
Abstract
Background:
Percutaneous lumbar laser discectomy is a minimally invasive treatment option for patients with a contained disc herniation with back and/or leg pain.
Objective:
The goal of this study was to present our experience and results with patients who underwent percutaneous lumbar laser discectomy in our practice.
Methods:
A total of 65 patients were included, and their charts were retrospectively reviewed.
Results:
The most common level at which we performed the laser discectomy was the L5/S1 level 47.4% of the time. The next most common level was L4/L5 37.2% of the time and the least common level was L3/4 15.4% of the time. Neuritis was reported in four patients, which was treated with medication in two patients, and resolved in all four patients. The average preprocedure visual analog scale (VAS) score was 7.6/10 (range, 5–10/10). There was an improvement in the VAS score at 2-week follow-up. The average VAS score at 2-week follow-up was 3.7/10 (range, 0–10/10). The average VAS score at 6-week follow-up was 4.3/10 (range, 0–8/10). The average VAS score at 3–6 months was 4.1/10 [range, 0–8/10 and at 6–12 months was 4.2 (range, 0–8/10)].
Conclusions:
Appropriate patient selection and following a systematic stepwise approach are important in treatment planning for patients in whom percutaneous laser discectomy is being considered. Following appropriate patient selection criteria maximizes the success rate of percutaneous laser discectomy. In our experience with patients with persistent back and/or leg pain not responding appropriately to conservative therapy, percutaneous laser discectomy offers a minimally invasive treatment option with nominal complications.
Background
B
Methods
From January 1, 2016 to December 31, 2017, we had a total of 65 patients undergoing percutaneous laser discectomy. Patients initially presented to our clinic with a chief complaint of back pain and/or radicular symptoms. Selection criteria are summarized in Table 1. All patients had a chief complaint of low back pain and/or radicular pain. The magnetic resonance imaging (MRI) was consistent with a disc herniation but without extrusion or sequestration. All the patients had their pain for a minimum of 6 months and had failed conservative therapy, including medication management and at least one treatment course of lumbar spine physiotherapy which consisted of a minimum of two sessions a week for 6 weeks. The patients also had failed lumbar epidural steroid injection therapy. All patients in our review had received a minimum of one lumbar epidural steroid injection. In addition, patient demographics include an average age of 43.7 years of age and a male to female ratio of 1.2:1.
MRI, magnetic resonance imaging.
The procedure was performed for all patients in an accredited outpatient surgery center under MAC anesthesia and fluoroscopic guidance (Fig. 1). The LASE® (laser assisted spinal endoscopy) endoscopic discectomy set was used from Clarus® medical (Fig. 1). During the procedure, after we gain appropriate access to the disc, we verify placement using contrast dye and anteroposterior and lateral fluoroscopic views (Fig. 2). Lumbar laser discectomy was performed using the Coherent VersaPulse PowerSuite® Holmium 30W laser. The procedure performed at an energy/pulse setting was 1.5 J/pulse at a pulse repetition rate of 10 Hz for a 15 W laser power output. Total energy delivered is 8000–12,000 J per disc level. A void is created in the nucleus pulposus viewed endoscopically (Fig. 3). The patients were followed up for 12 months after their procedure. The visual analog scale was used to grade the patients' pain levels preprocedure and at each follow-up. Patients had an average of 3.6 follow-up visits. Finally, we reviewed complications associated with the procedures, including bleeding, infection, discitis, and neuritis.

The LASE® endoscopic discectomy set from Clarus® medical. LASE, laser assisted spinal endoscopy.
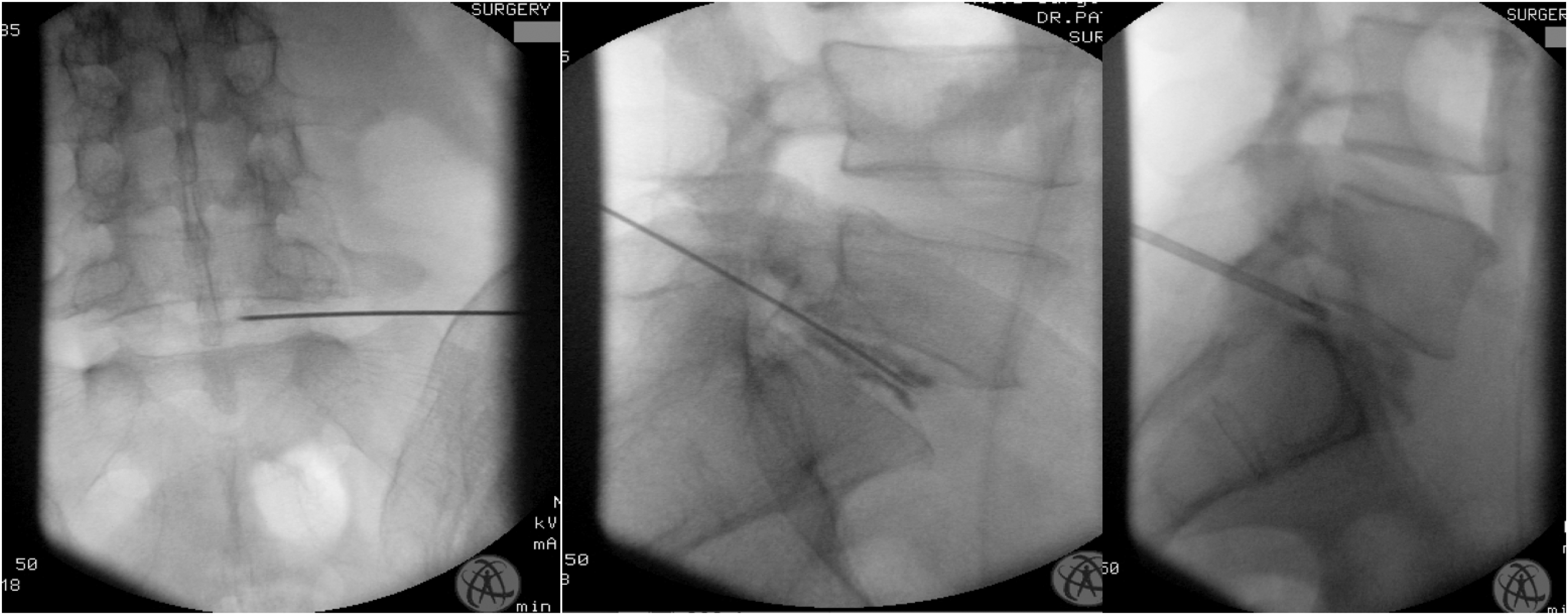
Anteroposterior and lateral fluoroscopic views with contrast demonstrating appropriate disc access.
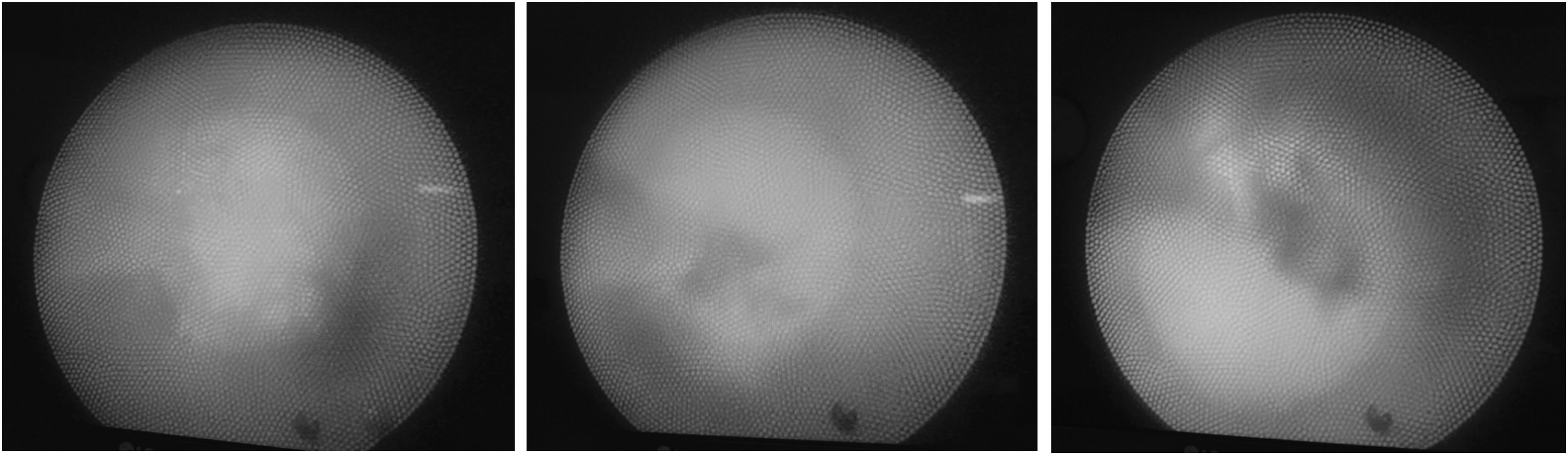
Endoscopic view of nucleus pulposus with void being created by laser.
Results
The most common level we performed the laser discectomy at was the L5/S1 level 47.4% of the time, the next most common level being L4/L5 37.2% of the time and the least common being L3/4 15.4% of the time. The majority of patients underwent a one level laser discectomy 76.9% of the time. Two level laser discectomies were performed in 23.1% of patients. The average size of patient's disc herniations was 4.2 mm. Neuritis was reported in four patients, which was diagnosed clinically at the 2-week follow-up visit. This was treated with medication in two patients and subsequently resolved in all four patients. There were no cases of bleeding, discitis, or infection. No other complications occurred with the procedure. The average preprocedure visual analog scale (VAS) score was 7.6/10 (range, 5–10/10). There was an improvement in the VAS score at 2-week follow-up (Fig. 4). The average VAS score at 2-week follow-up was 3.7/10 (range, 0–10/10). The average VAS score at 6-week follow-up was 4.3/10 (range, 0–8/10). The average VAS score at 3–6 months was 4.1/10 (range, 0–8/10). The average VAS score at 6–12 months was 4.2 (range, 0–8/10). The mean VAS scores from the preprocedure, 2 weeks postprocedure, 6 weeks postprocedure, 3–6 months postprocedure, and 6–12 months postprocedure groups were included in a one-way analysis of variance (ANOVA). There was a significant difference between the VAS scores at p < 0.05 [F(4, 320) = 41.56, p < 0.01].

VAS scores over time. VAS, visual analog scale.
Discussion
In our retrospective analysis, we demonstrated the outcomes of 65 patients who underwent percutaneous laser discectomy. The male to female ratio slightly favored men and patients most commonly underwent a one level procedure typically at the L5/S1 disc level. The complication rate was 6.1% which was neuritis that was treated conservatively and resolved in all cases. There were no cases of bleeding, infection, or discitis.
The current indications for percutaneous laser discectomy include discogenic pain, radicular pain, herniated lumbar discs, and lumbar spinal stenosis. 1,3 –6 Reported patient criteria in the literature include leg and back pain, disc protrusion on MRI but without disc extrusion or sequestration, chronic pain lasting longer than 3 months, preservation of at least 75% disc height, no neurological deficits, and no segmental instability. 1,7 Choy was the first to perform percutaneous laser discectomy in 1986 in Europe with a success rate of 75%. It was later FDA approved in the United States in 1991. 1,8 Ho:YAG lasers use the element holmium in yttrium aluminum garnet, which is a laser crystal and emits energy at a wavelength of 2.1 μm. The use of Ho:YAG rapidly became popular in clinical use because it offers precise cutting ability with minimal damage to adjacent tissue structures. In addition, it offers the ability to be used fiber optically through endoscopic means. The Ho:YAG laser has less than a 0.5 mm penetration in water and is an effective and safe method of delivering ablative energy. 9,10 Although initially designed for use in arthroscopic surgery, particularly discectomies, it is now used in many fields, including urology, dentistry, and general surgery. 11,12 With growing popularity, percutaneous laser discectomy has been used for more than 50,000 patients all over the world. 1
Erbas et al. had 197 patients undergo a percutaneous laser discectomy and documented pain relief with minimal complications. Of their patients, 12.7% underwent microsurgical discectomy after percutaneous laser discectomy. They concluded that percutaneous laser discectomy was a safe and effective procedure in appropriately selected patients. 1 Van Den Akker-van Marle et al. performed a cost utility analysis study in patients with lumbar disc herniation and radicular pain. They performed a randomized controlled trial comparing percutaneous laser discectomy to conventional surgery. They concluded that percutaneous laser discectomy followed by conventional surgery when needed resulted in significantly lower 1 year costs than conventional surgery alone. 13 McMillan et al. reported favorable outcomes for patients with lumbar discogenic and radicular pain during a 3-month follow-up without any instances of complication. In 30 patients with radicular pain, 80% of pain had improvement of symptoms with a mean improvement of 68%. In 32 patients with discogenic pain, 75% reported improvement with a mean improvement of 44%. 5 Tassi compared the results of 1000 patients who received either a percutaneous laser discectomy or a microdiscectomy for treatment of discogenic pain caused by a herniated lumbar disc. Of the patients who underwent microdiscectomy, 85.6% had a favorable outcome compared to 83.8% of patients who underwent percutaneous laser discectomy. However, compilations occurred in 2.2% of patients in the microdiscectomy compared to 0% in the percutaneous laser discectomy group. 6 Menchetti et al. reported a 70% success rate at a follow-up of 5 years in 900 patients in a multi-centric retrospective study on patients who had been therapy resistant for 6 months on average. 2 A systematic review of 2447 patients by Singh et al. showed evidence that percutaneous lumbar laser discectomy provides relief in properly selected patients with radicular pain due to a contained disc herniation. Level II-1 evidence (well-designed cohort or case–control analysis studies) from the U.S. Preventative Task Force exists for both short-term (less than 1 year) and long-term (greater than 1 year) effectiveness. 14 Gronemeyer et al. demonstrated the long-term effect in 200 patients treated for herniated lumbar discs who underwent percutaneous laser discectomy. Patients were observed over a 4-year period, and they noted a success rate of 74%. They also noted reduction in pain medication use and number of sick days used. Advantages of percutaneous laser discectomy included the minimally invasive approach in an outpatient setting with a low complication rate. 15 In a study by Brat et al. the changes in the size of a disc herniation were analyzed with repeat imaging at a mean follow-up time of 7.5 months in asymptomatic patients. They observed shrinking of the hernia in 66% of patients and overall stability of the disc height. 16
Conclusions
Appropriate patient selection and following a systematic stepwise approach ar important in treatment planning for patients in whom percutaneous laser discectomy is being considered. It has been suggested that minimally invasive intradiscal procedures be considered before open surgical procedures. 17,18 Following appropriate patient selection criteria maximizes the success rate of percutaneous laser discectomy. In our experience with patients with persistent pain not responding appropriately to conservative therapy, percutaneous laser discectomy offers an effective minimally invasive treatment option with nominal complications.
Footnotes
Author Disclosure Statement
No competing financial interests exist.