
Abstract
Introduction
D
The most common chronic complications of DM are nephropathy, retinopathy, ischemic heart disease, and cerebrovascular disease. 4 Diabetic foot is defined as a neuropathic or ischemic complication that causes biomechanical alterations present on the distal extremity, frequent on toes, on the lateral faces of the interdigital compression zones, and the lateral edges of the feet. 5,6 When the lesions are not perceived due to the loss of tactile and pain sensitivity, these can evolve to an infection and consequently nontraumatic amputation. 6,7
It is estimated that 7–20% of the patients will be directed to amputation, despite being submitted to conventional wound treatment, which contemplates debridement, humid dressing, and infection control. 7 The treatment for diabetic wounds must be effective to avoid chronic lesion and its complications, stimulating the search for new treatment protocols of wounds to avoid chronic ulceration and amputation. 7,8
In this context, tissue repair process has been the focus of several studies searching for therapeutic treatments that increase the tissue's healing speed. One approach that stands out in the treatment of these lesions is low-power light therapy, such as low-level laser therapy (LLLT) and low-intensity light-emitted diode (LED) therapy. 9 Using LLLT provides analgesic and biostimulant effects, benefitting the acceleration of tissue repair. 10 LLLT use has expanded to include different treatment conditions, such as neurological processes, soft tissue lesion and musculoskeletal lesions, and dental and dermatological diseases. 10,11
Studies prove that LLLT has been applied to wound treatment, as it is effective in reducing edema and hyperemia in the inflammatory process, besides inducing the proliferation of epithelial cells, osteoblasts, and fibroblasts, favoring the synthesis of collagen. 11 –13 In light of this, LLLT irradiation is used in different wavelength and energy density parameters, being useful in different studies to accelerate the tissue repair process altered by DM. 12,13
Therefore, the present study aims at analyzing the effectiveness of the therapeutic use of LLLT in the tissue repair process of chronic wounds in patients with diabetic feet.
Methods
This randomized clinical trial, with a prospective experimental method of qualitative and quantitative nature, was approved by the Research Ethics Committee of Universidade Federal do Piauí (UFPI/CAFS/CAAE No. 67985917.80000.5660). The study was carried out in the reference center specialized in treating diabetic feet located at Ambulatório Municipal Lineu Araújo in Teresina-PI, from October 2016 to March 2017.
Initially, the participants had their wounds inspected and measured with adhesive rulers to assess the area in length and width. The evaluations of the lesions were registered on a form elaborated according to the clinical intervention tool TIME to select the sample for the study. The clinical intervention tool TIME is an assessment tool to choose the proper conduct according to the characteristics of the lesions. Each letter of the word TIME has a meaning T—nonviable tissue, I—infection/inflammation, M—unbalanced moisture, E—nonadvancing edge or dead tissue presence. The inspected wounds that presented all characteristics on the TIME tool were not sampled.
The eligibility criteria were: individuals 30–59 years of age, with chronic wounds on their feet; carriers of DM with postprandial capillary blood glucose ranging between 140 and 350 mg/dL; noninfected lesion with II and III depth staging degree, 7 cm maximum length and 3 cm maximum width and a minimum of 0.5 cm2, not higher than 21 cm2; and wounds presenting a tissue in granulation stage and little exudate.
The study was carried out with 18 volunteer patients who were randomly allotted into 2 groups of equal number (n = 9/group): Control and Laser. According to standard therapeutic protocol, lesions in Control Group were treated with physiological solution (PS) 0.9%, to clean the wound bed, applying hydrogel 2 mg (DuoDERM Gel©) on the lesion bed, using gauze and bandages as secondary cover, done every 48 h. The lesions in Laser Group were also treated with PS 0.9% to clean the bed of the wound, with LLLT irradiation and finally applying hydrogel 2 mg (DuoDERM Gel), using gauze and bandages as secondary cover, done every 48 h, as well.
Hydrogel is the primary cover used in a conventional way at health services where there are ambulatories for treating wounds, which is why this product was used on the wounds of volunteers in both groups. It keeps the area humid and promotes autolytic debridement. 3,14
In this study, an LLLT equipment (Indústria Brasileira de Equipamentos Médicos—Ibramed) with a wavelength of 660 nm, 30 mW power, and dosage of 6 J/cm2 was used. During the application, the pen remained at a perpendicular position to the edge of the lesion, in a punctual mode with contact, the tip of the pen protected by a PVC film, distance of 1 cm between dots, continuous wave, and visible red spectrum beam. Both therapist and the patient wore protective laser eyewear. The changing of the coverings and the LLLT irradiation sessions were done every 48 h, totalizing 16 sessions in 4 weeks. The characteristics of the equipment and the irradiation parameters are described on Table 1.
Weekly, the PUSH (Pressure Ulcer Scale for Healing) and the VAS (Visual Analog Scale) scales were applied to the volunteers of every group. The PUSH scale was used to monitor the tissue repair process and it takes into account three parameters to assess the intervention results: area of the wound, exudate quantity, and appearance of the bed of the wound. The sum of subscore parameters, or the subscales, generates a total score, for which the possible variation is 0–17. Higher scores indicate worse ulcer conditions and lower scores indicate an improvement in the healing process of the wound. Therefore, measuring only three variables, the PUSH instruments generate scores that, according to their magnitude and direction, can describe the condition and the evolution of the wounds. 15
VAS is constituted of a unidimensional scale to assess pain intensity. The instrument presents a 10 cm line with numeric extremities (0 or 10), so the (0) extremity means an absence of pain and the (10) one unbearable pain. 16
To obtain the length and width measurements, a 10 cm adhesive ruler was used near the bed of the wound. The images of the wounds were captured weekly, using the digital camera Sony 4.1, with flash on, even under natural light, observing a 20 cm distance (lesion–camera), with standard zoom and angle. Besides using the PUSH scale, the wounds were analyzed through the ImageJ© software, having as reference the circumference of the edges of the wound, to measure in square centimeters (cm2), calculating thus the total area of the wound.
The data were analyzed according to their distribution through the Kolmogorov–Smirnov test, which showed a p < 0.05, evidencing a different distribution of the normality curve. Therefore, the nonparametric Mann–Whitney U test was used to compare groups, considering values of p ≤ 0.05 as statistically significant differences.
Results
Eighteen patients were included in the study. The anthropometric characteristics, such as age, body mass index (BMI), and postprandial glycemic values, are presented in Table 2, as well as clinical characteristics, such as lesion time, initial and final area, depth, and healing index of the wound.
Mann–Whitney U test.
BMI, body mass index; PUSH, Pressure Ulcer Scale for Healing; SD, standard deviation; VAS, Visual Analog Scale.
There were no significant differences in age and BMI between the groups. All the patients in the study were hyperglycemic with blood postprandial glucose levels >140 mg/dL with 2 h after a meal, according to the criteria set by the World Health Organization. There was no statistical difference for hyperglycemia between groups (p > 0.931) (Table 2).
All the patients had chronic wounds in the beginning of the treatment. The lesion time in the Control Group varied from 4 to 48 months and Laser Group from 2 to 24 months. There was no statistical difference regarding lesion time and initial area between the groups. However, there was significant difference in the final area (p < 0.031) (Table 2).
The Laser Group presented a significant increase in the tissue repair index compared with the Control Group, with a significant statistical difference (p < 0.013) (Table 2).
In relation to the application of the PUSH scale to follow the evolution of the wounds in both groups, there was a significant difference along the weeks. On the other hand, in the application of the VAS for the pain there was no difference between the groups (Table 2).
Tissue repair in Control and Laser groups
Measurements through the ImageJ software, showed a reduction of the final area in both groups. The average for Control Group was 1.63 cm2 and Laser Group was 0.32 cm2, which showed a significant difference (p < 0.031). In relation to the initial depth between the groups, there was no significant difference (p > 0.297). In Laser Group patients, we observed an effective response in treating ulcers on a diabetic foot in a short period, with a visible formation of epithelial tissue in 55.5% (n = 5) of the wounds in a 4-week period (Fig. 1).
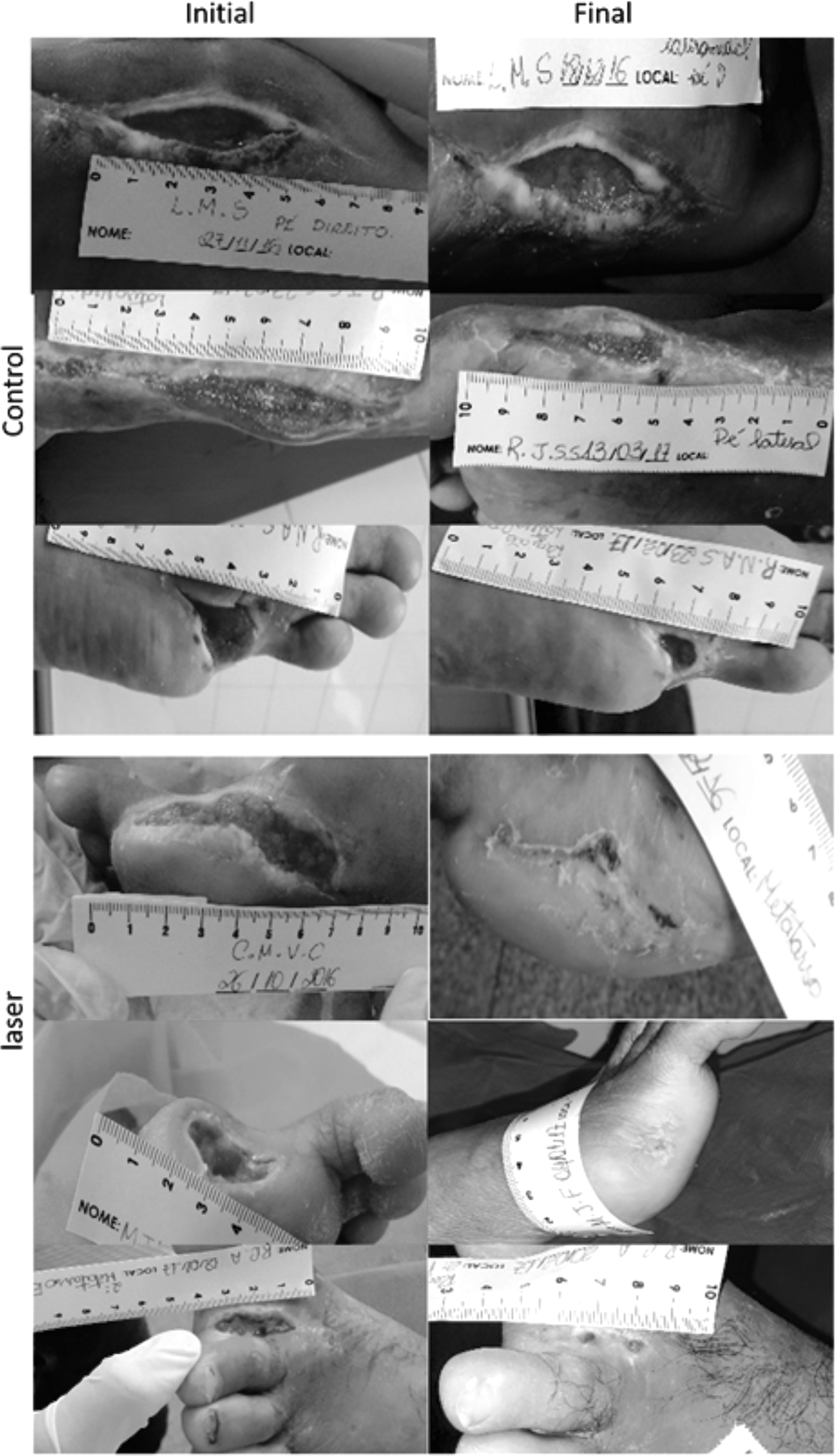
Image records of Control and Laser Groups, which evidences the measurement procedure of the initial and final areas (after 4 weeks) of ulcers on a diabetic foot.
Tissue repair in Control Group and Laser Group
The results indicate a difference in the healing level between Control and Laser Groups. Control Group presented a good response in repairing ulcer tissue, but conventional treatment was not able to achieve the expected result in a 4-week period. Laser group had an excellent response in the tissue repair process, despite all patients being hyperglycemic, with significant difference (p < 0.013) when compared with Control (Fig. 2).

Wound healing index graph in Control and Laser Groups, assessed by measuring the initial and final area. Mann–Whitney U test, p ≤ 0.05.
Ulcer weekly evolution on a diabetic foot using the PUSH scale
When comparing Control and Laser Groups, there was a significant difference in the 4 weeks of the study. We observed along the weeks that the intragroup difference increased, and in the 4th week, the difference was statistically significant (p < 0.0004) in the evolution of wounds according to the PUSH scale (Fig. 3).
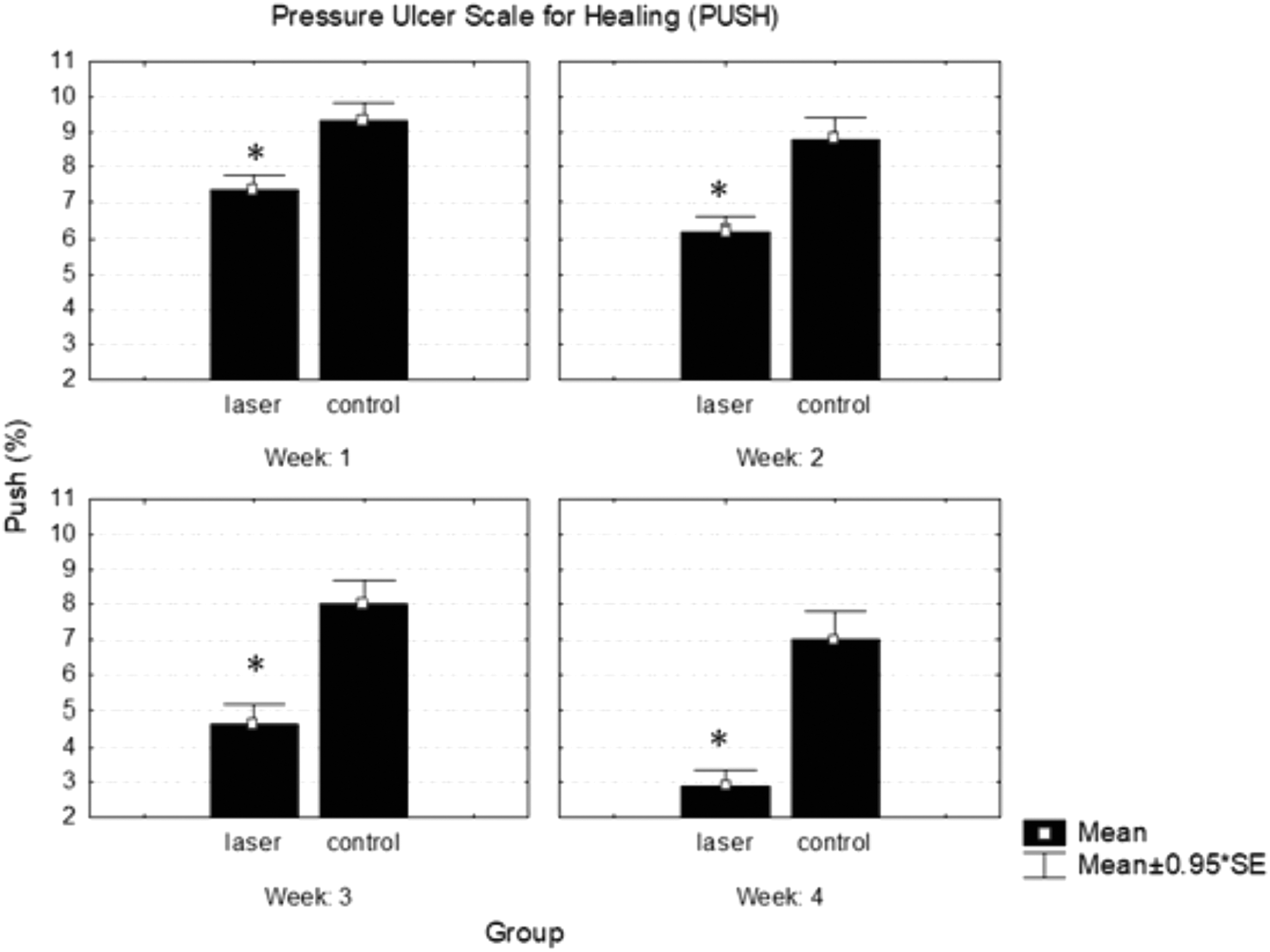
Graph showing the weekly measurement of wounds according to the PUSH scale. Intragroup comparison of patients in Control Group versus Laser Group. Mann–Whitney U test, p ≤ 0.05. PUSH, Pressure Ulcer Scale for Healing. *p = 0.01359.
Evaluation of the pain according to the application of the VAS for Pain
The results obtained with weekly applications of VAS in patients of both studied groups, Control and Laser, showed no significant difference regarding this parameter, considering that the p-value was not significant (p > 0.05) over all the weeks of the study (Fig. 4).
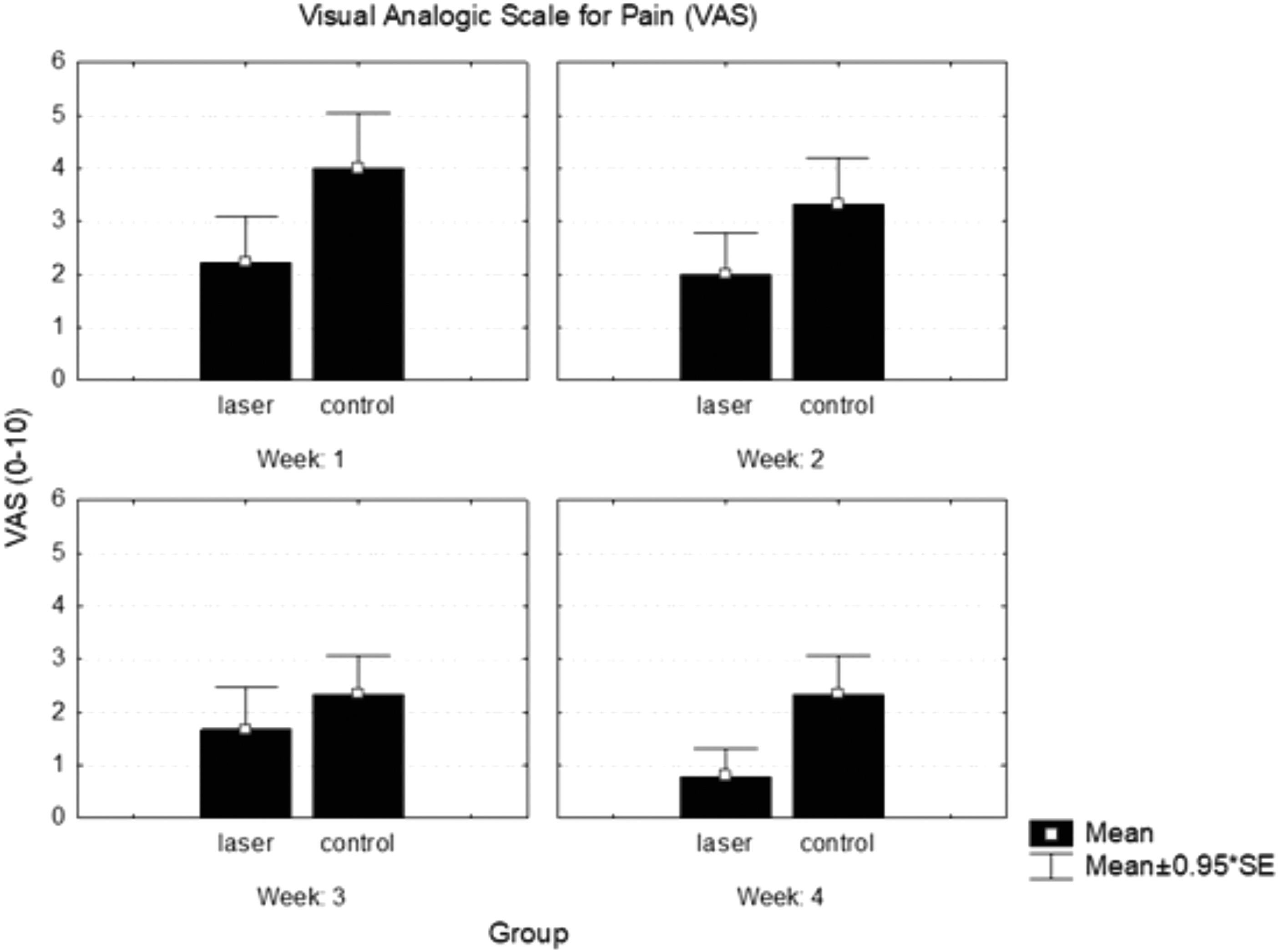
Intragroup comparison graph of patients in Control Group versus Laser Group, regarding the index pain measure by the VAS. VAS, Visual Analog Scale.
Discussion
From the groups analyzed in this study, Control Group needed more time for the tissue repair process by applying the conventional treatment used at Sistema Único de Saúde. We observed the presence of hard-to-debride hyperkeratosis and excessive dryness of the area, besides the presence of edge maceration due to humidity caused by hydrogel. On the other hand, we could observe an effective ulcer treatment response with the protocol used in applying LLLT (6 J/cm2, 48/48 h) on patients in Laser Group in a short period, in which the formation of epithelial tissue in more than 50% of the studied cases was visible.
In the present study, it was possible to verify a reduction in the inflammatory process after applying LLLT on the lesion, as well as, macroscopically, the proliferation of granulation tissue, an improvement on the hydration of the diabetic foot that is usually resected due to the diabetic neuropathy. In some cases, there was a mechanical debridement of devitalized edges that interfere on the healing process. It was also noted that the use of LLLT on the edges with keratosis made the areas more hydrated and softened, facilitating their debridement.
A study carried out in a network of public hospitals in Porto Alegre with 467 patients has attested that 95.7% of the amputation cases occurred due to clinical health problems, 50% of which were related to DM. Still, 33.8% and 33.4% of the cases occurred around the thigh and pododactiles, respectively. 17 All amputations observed for the patients of this study occurred around the pododactyl, most of them in the metatarsal region.
A study done by using aluminium gallium indium phosphide laser (InGaAIP; 660 nm, 3 and 6 J/cm2) in the healing process of wounds in the dorsal cervical areas of healthy rats showed an increase in the number of blood vessels on the 5th day after irradiation and contractions of the skin edges after the 10th day of the treated groups. The authors related that neovascularization is directly related to the action of LLLT on skin wounds and that in this same period they could notice a reduction of the inflammatory process and the production of growth factors. 18
In all the diabetic ulcers evaluated after applying LLLT (660 nm, 6 J/cm2) in this study, we could observe macroscopically that starting in the first session there was an improvement in the aspect of the edges of the wound and a minor increase of the granulation tissue. In the second session, we could notice a contraction of the edges of the lesion, besides a humidity increase in the bed and on the edges of the wound. From the third session on, we could observe a rapid proliferation of the granulation tissue, skin epithelialization, and the edges became viable, that is, without maceration, keratosis, and devitalized tissue for tissue repair. Moreover, a significant reduction of hyperkeratosis was evident, common to the diabetic foot, probably associated to LLLT, which contributed to the acceleration of diabetic ulcer healing.
A study done with diabetic rats treated with LLLT (660 nm, 100 mW continuous power, and 4 J/cm2 dosimetry for 24 sec) suggested the phototherapy capacity to influence the percentage of neoformed collagen on cutaneous wounds in the dorsal region, with an increase of the collagen fibers. 11
Other studies evidenced that LLLT increases mitochondrial respirations and the adenosine triphosphate (ATP) levels in cells from isolated cultures. The laser stimulus conducts the calcium exchange through the cellular membrane, causing transitory alterations in the cytoplasmic calcium level and it helps to synthesize regulating proteins. These modifications contribute to stimulate cellular proliferation, beneficial for the reestablishment of conjunctive tissue during tissue repair and wound healing. 19
From the sixth session, we could observe that patients reported pain and the return of peripheral sensitivity, which was lost along the years due to diabetic neuropathy. During the weekly applications of the VAS, there was no difference regarding pain between Laser and Control groups related to diabetic neuropathy. Diabetic neuropathy is a kind of damage to the systemic peripheral nervous system due to chronic hyperglycemia and other physiopathological alterations induced by DM. 20
When comparing Laser and Control groups in this study, there was a significant difference in all the weeks in the PUSH scale levels. This scale is a quick and trustable tool to monitor wound healing. 21 In a study performed in the Ambulatory Plastic Surgery at Hospital de São Paulo, it was observed, through the PUSH scale, an evolution of the wound, such as the reduction in length and width of the lesion, exudate decrease, and tissue improvement. 3
The tissue repair process for the patient with a diabetic foot is extremely important to improve their self-image and restore normal life. In addition, nontraumatic amputations need to be avoided, as they compromise the quality of life of these individuals, not to mention the high financial impact by increasing costs with possible hospital admissions, material, and disability remuneration. 4,5
Conclusions
Using LLLT has proven to be effective in reducing the necessary time for the tissue repair process in ulcers on a diabetic foot in a short period. Furthermore, LLLT has allowed the return of pain and tactile sensitivity in some patients who had lost the sensitivity in their feet completely. We suggest new research on the use of laser to restore the sensitivity of patients with a diabetic foot. The use of the PUSH scale was useful and effective to monitor the wounds, since its scores evaluate the area measurement, exudate level, and lesion tissue type. Due to diabetic neuropathy, the VAS pain scale was not effective.
Footnotes
Author Disclosure Statement
No competing financial interests exist.