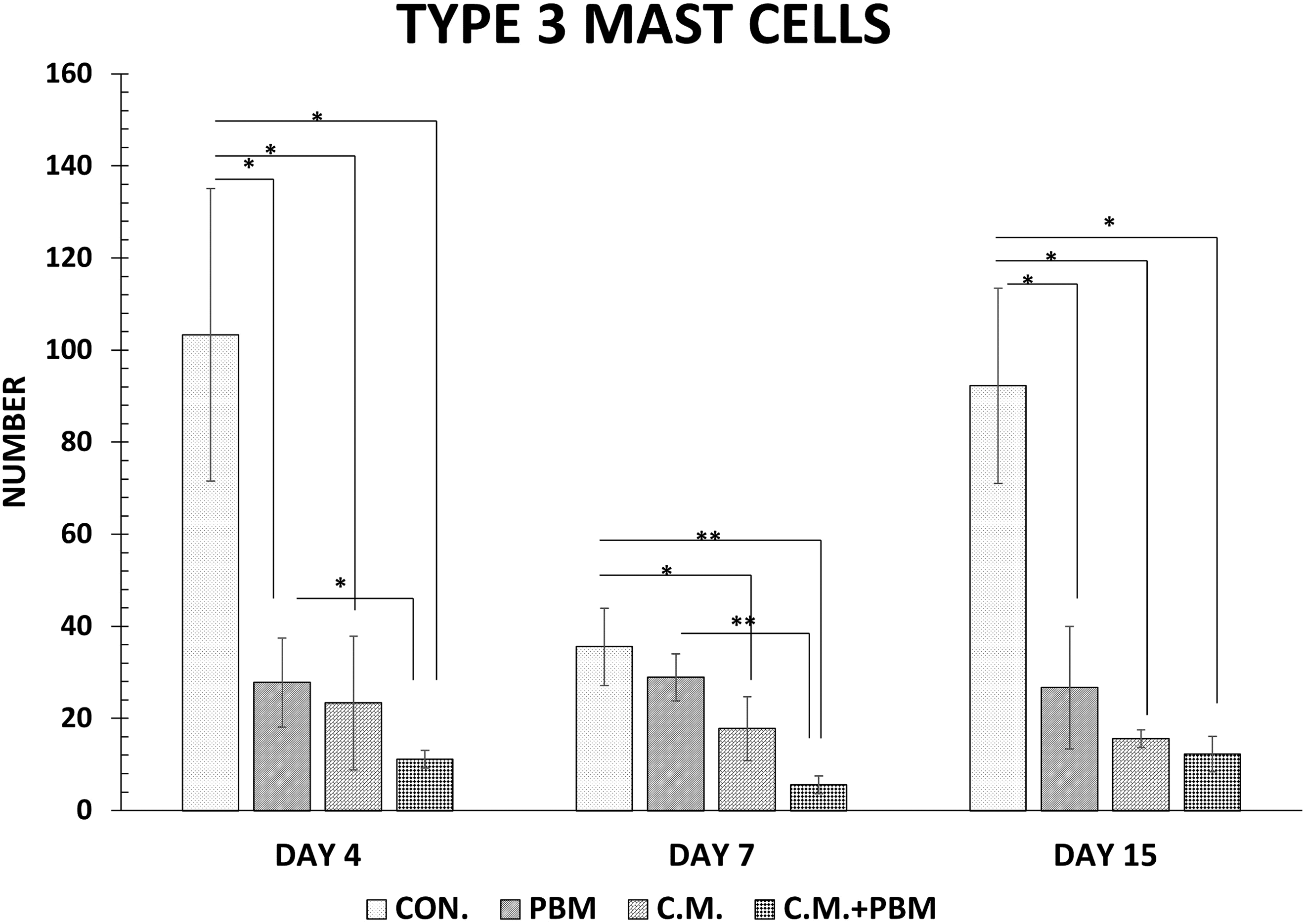
Mean ± standard deviation of number of T3MCs in the study group compared by ANOVA and LSD tests. *p < 0.05, **p < 0.01.
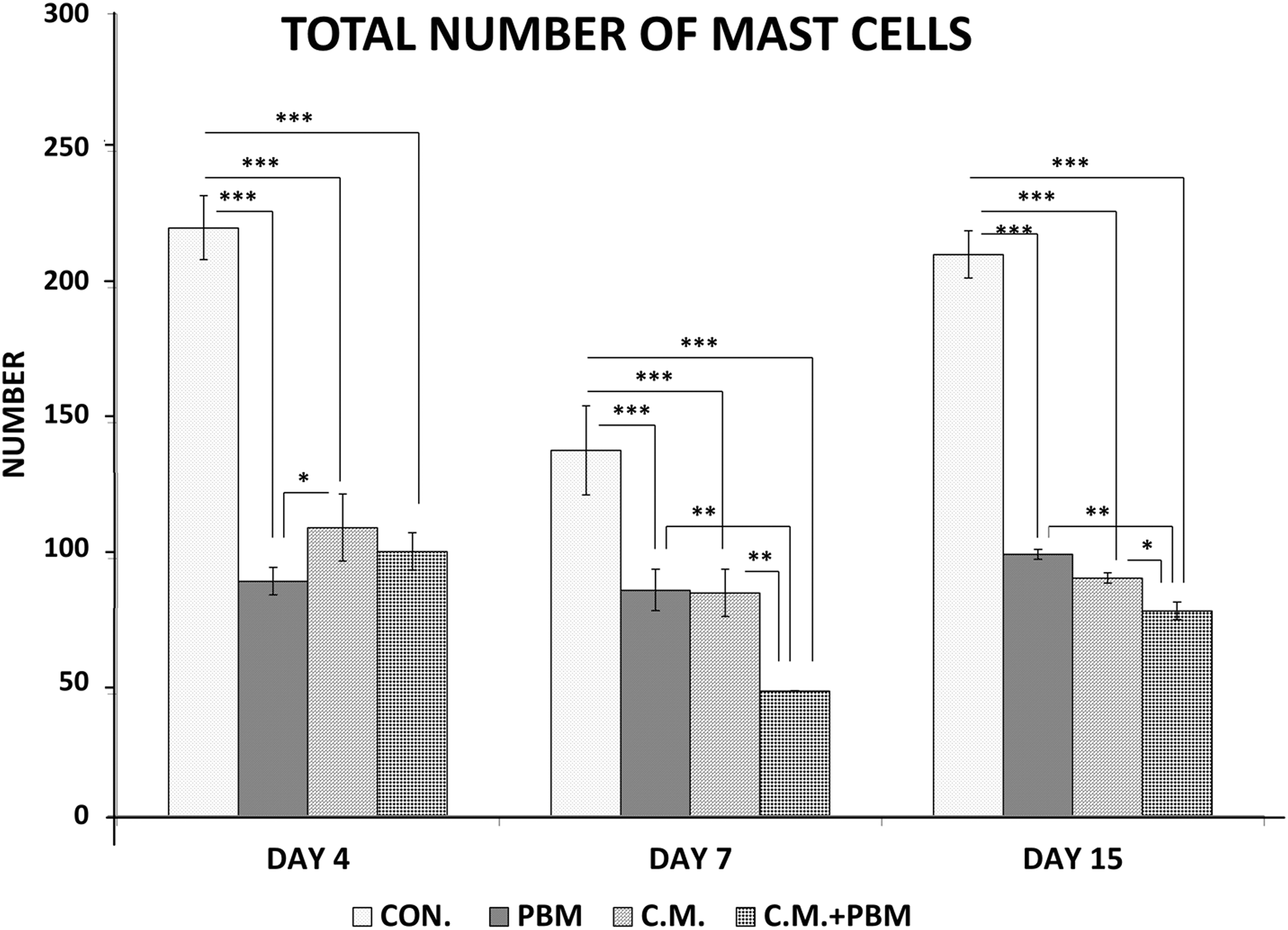
Mean ± standard deviation of total number of mast cells in the study group compared by ANOVA and LSD tests. *p < 0.05, **p < 0.01, ***p < 0.001.
T1MC–T3MC
There were significant differences in T1MCs among the study groups on day 15. CM and photobiomodulation groups showed a significant increase in T1MCs compared with the control group (the least significant difference test, p = 0.015, and p = 0.022, respectively) (Fig. 6). The photobiomodulation group showed a significant decrease in T2MCs compared with the control and CM groups on day 4 (the least significant difference test, both p = 0.041). Photobiomodulation+CM, CM, and photobiomodulation groups showed a significant decrease in T2MCs compared with the control group on day 7 (the least significant difference test, p = 0.001, 0.005, and 0.015, respectively) (Fig. 7). The control group showed a significant increase in T3MCs compared with the photobiomodulation+CM, CM, and photobiomodulation groups on day 4 (the least significant difference test, p = 0.001, p = 0.003, and p = 0.004, respectively). Photobiomodulation+CM, CM, and photobiomodulation groups showed a significant decrease in T2MCs compared with the control group on day 7 (the least significant difference test, p = 0.001, 0.005, and 0.015, respectively). CM, photobiomodulation, and CM+photobiomodulation groups revealed a significant decrease in T2MCs compared with the control group on day 15 (the least significant difference test, all p = 0.000) (Fig. 8).
Total number of mast cells
Particularly, the control group showed a significant increase in the total number of mast cells compared with the other groups on day 4 (the least significant difference test, all p = 0.000). Photobiomodulation+CM, CM, and photobiomodulation groups demonstrated a significant decrease in the total number of mast cells compared with the control group on day 7 (the least significant difference test, p = 0.000, 0.001, and p = 0.001, respectively) (Fig. 9).
Entire results of two-way ANOVA
The results for the entire two-way ANOVA showed that on day 4, the number of T2MCs was lower in the photobiomodulation groups than in the other groups. The smallest number of T3MCs belongs to the photobiomodulation group, and most of T3MCs belong to the control group.
On day 7, the number of all types of mast cells in the CM+photobiomodulation group was significantly less than that in the other groups.
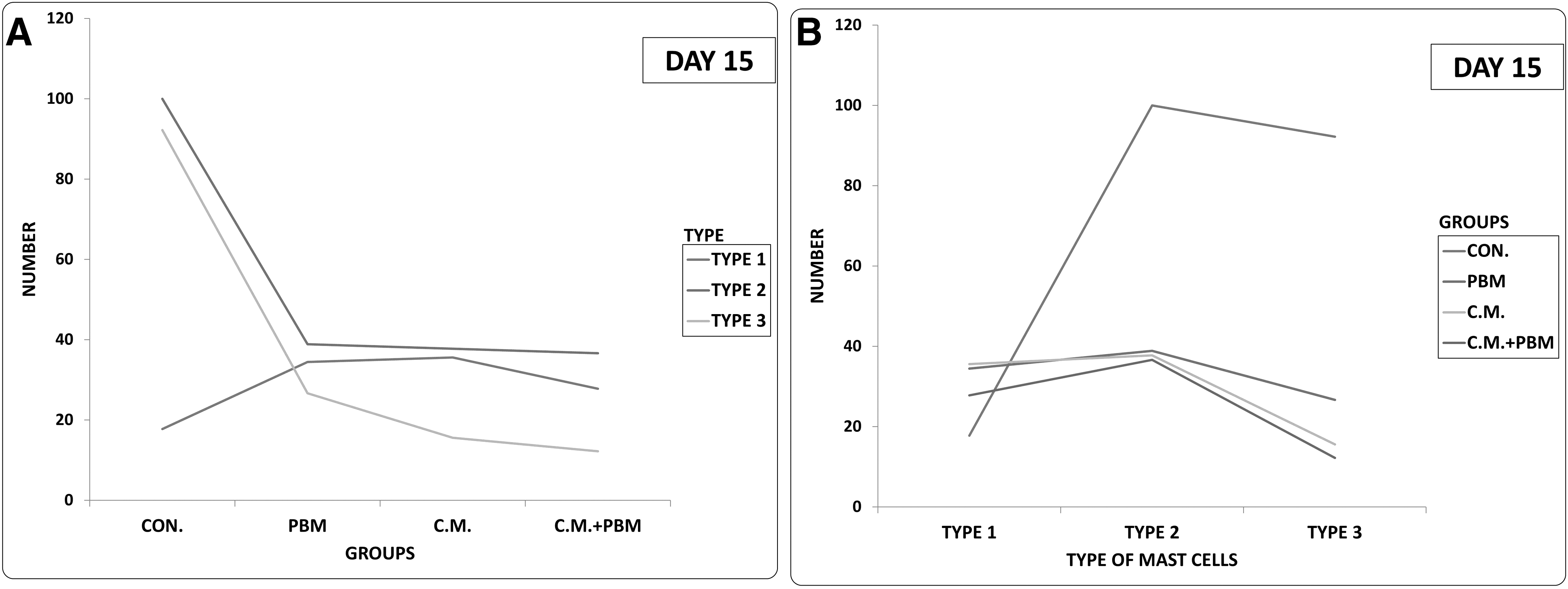
On day 15, the number of T2MCs and T3MCs in the control group was significantly higher than that in the treatment groups. In addition, the number of T1MCs was significantly lower in the control group than that in the treatment groups (Fig. 10).
Discussion
We observed a significant improvement in the tensiometric properties of wound healing in response to the treatment with photobiomodulation, CM, and photobiomodulation+CM. Here, photobiomodulation was statistically more effective than the CM. Histologically, the photobiomodulation+CM, CM, and photobiomodulation groups showed a significant decrease in three types of mast cells and in the total number of mast cells on day 15 compared with the control group. The results of the two-way ANOVA showed that on day 15, the number of T2MCs and T3MCs in the control group is significantly higher than that in all the treatment groups. In addition, the number of T1MCs was significantly lower than that in the treatment groups. We hypothesized that an interaction occurred between the degranulated and total number of mast cells and the tensiometric properties in the ischemic repairing tissue of the treatment groups.
The infiltration and proliferation of the mast cells are required for the secretion of certain toxic molecules, such as histamine and tumor necrosis factor-α (TNF-α). 32 In addition, the mast cells degranulate and discharge histamine and TNF-α. Recent studies have suggested that the mast cells participate in both T1DM and T2DM. 33,34 The population of the mast cells was altered during the remodeling step in the skin injury repair in STZ-induced diabetes mellitus in mice. 18
The mast cells produce TNF-α, which is involved in skin wound healing. 35 Although inflammation is vital for the enhancement of the proliferative step, extreme inflammation hinders skin injury repair. 4 Concerning TNF-α application to injuries, two important studies have to be considered. In the first one, treatment with four times of 200 ng TNF-α inhibited skin injury repair in rats. 36 In the second investigation, after four times of daily administration of TNF-α, a preventative influence on the wound bed was reported. Collagen formation was significantly lower in the TNF-α-treated rats than in the control groups. 37
We observed significantly lower tensiometric properties of the remodeling step in the control group than in the rats treated with photobiomodulation+CM, photobiomodulation, and CM. At the same time, the total number of mast cells and degranulated number of mast cells were significantly higher in the control group than in the photobiomodulation+CM, photobiomodulation, and CM groups. The administration of the treatments after surgery significantly improved the tensiometric properties and decreased the total and degranulated number of mast cells in response to diabetes mellitus. The results of the photobiomodulation+CM group were statistically more effective than the other treatment groups regarding the tensiometric evaluation. The protective effect of photobiomodulation+CM on increasing the tensiometric properties of repairing wounds might, therefore, relate to the decrease in the total and degranulated number of mast cells within the repairing wounds. Based on our results and the data compiled by other investigators, we hypothesized that the degranulated mast cells in an ischemic environment might release certain molecules such as TNF-α that decrease the volume of granulation tissue and the hydroxyproline content in the proliferation step of wound healing. 36,37 Consequently, those degranulated mast cells in the remodeling step of wound healing decrease the tensiometric properties of the repairing tissue.
Our data show that photobiomodulation and CM application alone significantly induced more T1MCs than the control group. This is in accordance with the two previous studies. 3,38 Tellechea et al. showed that pretreatment with the mast cell stabilizer (disodium cromoglycate) recovers diabetes mellitus-accompanied skin injury repair deficiency in mice and shifts the macrophages to the regenerative M2 phenotype. 3 Liu et al. reported that a mast cells stabilizer (Cromolyn) not only inhibited high-fat diet-induced diabetes mellitus in mice but also had a therapeutic effect. 38 Consistent with this, Zhang and Shi in their review article stated that mast cell stabilization and inactivation are an effective way to treat inflammatory illnesses in pre-clinical models, and the outcomes of mast cells stabilization suggest new healing potential for patients who suffer from diabetes mellitus. 39
We could not analyze the contents of mast cell granules in this study. This is considered as a limitation of the current work.
Conclusions
It was shown that photobiomodulation, and CM, alone and/or in combination, significantly accelerated the healing process in rat with a diabetic and ischemic wound; furthermore, the total number of mast cells and their degranulation significantly decreased. We suggest that the increased number of T2MCs in the control group adversely affected the tensiometric properties of wounds in this group. Future molecular studies are warranted to clarify the detailed interaction between mast cell degranulation and skin injury repair during the remodeling step, and content analysis of mast cell granules to distinguish the probable reasons that delay the process of wound healing in skin injury in diabetes mellitus.
Footnotes
Acknowledgments
We extend our appreciation for financial support (grant no. 5137) to Vice Chancellor of Research at Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Author Disclosure Statement
No competing financial interests exist.