
Abstract
Background:
To obtain the best result from flexor tendon repair surgery, proper surgical technique, appropriate materials, good rehabilitation, and patient satisfaction are essential to consider. Nevertheless, no general unique protocol still exists between researchers, for a suitable treatment plan.
Objective:
The aim of the present random clinical trial (RCT) was to determine the adjuvant effect of low-level laser therapy (LLLT) on healing tendon injury in patients.
Materials and methods:
In an RCT, 97 patients (114 fingers) with sharp injury in three zones of their hands were randomly divided into LLLT and control groups, using the unequal treatment allocation approach. Thirty-nine patients (31 males and 8 females, 46 fingers) were enrolled in the LLLT group, receiving 8–10 sessions of LLLT (red and infrared lasers) over the flexor tendon repaired area. In the control group, 58 patients were included, 20 patients did not come back for follow-up, and 38 patients (29 males and 9 females, 46 fingers) participated in the study. Patients were visited in days 28 − 32 after surgery. Passive range of motion (PROM), pain severity of groups, and patient satisfaction from LLLT were all recorded. The two observers, blind to the LLLT group assessed the data independently.
Results:
In two groups, no rupture was observed during 4 weeks postsurgery. None of the patients in the control group was able to perform the full passive flexion. There was a significant increase in PROM (t = 82.925, p = 0.000) and a significant pain reduction (t = −11.96, p = 0.000) in the LLLT group, compared with the control group. All Patients in the LLLT group were satisfied.
Conclusions:
LLLT is a proper adjuvant therapy in flexor tendon repair. Evidently, LLLT promotes tendon healing, alleviates the pain, and assists flexibility of soft tissue and joints, leading to the tremendous improvement in patient cooperation and compliance.
Introduction
P
Enwemeka et al. have assessed the effects of low-level laser therapy (LLLT) with He–Ne laser on tenotomizing Achilles tendons in rabbits. 3 –5 Enwemeka et al. showed an escalation in the rate of healing in morphometrical and biomechanical aspects. 3 –5
Subsequently, other researchers have studied different experimental models of tendon healing after LLLT, using histological, cellular, and molecular techniques. Guerra et al. divided the rats into the following groups: sham, partial tenotomy, partial tenotomy+laser [830 nm, 40 mW, 4 J/cm 2 , continuous wave (CW)], and partial tenotomy+laser (830 nm, 40 mW, 16 sec, 4 J/cm 2 at 20 Hz). Furthermore, glycosaminoglycan level, metachromasy and gait recovery, and collagen organization were analyzed. In the aforementioned study, an increase in the organized collagen bundles by pulsed wave LLLT (PW-LLLT) was demonstrated, eliciting a legitimate gait progress. 6 According to Bayat's data, the healing of complete tenotomized calcaneal tendons in diabetic rats was significantly accelerated, using LLLT (CW, He–Ne laser, 7.2 mW, 2.9 J/cm 2 ).
The positive effects of LLLT were reported by analyzing gene expression, and histological and tensiometrical techniques, in repairing calcaneal tendons in rats. 7,8 Carrinho et al. had six experimental groups: the primary group, complete tenotomy animals treated with LLLT [CW, indium, gallium, aluminum phosphide (InGaAlP), 685 nm laser, 3 J/cm 2 ]; the second group, complete tenotomy animals, treated with LLLT (CW, InGaAlP, 685-nm laser, 10 J/cm 2 ); the third group included complete tenotomy animals, treated with LLLT [CW, gallium, aluminum, arsenide (GaAlAs) 830-nm, of 3 J/cm 2 ]; the fourth group, comprised of complete tenotomy animals, treated with LLLT [CW, GaAlAs, 830-nm, 10 J/cm 2 ]; eventually, complete tenotomy control animals (placebo treatment); and the nontenotomy group. 9 The Collagen fiber organization was analyzed in all groups. The entire treated groups showed more arrangement of the collagen bundle organization, compared with the control group. In the first group, the most desirable results were observed. In Carrinho et al.'s study, all wavelength and energy densities could improve healing of a tenotomized calcaneal tendon; nonetheless, 658 nm wavelength and 3 J/cm 2 had the most effective outcomes. 9
Elwakil investigated the effect of LLLT (He–Ne laser, 1 J/cm 2 ) on the repairing process of surgically induced complete tenotomy in rabbits. The histopathology and tensiometry were evaluated; moreover, Elwakil accomplished satisfactory arrangement of the newly made collagen in repairing the tendon site as well as higher tensiometrical values, in the laser-treated group. Elwakil concluded that LLLT is efficient in postsurgical repair of lacerated and injured tendons in patients. Translucently, no side effects were found after their procedure. 10
LLLT (CW, 10 Hz, 830 nm, 9.7 J/cm 2 per fracture site, and 600 sec) has demonstrated a desirable outcome in accelerating the fracture healing in patients. 11
There are sporadic predictive factors after the flexor tendon repair procedure that patients should be aware of side effects. 12 The aim of the present random clinical trial (RCT) study was to investigate the outcomes of the combination of the PW LLLT with CW LLLT on the healing of digital flexor tendon injury and skin wounds in patients.
Materials and Methods
An RCT, involving a total of 97 patients and 114 digits with zone I, II, and III flexor tendon injuries, was conducted in the 15 Khordad Hospital of Shahid Beheshti University of Medical Sciences (SBMU) Tehran, Iran. This study was approved by the SBMU Medical Ethics Committee (SBMU.REC.1394.9), and received an IRCT Code (IRCT2017050233783N1). Moreover, the informed consents were obtained from patients. Using the unequal treatment allocation method, patients were randomly divided into two groups: the control (placebo) group (with 58 sample size) and the LLLT group (with 39 sample size), who received LLLT. Patients in the control group received placebo LLLT with the power off.
It is necessary to take into account that the efficiency (statistical power) has to be maximized for comparing the laser received group and the control group, and researchers typically employ an equal allocation in the participated patients. However, unequal allocation may be preferable in different cases; for instance, when the individuals in the control group would not come back for follow-up. Therefore, we used the stratified block randomization scheme with an allocation ratio of 0.60:0.40 to determine the unequal sample size. The allocation ratio of 0.60:0.40 would lead to random assignment of 60% of subjects in the control group, and 40% in the LLLT group. 13
Patients were recruited based on the hand surgeon's referral, over a period of 6 months from April to September 2015, including a total of 97 patients and 114 digits with zone I, II, and III flexor tendon injuries. The treatment was performed by the Department of Plastic Surgery. Primarily, the patients visited the emergency department and enrolled in two groups by a stratified block randomization scheme. A questionnaire, consisting of patient characteristics, such as personal information, demography of injury, and an informed consent form for participation in the study, was filled out (Table 1).
“a” in Table 1 shows the frequency and percentage of male and female who participated in the LLLT and control group. “b” in Table 1 shows mean ± SD of age variation in the groups. The frequency and percentage of each finger involved are presented separately, based on each group in “c” in Table 1. “d” in Table 1 shows the frequency and the percentage of each zone in various groups. Eventually, nerve and soft tissue injury frequency were presented; in addition, the percentage of gender, based on gender variable, is given in “e” in Table 1. Conspicuously, the main objective of the present scientific study was to analyze the total passive range of motion (PROM), pain control, and patients' satisfaction. Data are shown in Table 2.
All patients in the laser group were satisfied.
p < 0.001.
The exclusion criteria were as follows: multiple injuries to one flexor tendon, simultaneous injuries to bone and extensor tendons, skin loss, noncompliant patients or patients under 10 years, and gross contaminations of wounds. Utterly, the primary repair was performed under general or regional anesthesia, 6 − 24 h following the patient's admission. The surgery protocol under loop magnification was Brunner incision, exploring, and repairing flexor tendons by four-strand modified Kessler core suture method; moreover, periphery running suture was performed with 4/0 Nylon, and digital nerve repairing with 10/0 Nylon in 32 patients. Plaster brace was positioned for 4 weeks, in the wrist, metacarpophalangeal joint and interphalangeal joints in 10°, 90°, and 0° flexion, respectively. Precisely, the rehabilitation program started in the first 24 h in Kleinert regime. The patients were strictly advised to be under the supervision of a hand therapist and all the procedure ought to be done with consultation. The corresponding consort table is given in Fig. 1.
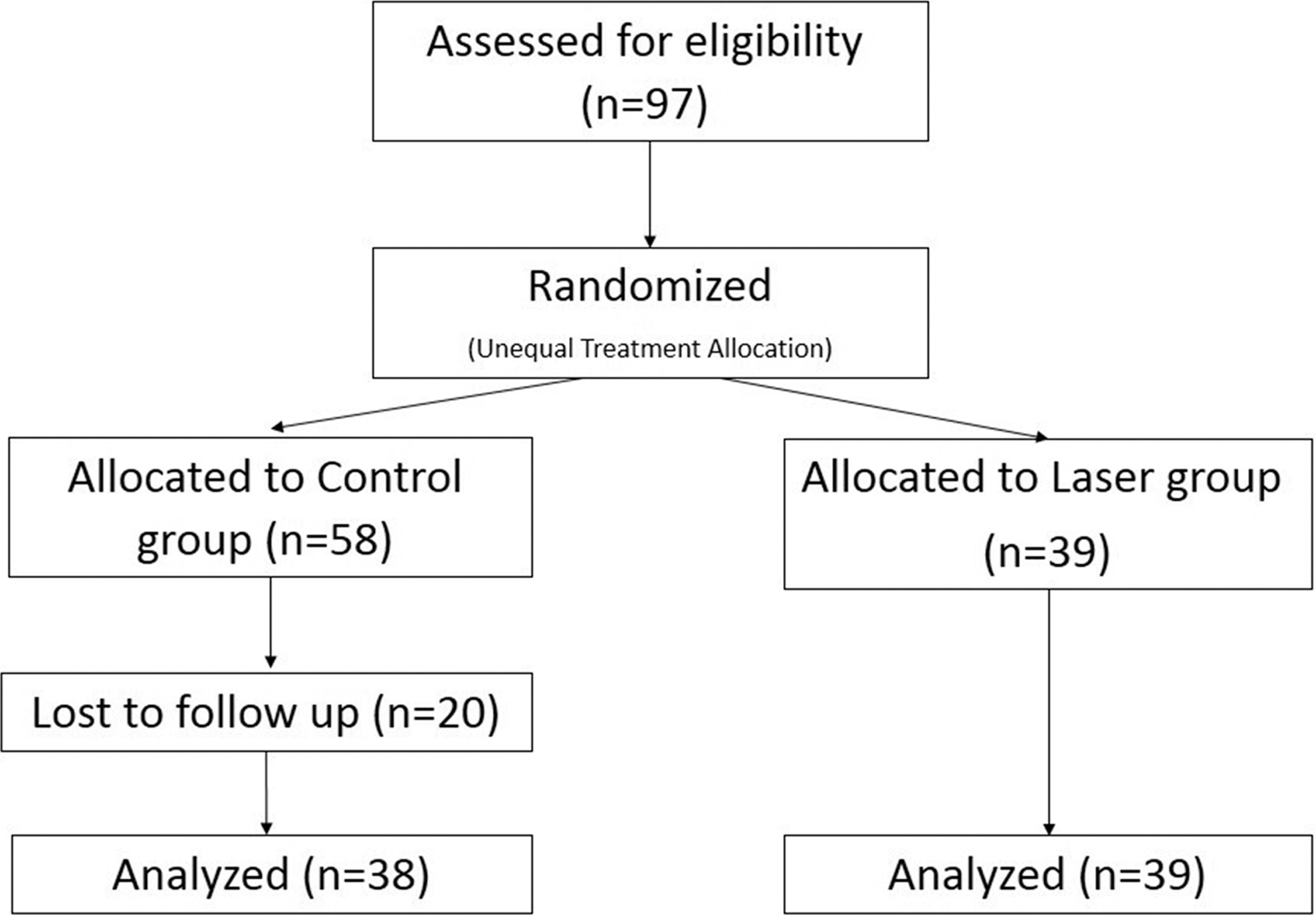
Consort table for our study.
The LLLT was performed from the second postoperative day, two or three times per week, for a period of 4 weeks for 10 sessions. In fact, immobilization remained in LLLT sessions and plaster brace was not removed. We used Mustang 2000 Laser device (Technical Co., Moscow, Russia) with two probes of red (KLO4) and infrared laser (LO7). The laser probes were placed over the repairing site in the contact method. The specifications of red and infrared lasers are shown in Tables 3 and 4, respectively. Particularly, red and infrared laser were used to accelerate tendon healing. 9
Patients and injury characteristics
Personal and clinical characteristics of patients were reported in “a–e” in Table 1. In the LLLT group, 39 patients with involvement of total 46 digits were treated. Primary repair was performed in 39 digits (84.7%), in 6–8 h to 24 h of trauma. Additional incision was necessary as lazy S in nine digits. During the study, one heavy smoker got wound infection, which was managed with conservative treatment with no sustained dysfunction.
Of 58 patients in the control group, 20 patients did not come back for follow-up and 38 patients were treated with involvement of total 46 fingers. Patients were visited on days 28 − 32 of surgery. None has attended a hand therapy clinic. At that time, splint was removed, wound, pliability of soft tissue, and passive ranges of movements at the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints were measured, using goniometer, and recorded.
Range of motion, pain assessment scales, and patient satisfaction
PROM at the PIP and DIP joints were measured by goniometer and recorded after the first session of LLLT, and at weekly intervals.
Pain severity was reported, using the Wong-Baker FACES pain rating scale (WBS). 14 In WBS scale, pain was rated from 0 (no pain) to 10 (the worst possible pain). 14 In each session after LLLT in LLLT group, or routine treatment in the control group, pain severity was recorded. Using a standard questionnaire for life scale, the patients rated their satisfaction with LLLT on an analog scale from 1 (dissatisfied) to 7 (completely satisfied). 15 Final assessment of the results was recorded at four weeks. The two observers, blind to the LLLT group, assessed the data independently.
Statistical analysis
One-sample Kolmogorov–Smirnov test was used for normality distribution. The student's t-test was used to analyze the data, particularly for comparing the range of motion and finger pain in the PROM, between the control and the laser-treated groups. Chi-square was used to compare distribution flexor tendon zone between groups. The data were shown as mean ± SD, and the p-value less than 0.05 was considered statistically significant.
Results
Kolmogorov–Smirnov test approved the normality assumption in a significant level of 0.05; t-test statistic was used to compare the control and LLLT groups.
Thirty-one (79%) subjects in the LLLT group and 29 (76%) subjects in the control group are male; data are presented in “a” in Table 1. The corresponding chi-square value is 0.113 with p = 0.737, showing no significant association between the frequency distribution of genders in the LLLT and control groups.
Mean ± SD for the patient's age, a t-statistic, and the corresponding p-value to test the hypothesis (there is a significant difference between the age of patients for the LLLT group and the control group), are reported in “b” in Table 1. The p-values 0.219 and 0.595 correspond to male and female categories, respectively, showing no significant difference between the mean of age in the LLLT and the control groups. “c” in Table 1, the frequency of fingers are distributed as: 9 (19%) for Finger 1, 5 (11%) for Finger 2, 5 (11%) for Finger 3, 9 (19%) for Finger 4, and 18 (40%) for Finger 5, in the LLLT group; moreover, 5 (11%) for Finger 1, 11 (23%) for Finger 2, 10 (22%) for Finger 3, 8 (17%) for Finger 4, and 12 (27%) for Finger 5, in the control group. The corresponding chi-square and p-value are 6.318 and 0.177, respectively, showing no significant association between the frequency distribution of fingers in the LLLT and control groups.
“d” in Table 1 shows the frequency distribution and p-values: 4 (8%) for zone 1, 37 (81%) for zone 2, and 5 (11%) for zone 3 in the LLLT group, and 2 (4%) for zone 1, 30 (65%) for zone 2, and 14 (31%) for zone 3 in the control group. The chi-square value is 6.318 with p-value of 0.059. Therefore, there is no significant association between the frequency distribution of zones in the LLLT and the control groups at significant levels of 0.05.
The number of nerves and soft tissue injury are distributed in “e” in Table 1. Table 1 shows the frequency distribution: 12 (71%) for the number of nerve injuries and 5 (29%) for the soft tissue injury in the LLLT group; moreover, 20 (95%) for the number of nerve injuries and 1 (5%) for the soft tissue injury in the control group; furthermore, the chi-square value is 4.293 with p = 0.038, showing a significant association between the type of injury in the LLLT and the control groups. This small association measure could be ignored at a significant value of 0.01.
No reduction in edema was observed in the LLLT group. The included patients received 10 sessions, but two patients received 8 sessions. There has been just one complication as wound infection in a heavy smoker patient that was managed with conservative treatment with oral antibiotics and wound management. After 4 weeks, no tendon rupture was observed and the patients had full satisfaction.
In the control group, after 4 weeks, full PROM in the PIP and DIP joints was not accomplished because of joint stiffness and pain. Active extension in the range of splint boundary was established.
Table 4 shows a significant increase in the total PROM (t = 82.925, p = 0.000) and a significant reduction of pain (t = −11.96, p = 0.000) was observed in the LLLT group, compared with the control group. Indeed, the patients were having full satisfaction with the treatment in the LLLT-treated group.
Discussion
The goal of the flexor tendon healing was to have less scarring in tendon healing. 16,17 The most common complications are adhesion formation, limiting the range of motion and rupture. 2,18 –20 Rehabilitation protocol becomes influenced by patient compliance, wound healing, and the method of the repair. 20 –26 The first 4 weeks are notably important for the hand functionality. 19
Any treatment program that can relieve pain and promote healing can facilitate tendon excursion and increase the range of active movement. There are many facts to consider regarding LLLT. The most wave absorption range in HeLa cells is in the range of 630, 860, and 880 nm; moreover, the proper radiation for promotion of DNA and protein synthesis are in the range of 400, 620, 680, 780, and 820 nm. 27 Different wavelengths were used for various purposes; for instance, 780 − 950 nm was used for deeper layers of tissues and red wavelengths for superficial layers in the range of 1–10 J/cm 2 . 27,28 The PW LLLT was selected with 810 nm, 5.85 J/cm 2 along with CW LLLT with 660 nm, and 2 J/cm 2 , for accelerating tendon repair. 9
The 15 Khordad Hospital is a referral center for hand trauma. Solely in 2014, 772 patients visited the hospital for hand traumas, of which 656 of them were young men and workers. There is a high volume of referral for this problem; therefore, there is a necessity for mandatory implementation of a detailed and all-inclusive postoperative programs. 24 There was an assessment of early active motion planned in an RCT study in our hospital, but only two third of the enrolled patients finished the total procedure. 26 According to the scientific studies, it is indicated that patients do not like to go through the rehabilitation programs and use thermoplastic splint. According to the data, 67% of patients do not use splint for personal activities such as using a restroom or taking a shower. 29 One third of the control group, in our study, did not follow the treatment.
In the current study, the postoperative adjuvant LLLT was evaluated in the first 4 weeks. Distinctly, it was proposed that the application of PW LLLT plus CW LLLT, immediately after flexor tendon repair could accelerate the healing process. 3 –10 Notably, the purpose in our experiment was to evaluate the outcomes of LLLT protocol.
Clearly, LLLT accelerates intracellular ATP and Ca2+ production as second messengers; in addition, it could mediate the proliferation and collagen synthesis of tenocytes, 30 stimulate collagen type I & III proliferation, increase tendon thickness, 31,32 affect the organization and aggregation of collagen bundles, 9 affect the remodeling of extracellular matrix, 33 stimulate tenocyte proliferation, 34 improve tendon healing, 35 prevent oxidative stress, and reduce tendon fibrosis. 36 Ozkan et al. reported that LLLT (Gallium arsenide laser, 100 Hz) had some beneficial effects on reducing edema in human tendon injury, using Whirpool program in patients after 12 weeks. 37
Nevertheless, in Ozkan et al's. study, no successful and significant desirable outcome was achieved from LLLT, on the other practical regaining factors of patients' flexor tendon injury rehabilitation; furthermore, authors suggested that more clinical studies in this field have to be done, using other LLLT protocol, to properly define the role of LLLT. 37 In the current study, it was shown that LLLT improved tendon gliding and excursion with less pain, permitting full PROM in the DIP and PIP joints. The compliance is defined as an active improvement in the rehabilitation programs. It has a profound impact on the clinical outcome of hand injuries in RCT. In fact, noncompliance with the medical regimen is a major problem in the healing process. 38 Rates of compliance with splint usage vary from 23% to 65% with the exercise regimens from 40% to 55%.
The issue is the limitation in this probe, which is, it is not predictable what percentage of patients would cooperate. The patients' perception of the effectiveness of treatment plays an essential role in the compliance. 38 It was found that LLLT could change patient's compliance. Patients participated in 8–10 sessions; all of them completed the treatment program; furthermore, their satisfaction was 6 − 7, on a scale of 1–10, according to the statistical analysis. The LLLT effects were translucent for the physicians. Laser effects remain effective for at least 4 weeks. 39 Even the patients living in suburbs completed their treatments since they were pleased with the result. Indeed, the administration of simultaneous red and infrared lasers, in the laser-treated group increased the efficacy significantly. 39 In the current study, there were two limitations: we were not able to measure temperature of skin finger, and blood perfusion as well.
Conclusions
It was ultimately concluded that LLLT could be an effective adjuvant therapy for patients with flexor tendon injury; furthermore, it could increase the PROM, alleviate pain, and increase patient cooperation.
Footnotes
Acknowledgments
This article was extracted from the hand surgery fellowship thesis at the Research & Developmental Center, performed at the 15 Khordad Educational Hospital, School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran. The authors would like to thank Hasan Davoudabadi and Payame Arabani for their contribution in providing the Mustang-2000 laser device. The authors would like to express their appreciation to Azade Riyahi for her sincere cooperation in the study.
Author Disclosure Statement
No competing financial interests exist.