
Abstract
Introduction
C
Recently, resin matrix ceramic (RMC) materials have been developed to combine the physical and mechanical advantages of ceramics and improved flexural properties and low abrasiveness of composite resins. 4,7 The resin nanoceramic (RNC, Lava Ultimate; 3M ESPE, MN), polymer-infiltrated hybrid ceramic (PIHC; Enamic, Vita), and flexible hybrid ceramic (FHC, Cerasmart; GC Corporation) materials are popular resin matrix ceramic CAD/CAM blocks in the markets. 5,7,10,11 RMC has not only an altered stress distribution characteristic owing to the closer modulus of elasticity to dentine but also has an easier and safer milling-adjusting capacity when compared to glass matrix or polycrystalline ceramics. 7,10,12 In addition, the organic polymer compounds allow facilitating repair or characterization with direct composite resin filling and coating materials. 10
One of the main limitations of novel monolithic CAD/CAM restorative materials is the insufficiency of obtaining the exact optical properties of a natural tooth. Although there are some multi-chromatic blocks available in the markets, characterizations with direct composite resin filling and coating materials may be essential for some cases. 11 The higher flexural properties of RMC material and the adhesive cementation procedures may complain the removing process, in the case of fracture or replacement. Therefore, intraoral repair and layering methods with composite resin material addition possibly indicated to provide an efficient, functional, and aesthetically satisfying alternative to restoration replacement. 3,13 –15
Clinical applications of different surface conditioning and adhesive methods may be required for RMC to optimize the adhesion of the additional resin materials onto the substrate. 14 This conditioning (surface treatment) methods include chemical etching with hydrofluoric acid, acidulated phosphate fluoride, or phosphoric acid, airborne particle abrasion by using aluminum oxide, tribochemical silica coating, and laser treatment. 2,15 –18 Nevertheless, there is still no definitive information about which commercially available method is suitable and effective for the characterization and repair process of RMC. 12,15
Based on these considerations, the purpose of this study was to evaluate the shear bond strength (SBS) of a nanohybrid composite to the various RMC blocks using different surface treatments. The first null hypothesis was that the different surface treatment applications would not affect the SBS of a nanohybrid composite to RMC blocks. The second null hypothesis was that the effect of surface treatments would not vary depending on the type of RMC materials.
Materials and Methods
Three different CAD/CAM RMC blocks were used in this study. Manufacturers and compositions of the materials are presented in Table 1.
Al2O3, aluminum trioxide; Bis-EMA, bisphenol-A-ethoxylate glycidyl methacrylate; Bis-GMA, bisphenol-A-glycidyl methacrylate; DMA, dimethacrylate; FHC, flexible hybrid ceramic; HEMA, hydroxyethylmethacrylate; MDP, methacryloyloxy-decyl-dihydrogen-phosphate; MPS, methacryloxypropyltrimethoxysilane 2; PIHC, polymer-infiltrated hybrid ceramic; RMC, resin matrix ceramics; RNC, resin nanoceramic; SiO2, silicon dioxide; TEGDMA, triethylene glycol dimethacrylate; UDMA, urethane dimethacrylate; ZrO2, zirconium dioxide.
Specimen preparation
A total of 99 cubic form (6 × 6 × 2 mm) RMC specimens were prepared with a cutting machine (Mecatome T180; Presi Metallography, Eybens, France) under copious water. Specimens' thicknesses were measured with a digital micrometer (Digimatic Caliper; Mitutoyo MC, IL) and adjusted at required dimensions. Then, all specimens were fixed into autopolymerizing acrylic resin blocks (Meliodent; Heraeus Kulzer, NY), ground-finished using 200, 400, and 600-grit silicon carbide paper (3M ESPE) under water cooling, ultrasonically cleaned for 5 min in distilled water, and air-dried before surface treatments.
Surface treatments and scanning electron microscope analysis
The RMC specimens were randomly divided into three subgroups (n = 11) and the following surface treatments were applied, and are shown in Table 2. After the application of surface treatments, one sample for each of the nine subgroups was taken to examine with a scanning electron microscope (Nova Nano-SEM 450; FEI Comp., OR).
Nd:YAG, neodymium-doped yttrium aluminum garnet.
Application of resin composite
Before condensing the composite resin material, a methacryloxypropyltrimethoxysilane 2 (MPS) containing agent (Rely XTM Ceramic Primer; 3M ESPE) was applied onto the RMC specimens for 60 sec and lightly air-dried. Then, an adhesive material (Scotchbond Universal; 3M ESPE) was applied and cured for 20 sec using an LED light-curing unit (Blue-phase; Ivoclar Vivadent, Liechtenstein). Finally, a nanohybrid composite resin (Filtek Z-250; 3M ESPE) was incrementally layered onto the treated RMC surfaces using a silicone mold with a disc-shape cavity (2 × 3 mm) to standardize the dimensions of the composite. The application of adhesives and composite materials was performed according to the manufacturer's instructions. All bonded specimens were stored in distilled water at 37°C for 24 h and then subjected to thermal cycling between 5°C and 55°C for 3000 cycles at 30 sec in distilled water before SBS testing.
SBS test and failure mode analysis
A universal test machine (Autograph AGS X; Shimadzu Co, Kyoto, Japan) was used to perform SBS test at the crosshead speed of 1 mm/min. The SBS values were calculated in megapascals (Mpa) by dividing failure load (N) by the area of the composite resin (α = P/A). After the SBS test was completed, the failure modes of all specimens were analyzed by using an optical microscope (MP 320; Carl Zeiss, Oberkochen, Germany) at the magnification of 50. Failure types were categorized as an adhesive (between ceramic and composite resin interface), cohesive (failures related to the one type of material), and mixed.
Statistical analyses
Kolmogorov–Smirnov test of homogeneity was used for evaluating the normal distribution of the variables. Then, the SBS results were analyzed by two-way analysis of variance (ANOVA) for evaluating the effects of surface treatment, ceramic type, and their interactions. The mean SBS values were compared by using Tukey's multiple comparison test (α = 0.05). The failure modes were analyzed with Pearson chi-square test and the correlation between SBS and fracture modes also compared with Kendall's tau_b correlation analyses. SPSS 20.0 V statistical software (SPSS 20.0 V; SPSS, Inc., Chicago, IL) was used for statistical analyses and significance evaluated at p < 0.05 for all tests.
Results
The SBS values of untreated (control, Cnt) groups were compared with the values of other surface treatment groups. According to the two-way ANOVA, the RMC type, surface treatments, and their interaction were statistically significant (p < 0.05) (Table 3). The mean SBS values, standard deviations, and the statistical differences between RMC/surface treatment groups are listed in Table 4. Statistical differences were shown in these table as superscripts with capital letters, which indicate the differences between surface treatment, and the small caps indicate the differences between RMC groups.
Significantly different at p < 0.05.
The capital letters indicate the differences between the surface treatment groups and small letters indicates the differences between hybrid ceramic groups.
Statistical comparisons between hybrid ceramic/surface treatment groups were shown as letters and values having same letters are not significantly different for Tukey HSD test (p > 0.05).
SD, standard deviation.
The SBS values of Tbc and Lsr surface treatment applied RMC groups (15.92–25.41) were higher than Cnt groups (14.72–19.92). However, significant differences were observed between Cnt and Tbc (p < 0.001); Cnt and Lsr (p = 0.004) for FHC; between Cnt and Lsr (p < 0.001) for RNC; and Cnt and Tbc (p < 0.001) for PIHC groups. There were also significant differences observed between the Tbc and Lsr surface treatment groups, not only for RNC (p = 0.006) but also for PIHC (p < 0.001). When the same surface treatment applied RMC were compared, significant differences were observed between the RNC and other RMC, not only for Cnt but also for Lsr surface treatment groups (p < 0.05). There was no significant difference observed between the remaining groups (p > 0.05).
The SEM images of test groups are shown in Figs. 1 –3. Prominent changes were observed on the topographical surface of all treated groups when compared to the control specimens. There were significant differences among the same surface treatment applied RMC groups. Melted areas should be seen on the whole surface of Lsr applied PIHC group.
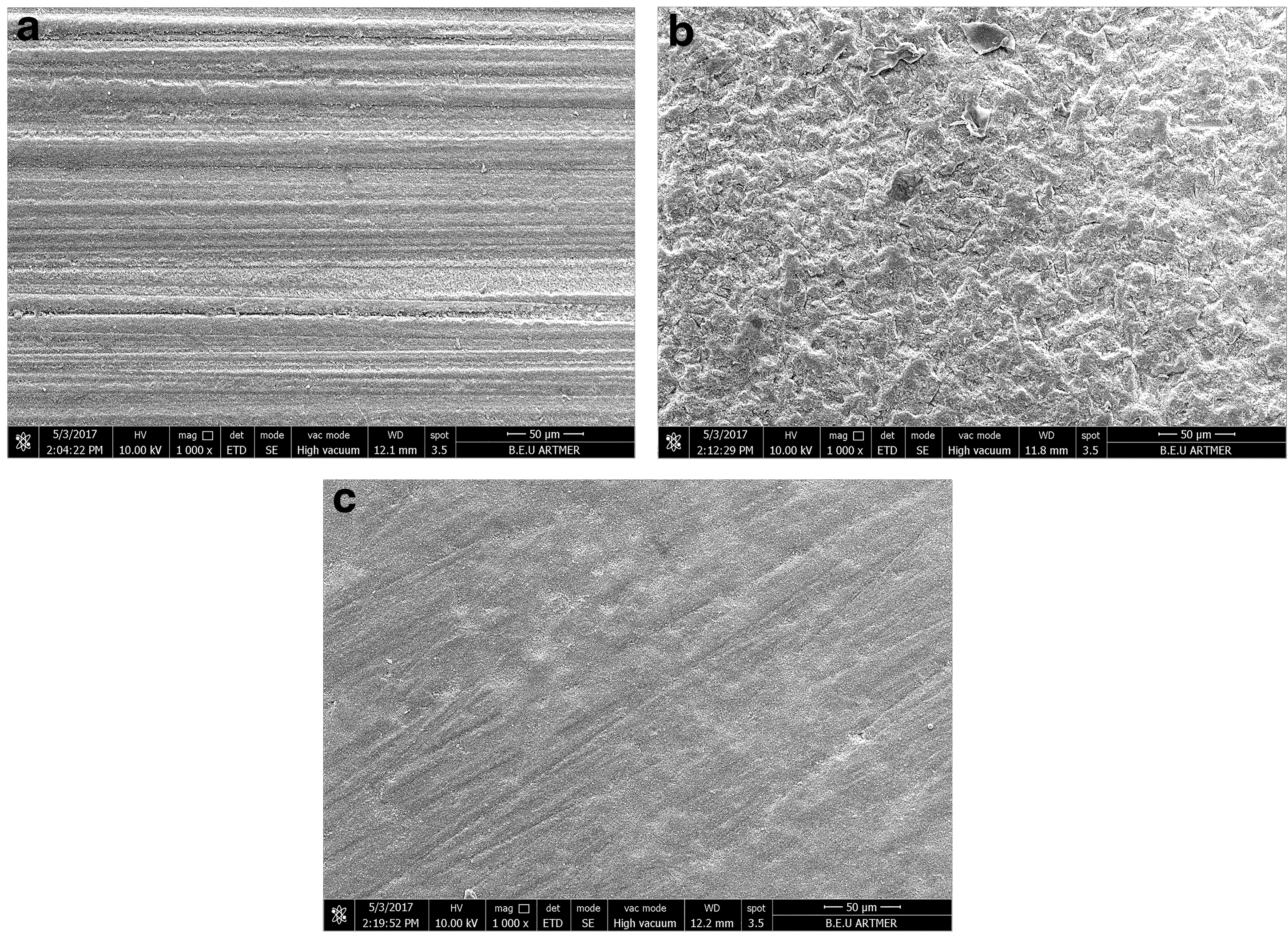
SEM images ( × 1000 magnification) of FHC RMC groups:

SEM images ( × 1000 magnification) of RNC RMC groups:
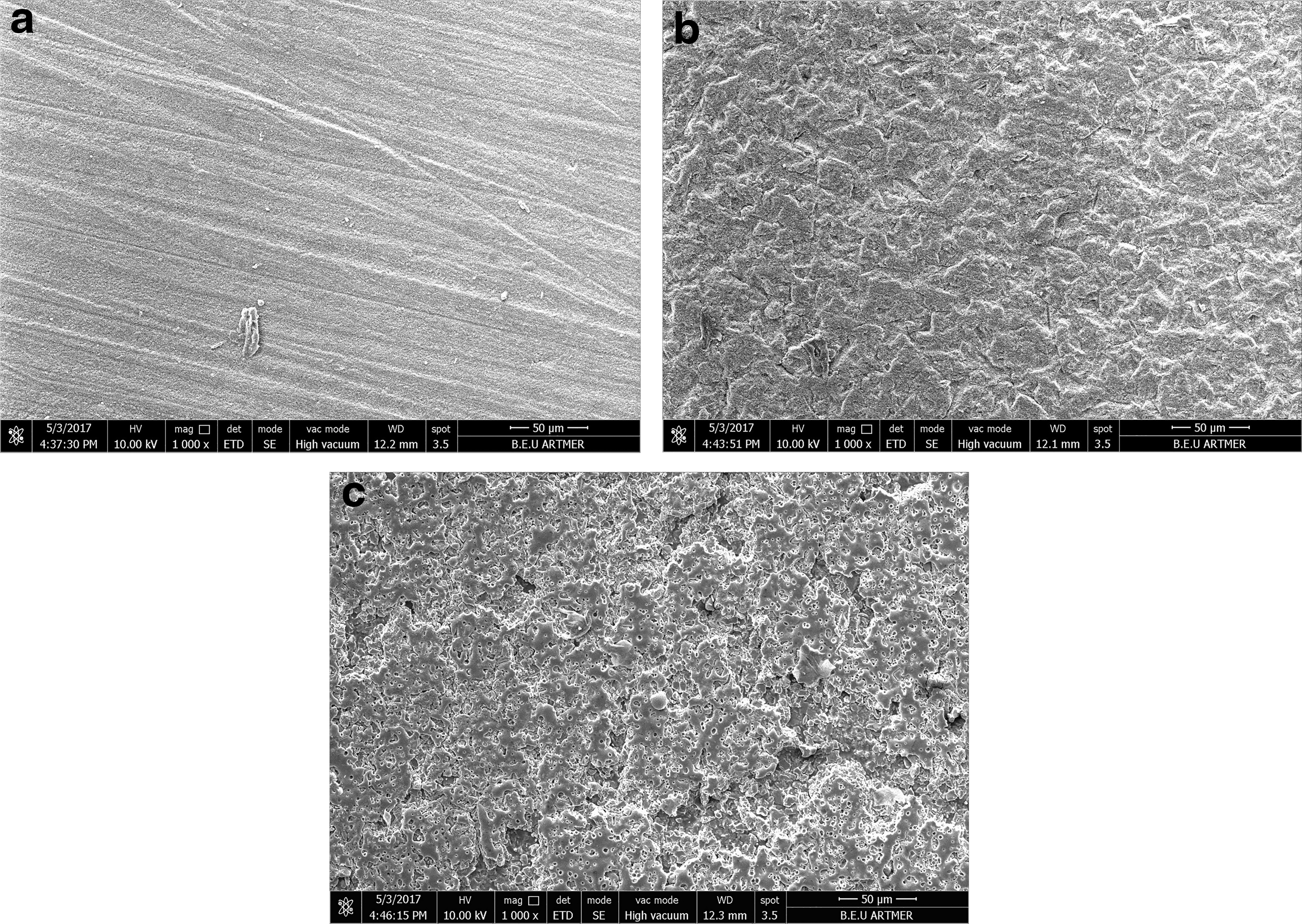
SEM ( × 1000 magnification) images of PIHC RMC groups:
A statistically significant difference was determined among the test groups according to the Pearson chi-square test (p < 0.001). When the fracture modes were analyzed, adhesive-type fractures were observed for all untreated RMC. However, the number of cohesive-type fractures was higher for each surface treatment applied group, except Lsr applied PIHC, and these fractures were observed in the side of RMC materials (Table 5). As a result of Kendall's tau b correlation analyses, the coefficient of correlation between SBS and fracture modes was statistically significant (p < 0.001, r 2 = 0.326), indicating that these two variables were moderately correlated.
Discussion
From the results of this in vitro study, both null hypotheses were rejected. Because, not only were the surface treatment techniques effective on the SBS of a nanohybrid composite to RMC blocks but also the effect of these techniques would vary depending on the type of RMC materials.
RMC materials have a composite structure that consists of both organic matrix and highly filled ceramic particles with a bridgework silane agent. 4,5,7,10,12 This versatile structure may provide a superior feature that allows a high degree of characterization, adjustment, and repair extraorally or intraorally. 5,7,10 Before this procedure, a bifunctional monomer of silane agent application is critical to ensure a chemical adhesion between organic and inorganic substrates. The organofunctional monomeric ends of silane molecules react with the methacrylate groups of adhesive resin and the integrated polymer components of RMC materials. 4,13 Concurrently, the hydroxyl groups maintain strong covalent bonds to inorganic components of RMC materials.
The bond with ceramics happens by means of a condensation reaction between the silanol groups (Si–OH) in the ceramic surface and the silanol group of the hydrolyzed silane molecule, creating a siloxane bond (Si–O–Si) and producing a water molecule by-product. 2,3,8 Silane also enhances ceramic–resin bonds by promoting the wetting of the ceramic surface, making the penetration of the resin into the microscopic porosities of the ceramic substrate more complete. 2,13 In a related study, no adhesion was found between veneering composite resins and nonconditioned polymeric CAD/CAM blocks, and thus attributed to the insufficient free radicals on polymer materials. 9 Therefore, an adhesive bonding technique was performed with an MPS silane agent and adhesive resin application for all RMC blocks. However, it was indicated in a related study that unsatisfactory bond strength results would be gained if an adhesive bonding technique is performed without any prior surface conditioning to enhance mechanical retention on RMC blocks. 4
The total of physical and chemical bonding is a main point in adhesion guideline. The first step of adhesion systems generally includes mechanical surface enhancement followed by the application of the chemical agent. Numerous studies suggested that it is essential to achieve a microretentive ceramic surface to facilitate ceramic repair with a resin composite. 1,3,4,14 –16
Hydrofluoric (HF) acid etching, abrasion with diamond rotary instruments, airborne particle abrasion with Al2O3, or silica coating were declared as the most favorable conditioning methods regardless of the ceramic type. While the HF acid etching and then applying a silane coupling agent was suggested as the most appropriate surface treatment method for feldspathic ceramics, the potentially harmful and irritating effects of HF on oral tissues limited its use during the intraoral repair process. 2,3,16,17 The acid etching process was also shown questionable for some ceramics, because of its inadequate effects on altering the surface roughness and weakening effect on the biaxial flexural strength of low fusing feldspathic ceramics; it merely has a surface cleaning effect and alters the surface free energy. 15,18 –20 The use of acid etching surface pretreatment protocol was not performed not only for these unfavorable results but also the restriction of the manufacturer of RNC material related to the modification of resident surface flaw population.
Airborne particle abrasion with Al2O3 particles is also a commonly preferred technique for creating a roughened surface on ceramics not only in prosthodontic laboratories but also in dental clinics. 13,16,17 However, the airborne particle abrasion technique is not only unavailable for intraoral repair and characterization procedures but also has potential destructive effects on the surface of RMC materials due to the large particle size (>110 μm) and high-pressure settings, which result in huge volume loss. 4,13 While the tribochemical silica coating followed by the silanization technique is more suitable for intraoral usage, which also increases the silica content on the ceramic surface, it evidently enhanced the bond strength between the ceramic surfaces and the resin materials. 9,13,14
It was indicated in related studies that the 15–25 MPa bond strength values might be ideal for the clinical applications of direct composite resin to RMC, regardless of the composite resin material and repair method. 17 When the SBS results of this study were evaluated according to these limits, it may be concluded that using chemical bonding procedures without any physical process for the RMC materials was nearly enough to obtain adequate bonding results with nanohybrid composites. On the other hand, significantly higher SBS values were obtained for FHC and PIHC RMC materials, using the tribochemical silica coating technique, which is also in line with the results of previous studies. 17
The laser irradiation is also an alternative treatment technique, especially for intraoral usage to create rougher RMC surfaces by removing of the glass phase and increase the micromechanical retention with resin materials. 16 In this study, using a neodymium-doped yttrium aluminum garnet (Nd:YAG) laser irradiation at an energy setting of 3 W (150 mJ/pulse and 20 Hz for 20 sec) was significantly effective on the SBS values of FHC and RNC RMC materials. In contrast to our findings, insufficient bond strength values were declared in related studies for the Er:YAG laser-irradiated feldspathic ceramics at energy settings of neither 10 W (500 mJ/pulse and 20 Hz for 20 sec) 16 nor 2 W (500 mJ/pulse and 4 Hz for 120 sec). 21 Some surface deformations like erosion and melting points had been observed for the Er:YAG laser irradiation at 10 W energy setting 16 and inadequate surface roughing at 2 W setting, 21 which were shown as the reason for lower bonding results.
In this study, significant differences have been detected between same surface treatment applied RMC material groups, and this situation was associated with the variations of the material microstructure. 12,17 These variations include the type, grain size, ratio of the filler particles, and the polymer matrix of the material. The PIHC is the densest inorganic filler containing RMC material with the porous feldspathic ceramic network (86% by weight), which is also strengthened by an interpenetrating polymer matrix. 7,11 The inorganic filler ratio of RNC (80% by weight) and FHC (71% by weight) RMC materials is gradually decreased and commonly consist of silica-zirconia and silica-barium glass nanoparticles, respectively. 4,7,10
The relationship between the filler content and bond strength had been investigated by a previous in vitro study and stated that bond strength increases with increasing filler content. 22 In this study, while the SBS values of Tbc surface treatment applied RMC groups have been completely parallel with this result, the SBS values of PIHC RMC material were in contrast for Cnt and Lsr groups. The low SBS values for Lsr treatment applied PIHC material should be interpreted with the deformation of the laser surface treatment process on the material structure, which was also shown in the SEM image as melting points detected on the whole material surface. According to this result, the use of Nd:YAG laser treatment process at the energy settings of this study may be questionable for PIHC and further investigations should be performed to gain better SBS values for this material without any damaging.
Aging conditions should be considered and included in the planning of restoration characterization and repair procedures. Aging conditions such as humid and thermally dynamic oral environment may lead to some alterations on the surface, mechanical properties, and long-term performance of restorative materials. 3,4,11,17 For this reason, the specimens were both water stored and thermocycled in this study to evaluate the effect of aging on the performance of the bonded interfaces. The water sorption scale of a composite resin material may be related to the monomer hydrophobicity. 11 All the tested RMC materials in this study consist of hydrophobic urethane dimethacrylate (UDMA), and mostly contain hydrophilic triethylene glycol dimethacrylate (TEGDMA) and bisphenol-A-glycidyl methacrylate (Bis-GMA), which are shown responsible of higher water sorption. 9,11 The highest resin matrix containing RMC of FHC in this study had lower SBS values than the others, almost for all treatment groups, which might be caused by the water penetration into the resin matrix of the block following 1-day water storage and thermocycling aging procedures.
A moderately positive correlation was detected in this study between SBS values and failure mode results. According to the failure mode analysis in this study, it was revealed that all untreated RMC mostly showed adhesive failure between composite and ceramic; the number of cohesive-type fractures was higher for both Tbc and Lsr surface treatment applied groups, except En_Lsr. This result was in agreement with a previous study and noticed that better adhesion with cohesive-mixed failures had been gained for surface treatment applied RMC materials, whereas adhesive failures for untreated ceramics typically associated with low bond strength values. 4 The unexpected fracture modes for the Lsr applied PIHC group may be explained with the damage of the laser surface treatment on the surface of the material, also mentioned before, and composite seemed to exceed the strength of the material itself.
The design of this in vitro study has several limitations, making it difficult to compare with all clinical situations. The SBS test has been widely used for in vitro investigations of resin ceramics, has also some limitations about the uniform stress distribution across the material. 4,16,17 The variables about the composite resin and adhesive materials could influence the bond strength of ceramics. 4,6 In this study, a nanohybrid composite resin restorative material was preferred for intraoral repair and characterization procedure due to improved esthetic and mechanic properties. 4,17,23 The efficiency of tested surface treatments, especially the Nd:YAG laser treatment, should be evaluated at different irradiation time and power settings for surface roughening of RMC. 24 The bond strength of different types of composite resin materials to newly developed RMC should be evaluated in further in vitro and in vivo studies using various surface treatments and adhesive systems.
Conclusions
Within the limitations of this in vitro study, the following conclusions could be drawn:
The type of surface treatment and RMC materials were both significant on the SBS of nanohybrid composite to the RMC blocks. The chemical bonding procedures without any physical process were nearly enough to obtain adequate bonding results between nanohybrid composites and RMC materials. However, using tribochemical silica coating or Nd:YAG laser irradiation techniques significantly improved the SBS values for most of the RMC materials. The use of Nd:YAG laser treatment process at the energy settings of 3 W (150 mJ/pulse and 20 Hz for 20 sec) should be questionable for PIHC RMC material. Same surface treatment technique may not provide similar successful results for all types of RMC materials, and it is recommended to choose the most effective and reliable technique for clinical application.
Footnotes
Acknowledgments
This in vitro study has been financially supported by Ordu University Department of Scientific Investigation Projects with the number HD-1617.
Author Disclosure Statement
No competing financial interests exist.