
Abstract
Objectives:
The aim of the present study was to investigate differences in the amount of dentin microcracking caused by the use of a 970-nm diode laser with different parameters for endodontic disinfection procedures.
Materials and methods:
Forty dental roots underwent mechanical endodontic preparation in a standardized manner. Each sample was randomly allocated to 4 groups receiving constant or interval laser irradiation time, calcium hydroxide disinfection, or a control group, with 10 samples per group. Transmission microscopy of all samples was performed at T0, before preparation; T1, immediately after endodontic preparation; and T2, after laser application in the laser groups and after 1 week of storage in the control and calcium hydroxide groups. The microcracks at each measurement point were color labeled, layered, and compared.
Results:
No significant differences were noted at T0 and T1 (p > 0.05). Statistically significant differences in the overall amount of microcracking were observed between the constant laser group and all other groups at T2 (p < 0.05). There were no statistically significant differences between the interval laser group, the calcium hydroxide group, and the control group at T2 in relation to the overall amount of microcracking (p > 0.05). When the root sections were analyzed separately, the coronal section did not show any statistically significant differences between the constant laser and interval laser groups (p > 0.05). The middle and apical root sections in the constant laser group showed the significantly largest amount of crack formation in comparison with the other groups (p < 0.05). The statistically significantly smallest amount of crack formation was observed in the apical third for all groups (p < 0.05).
Conclusions:
Clinically proposed laser protocol seems to be able to prevent side effects to the tissue, such as microcracks of the root canal dentine.
Introduction
T
Various rotating endodontic systems with different designs and configurations have improved the mechanical procedures used for root canal preparation. 2,3 Even with modern systems, however, various amounts of stress on the root canal walls are still generated during preparation procedures. 4 Several studies have hypothesized that dentin microcracks are caused by the use of rotary endodontic instruments with varying depths and extensions, which may lead to vertical root fractures and may ultimately result in tooth loss. 2,5,6
Calcium hydroxide is used for chemical disinfection of the root canal system, on the basis of its antibacterial effects, inhibition of root desorption, and its calcifying action. 7,8 The antibacterial effect of the strongly alkaline hydroxide ions is based on destruction of bacterial cell membranes, denaturation of structural proteins and enzymes, and damage to the DNA. 9 Negative side effects, such as the formation of microcracks in the hard tissue of the tooth, have also been observed when calcium hydroxide is used. 10,11
Previous studies have shown that due to its penetration depth of 130–300 μm in the dentinal tubules, chemical disinfection does not achieve complete elimination of bacteria, since bacteria such as Streptococcus mutans penetrate up to 1150 μm into the dental canaliculi. 12,13
Lasers provide an alternative to chemical disinfection of the canal. The Nd:YAG laser has a wavelength of 1064 nm and is well absorbed by chromophores that are found in oral and dental tissues. 14 It is therefore very suitable for decontamination of the root canal. 15 The Nd:YAG laser also has a penetration depth of up to 1000 μm into the root canal dentine. 16
The penetration depth of the diode laser is slightly less, but it also has fewer thermal side effects due to its slightly shorter wavelength of 810–980 nm. 17 With irradiation using Nd:YAG and diode lasers, bacterial colonization can be reduced by up to 99.9%, mainly due to thermal interactions. 15,18,19 With a wavelength of 810 nm in particular, the diode laser has a very high level of absorption in oral and dental tissues and low absorption in water. This makes it very suitable for decontamination, as it can destroy the pigments in the bacterial cell walls. However, isolated studies have also shown that there is a risk of dental hard-tissue chipping by the use of diode laser. 20 In endodontic applications, the bactericidal effect of the diode laser has been found to be similar to that of the Nd:YAG laser, but it has fewer thermal effects and is consequently associated with a lower risk of causing microcracks in the dentin. 17 Gutknecht et al. have reported that crack formation resulting from laser application in the root canal correlates with temperature increases, based on the following parameters: wavelength, power, frequency, pulse duration, pause duration, and time of irradiation. 21 Decontaminating root canals using diode lasers is an alternative, which has a higher impact on bacteria reduction in comparison with the conventional chemical decontamination technique. Both techniques are associated with a risk of microcracks in the dental hard tissue.
As far as we are aware, there have been no published studies comparing the microcracks that result with the two techniques. There is consequently no current evidence available on the question of whether diode laser decontamination of the root canal leads to a more or fewer dentin microcracks in comparison with the chemical decontamination process. The aim of the present study was therefore to investigate whether there are any differences in the amount of dentin microcracking that occurs when a 970-nm diode laser is used with different application modes in the root canal, in comparison first with calcium hydroxide in the root canal with an application time of 1 week and second with a control group without any adjunctive disinfection protocol. Therefore, the hypothesis of the occurrence of a higher amount of microcracks caused by irregular laser irradiation should be tested.
Materials and Methods
The study included 40 freshly extracted human teeth with 1 straight root, from different patients. Immediately after extraction, the teeth were stored in 0.9% isotonic sodium chloride (NaCl) solution with 0.001% sodium azide. The study was conducted in full accordance with established ethical principles (World Medical Association Declaration of Helsinki, version VI, 2002). All of the patients were informed that their teeth were to be used in an in vitro research project.
Tooth preparation
All teeth were cleaned with a brush (Snap-On Brush; Kerr, Rastatt, Germany) and cleared of tissue remnants and concrements using a hand scaler (Hu-Friedy Mfg. Co., LLC, Chicago, IL). The teeth were then examined for initial microcracks under a microscope and optionally excluded. The teeth were decapitated using a torpedo-shaped dental diamond fraise (Colorless; Komet, Brasseler GmbH & Co. KG, Lemgo, Germany) at 40,000 rev/min to expose the root canal. The average length of the roots was 12 mm. After this preparation step, the initial measurements were made.
The preparation of the teeth continued with standardized endodontic preparation of the canal using the VDW.Silver Reciproc (VDW GmbH, Munich, Germany) endo motor for reciprocating and classical preparation techniques and a rotary nickel-titanium file system (FlexMaster; VDW GmbH) up to size 45.04. Each tooth was randomly assigned, on a computer-generated basis, to 1 of 4 different study groups, resulting in 10 samples in each group.
Laser system and parameters
A class IV diode laser system (SiroLaser Advance; Dentsply Sirona, Bensheim, Germany) with a wavelength of 970 nm was used. The system was set to an output power of 1.5 W in chopped mode with a frequency of 15 Hz and a duty cycle of 50%, resulting in an effective output of 2390 ± 3 W/cm2 at the fiber tip. These parameters are the preliminary settings for endodontic treatments based on the standards described by Gutknecht et al. 21 The handpiece was used with a 200-μm (core diameter) fiber and was activated with a finger switch (Table 1).
Laser Parameters Used in the Present Study
Definition of the study groups
Constant laser group (group 1)
The optical fiber was guided for 1 min without interruption in circular movements with a vertical speed of 2 mm/sec from apical to coronal and back again. After an application time of 1 min, the samples were stored again in the 0.9% isotonic NaCl solution with 0.001% sodium azide (Table 1).
Interval laser group (group 2)
The optical fiber was moved from apical to coronal with a vertical speed of 2 mm/sec four times for 5 sec, with a pause of 5 sec in between. This laser interval is based on the guidelines for irradiation in the dental root canal described by Gutknecht et al. for avoiding thermal damage of tooth supportive periodontal tissues (Table 1). 21
Calcium hydroxide group (group 3)
After mechanical endodontic preparation and photographic documentation, the canals were dried with paper tips, and Calxyl (red; OCO-Präparate GmbH, Dirmstein, Germany) was placed into the canal using a Lentulo instrument (VDW GmbH). The samples were then individually stored for 1 week in the 0.9% isotonic NaCl solution with 0.001% sodium azide.
Control group (group 4)
The samples were stored for 1 week after the root canal preparation in the 0.9% isotonic NaCl solution with 0.001% sodium azide, with no subsequent treatment procedures.
Photo documentation and evaluation
After decapitation of the teeth, silicone molds (Flexitime Easy Putty; Heraeus Kulzer GmbH, Hanau, Germany) were produced to allow reproducible positioning for photographic documentation. For this purpose, the teeth were stored in such a way that they were half-embedded in the silicone mass. After silicone curing, the root surface in contact with the silicone was cut in a wedge shape, to hold the root laterally with an almost completely free surface. This allowed optimal transillumination of the tooth with a cold light lamp under the microscope.
Photos were taken at three different time points (T0, T1, and T2) for measurement with an optical microscope (Z6 APO; Leica, Wetzlar, Germany) at eightfold magnification. Photographic documentation of all samples was carried out at T0, immediately after the tooth preparation and before endodontic preparation of the canal; at T1, immediately after endodontic preparation of the canal; and at T2 after laser application in groups 1 and 2 and after 1 week of storage in 0.9% isotonic NaCl solution with 0.001% sodium azide in groups 3 and 4.
A total of 420 photos were thus taken of the 40 teeth, from 2 sides (mesial and distal) and at 3 time points. The microcracks observed at each measurement point were color labeled, layered, and compared using the Photoshop CS6 program (Adobe Systems Software Ireland Limited, Dublin, Ireland) by one observer who did not perform the tests. The observer was blinded because he had no information which sample belonged to which group. The plotted pixels (microcrack quantity) were also calculated using Photoshop CS6 at the different measurement times (T0 = blue, T1 = red, and T2 = turquoise) and documented in Excel (Microsoft, Redmond, Washington). These calculations were done for the apical third of the root (3 mm), the central third of the root (3 mm), the coronal third of the root (3 mm), and the sections in total (9 mm from the apex) (Fig. 1).
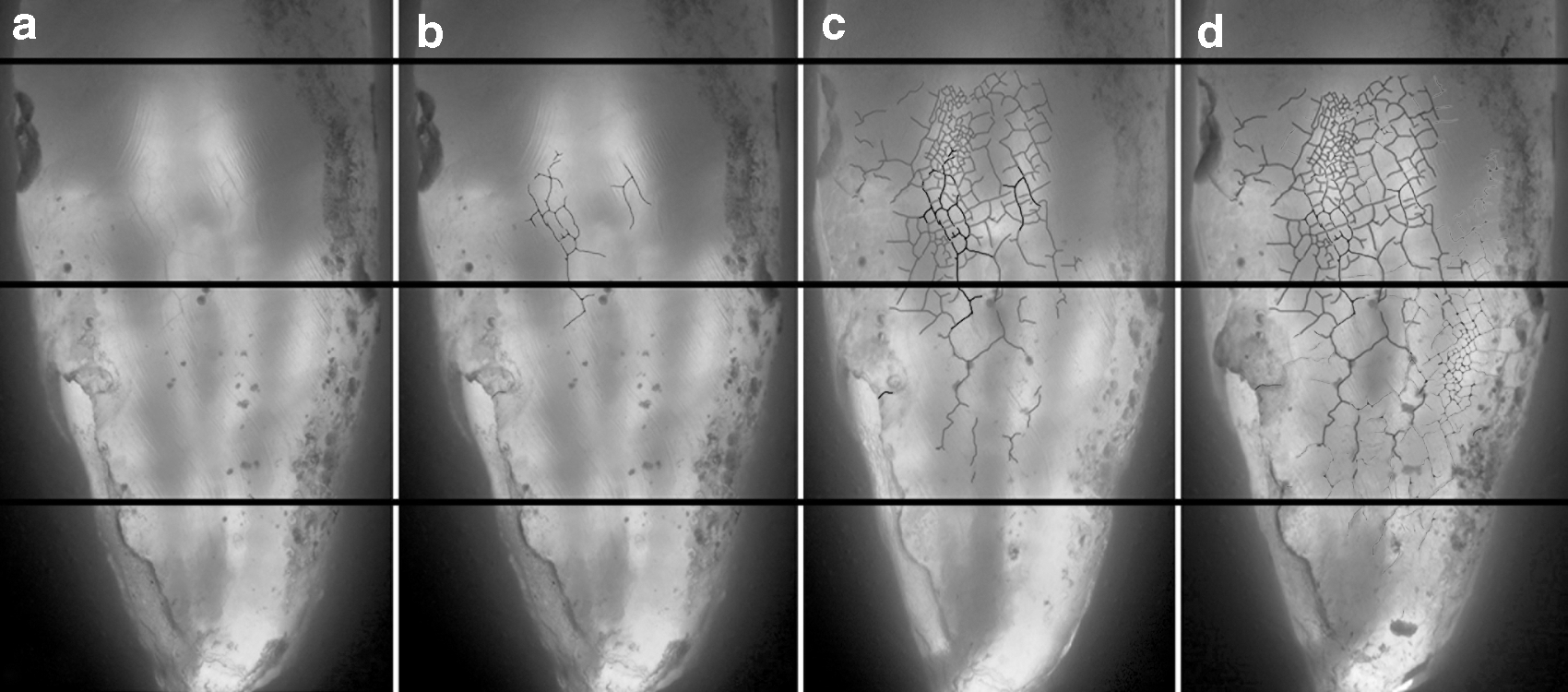
Analysis of crack formation by transmitted light microscopy (original magnification 8 × ). The baseline situation without
Statistics
A power analysis was performed before the study. Analyzing the data for five teeth actually measured in each group, an effect size of 1.3 was estimated. For an alpha error of 0.05 and a power of 0.8, a total sample size of at least nine specimens in each group was calculated. The normal distribution of the values was assessed using the Shapiro–Wilk test. Since not all data were normally distributed, values for crack formation between the groups were analyzed using a nonparametric test (Kruskal–Wallis) and with Mann–Whitney pairwise comparisons. Comparisons of crack formation between the coronal, middle, and apical thirds of each root were performed using nonparametric tests for related samples (Friedman and Wilcoxon tests). Differences were considered as statistically significant at p < 0.05. The sequentially rejective Bonferroni correction of the critical p-value was used when multiple statistical tests were performed simultaneously on a single dataset. Box plot diagrams are used to show the median, first and third quartiles, and minimum and maximum values (whiskers). Values of more than 1.5 to three times the interquartile range are specified as outliers and marked as data points. Values more than thrice the interquartile range are specified as distant outliers and marked as asterisks.
Results
Crack formation in root dentin was observed using transmitted-light microscopy in all of the tooth samples examined. Different quantities of cracking were therefore evaluated in relation to both the study group and the three different sections of the root (Fig. 1).
Impact of the treatment procedure
Comparison of the amount of crack formation showed significant differences relative to the treatment groups. However, these differences were only observed after root canal preparation in relation to the additional disinfection protocol. At baseline, overall crack formation did not differ between the treatment groups (p > 0.05), with a median value of 1.218 pixel units (min. 0, max. 36.267, interquartile range 10.531). Root canal preparation caused a statistically significant increase in crack formation (median value 8.047, min. 0, max. 55.460, interquartile range 27.557; p < 0.05), with no differences between the treatment groups (p > 0.05). The additional disinfection protocol had a statistically significant impact on the results. The largest amount of crack formation was observed with the 970-nm laser during constant irradiation (p < 0.05) (Fig. 2). In comparison with the untreated control group, both the calcium hydroxide group and the group with laser irradiation in interval mode did not show statistically significant amounts of crack formation (p > 0.05) (Table 2). Disregarding the amount of crack formation after root canal preparation and focusing only on cracks caused by each additional treatment procedure, the largest amount of crack formation was also found after laser treatment during constant irradiation (p < 0.05) (Table 3), with no differences between the other groups (p > 0.05) (Fig. 3).
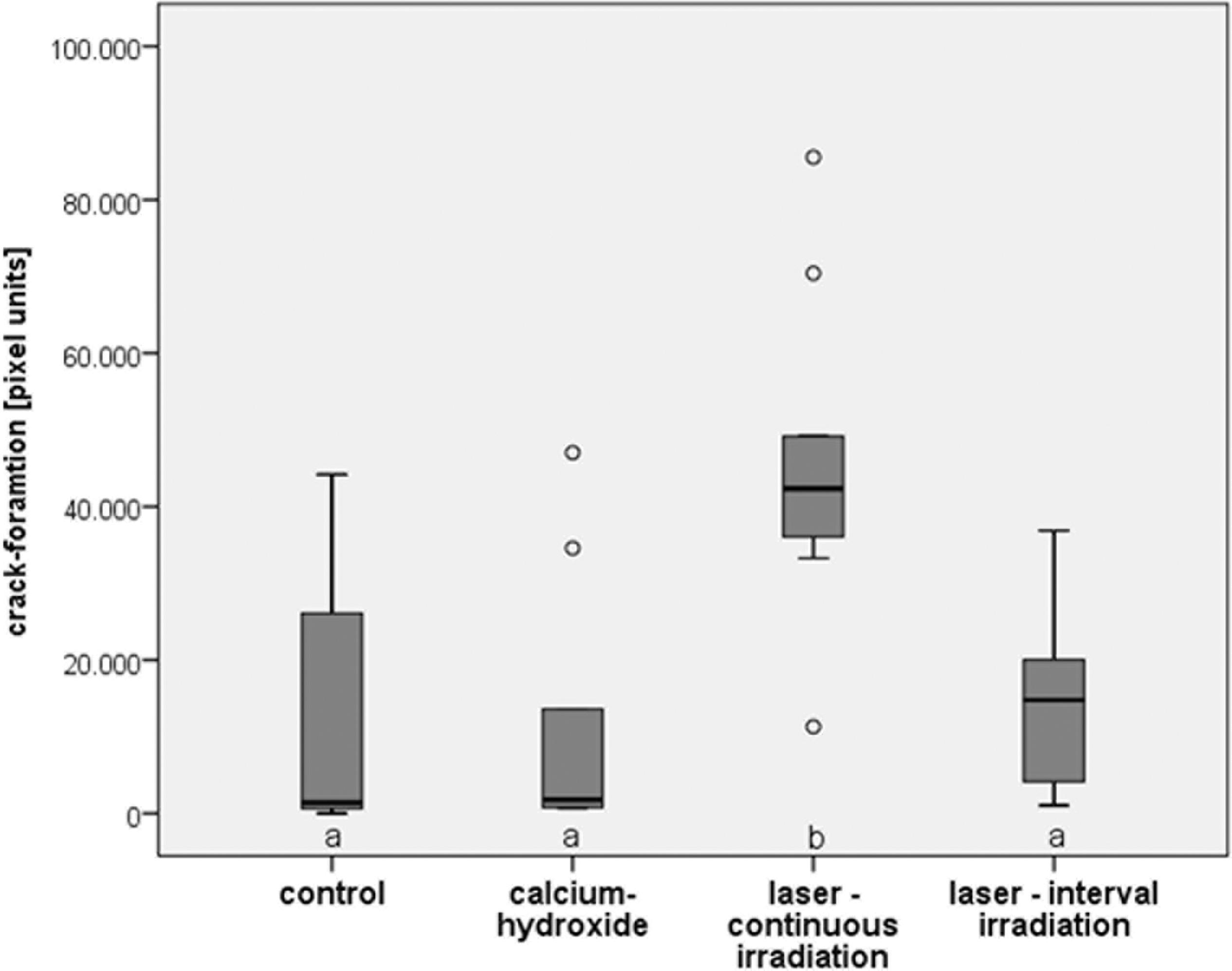
Overall crack formation in root dentin for all root sections, comprising cracks observed at baseline, after root canal preparation, and after each additional treatment procedure. The statistically significantly greatest amount of crack formation occurred after continuous laser irradiation (p < 0.05). The different letters show statistically significant differences.
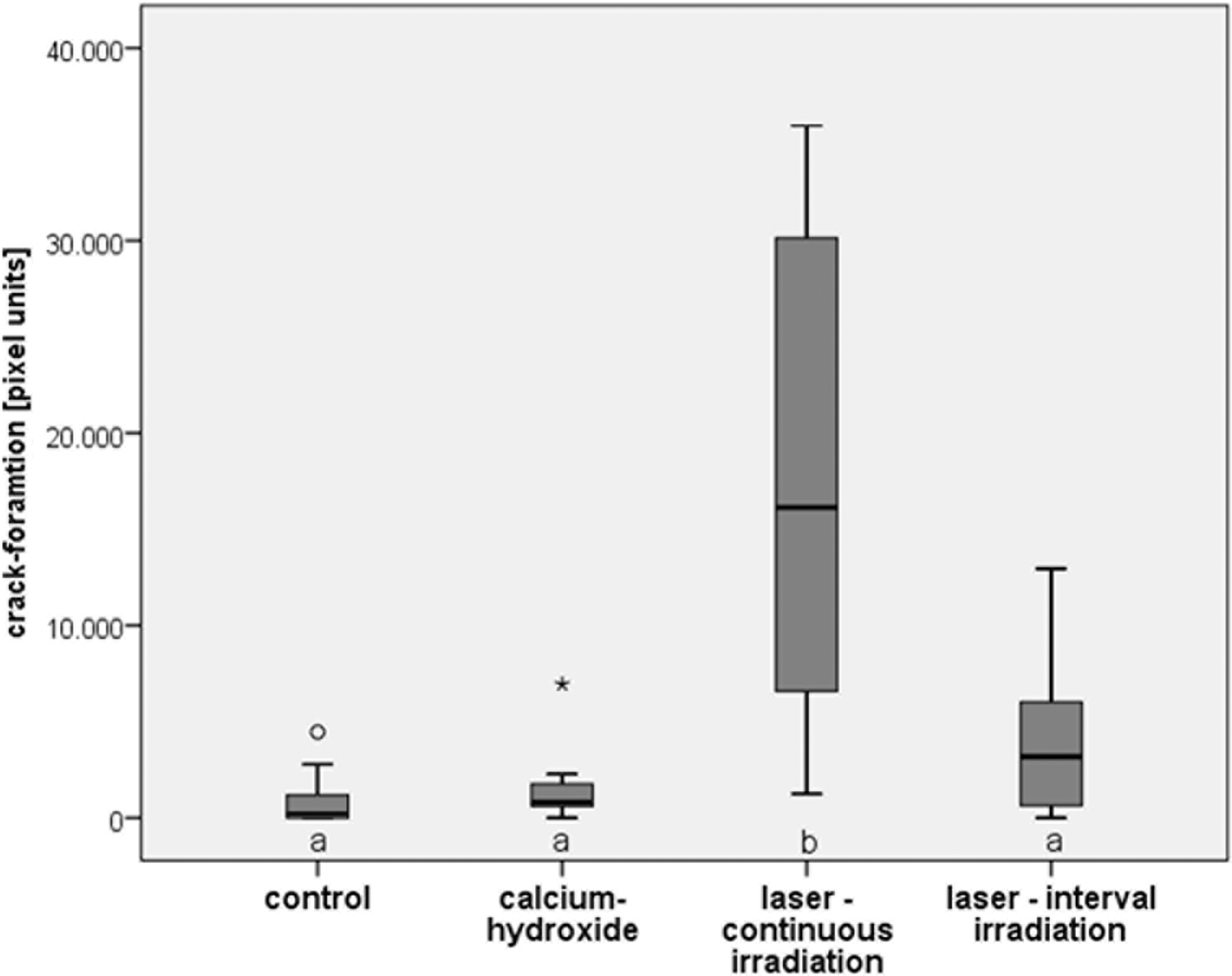
Crack formation in root dentin for all root sections caused only by each additional treatment procedure after root canal preparation. The statistically significantly largest amount of crack formation occurred after continuous laser irradiation (p < 0.05). The different letters show statistically significant differences. *Far outliers with values more than 3 times the interquartile range; °outliers with values 1.5 to 3 times the interquartile range.
Overall Crack Formation (in Pixel Units) in Root Dentin for All Root Sections, Comprising Cracks Observed at Baseline, After Root Canal Preparation, and After Each Additional Treatment Procedure
The different letters show statistically significant differences (p < 0.05).
Crack Formation (in Pixel Units) in Root Dentin for All Root Sections Caused Only by Each Additional Treatment Procedure After Root Canal Preparation
The different letters show statistically significant differences (p < 0.05).
Location of crack formation
When the coronal, middle, and apical root sections were analyzed separately, the coronal section did not show any statistically significant differences for laser irradiation in constant and interval modes (p > 0.05) (Table 4). For both the middle and apical root sections, however, laser application in constant irradiation mode resulted in the significantly largest amount of crack formation in comparison with the other groups investigated (p < 0.05). When crack formation was compared with location in the coronal, middle, or apical root sections in a single treatment group each, the statistically significantly smallest amount of crack formation was noted in the apical third for all groups investigated (p < 0.05) (Fig. 4).
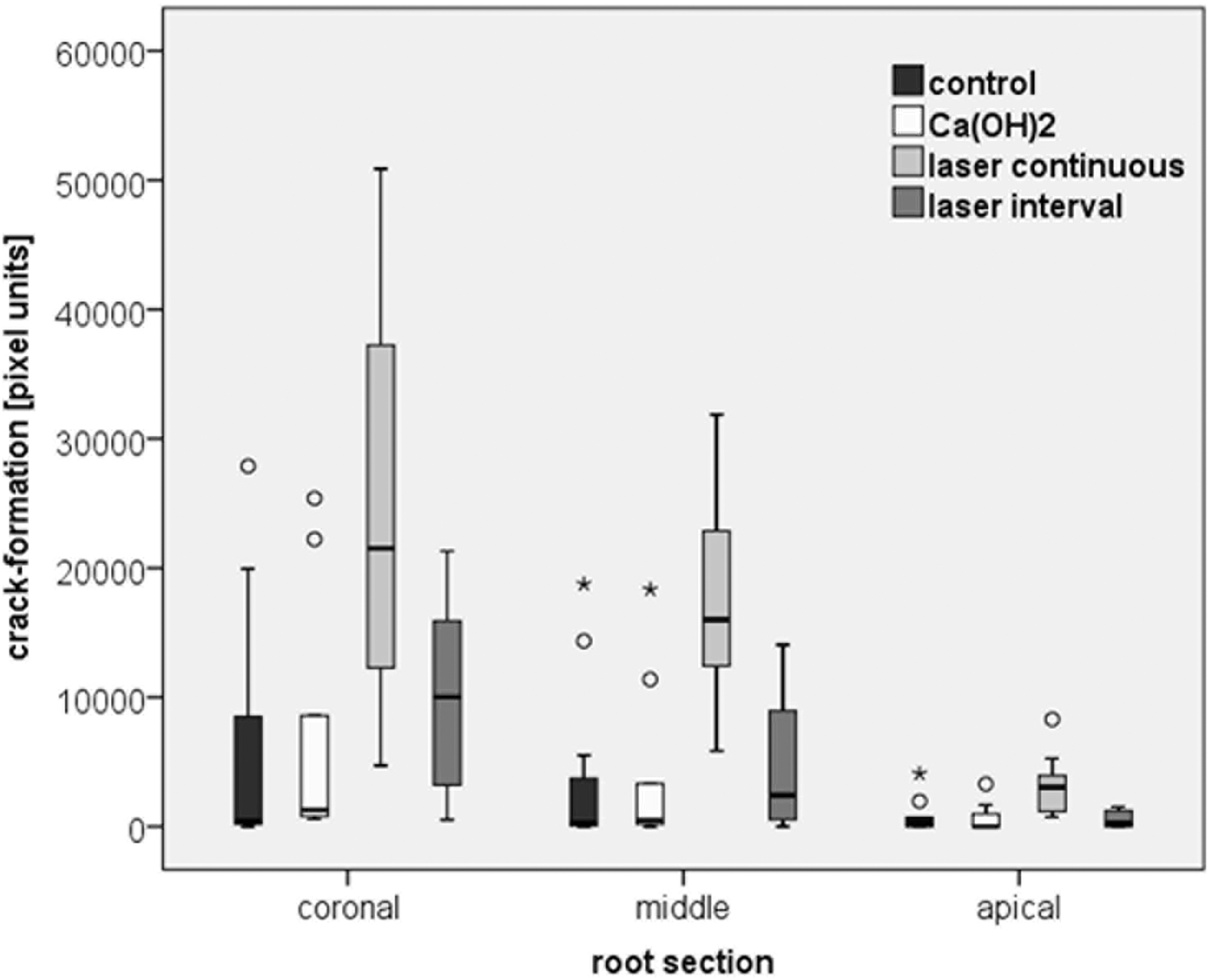
Crack formation in root dentin after continuous laser irradiation in the coronal, middle, and apical thirds. The statistically significantly smallest amount of crack formation occurred in the apical section in all treatment groups (p < 0.05). *Far outliers with values more than 3 times the interquartile range; °outliers with values 1.5 to 3 times the interquartile range.
Overall Crack Formation (in Pixel Units) in Dentin for the Coronal, Middle, and Apical Root Sections, Comprising Cracks Observed at Baseline, After Root Canal Preparation, and After Each Additional Treatment Procedure
The different letters show statistically significant differences (p < 0.05).
Discussion
The aim of this study was to investigate the influence of adjunctive dental root canal disinfection on microcracking with a 970-nm diode laser in different irradiation modes, in comparison with chemical disinfection with calcium hydroxide. The present results show that a 970-nm diode laser with the laser parameters for endodontic treatment, adjusted as described by Gutknecht et al. in the interval mode, 21 did not lead to any differences in the formation of microcracks in comparison with the control group or calcium hydroxide group. Other studies have reported an increased risk of fracture resulting from endodontically induced microcracks. 2,5,6 Since larger amounts of microcracking induced by the laser system with endodontic laser settings in the interval group do not occur, it can be assumed that the risk for later root fracture is not increased as a result of disinfection of the root canal with the laser system used, in comparison with the calcium hydroxide disinfection protocol. Since it has been shown that using a diode laser to disinfect the root canal leads to significantly greater bacterial reduction in comparison with chemical disinfection based on calcium hydroxide, 12 –15,18 the results of the present study appear to show that the disinfection protocol using a 970-nm diode laser is preferable.
Gutknecht et al. reported that the crack formation resulting from laser application in the root canal correlates with the temperature increase, and the present results confirm this view. 21 In microcracking relative to all the treatment procedures investigated, and in microcracks that arise only as a result of disinfection procedures in the root canal, the constant irradiation group was characterized by a statistically significantly higher rate of microcracking in comparison with all other study groups (Tables 2 and 3 and Figs. 2 and 3). Since the antibacterial effect of lasers is based on the thermal interaction, it might be suggested that maximum bacterial reduction can be achieved with the highest possible heat development in the root canal. 15,18 On the basis of the present study results, it can be concluded that the laser parameters recommended by Gutknecht et al. should be observed to avoid unnecessarily high dental microcracking due to excessive heat development. 21
With regard to the results for crack formation in the different root sections, the present study again confirms the finding by Gutknecht et al. that there is a correlation between microcracking and heat development. 21 It can be assumed that heat generation reaches its highest point at the location where the laser radiation hits the canal surface. This is confirmed by the statistically significant increase in microcracks in the coronal section in both laser groups. Most of the laser radiation hits the canal surface directly in this section. In the middle section, laser radiation in the constant group is still so high that significantly more microcracks arise in this group in comparison with the other groups. The deeper the laser goes in the root canal, the faster the heat is transmitted through the dental hard tissues. The fact that the fewest microcracks were induced by laser application in the apical section in both groups confirms this view. However, the study was not designed to investigate heat conduction processes in the dental hard tissues in detail (Table 4 and Fig. 4).
Various lasers are used in dentistry and endodontics like diode lasers, the Erbium:YAG laser, the Neodymium:YAG laser, the Erbium and Chromium:YSGG laser, and the CO2 laser (Table 5). 19 Most of the laser studies focusing on endodontics attempt to investigate the antimicrobial potential of lasers in the dental root canal. 19,22 –27 Concerning the formation of microcracks as a result of laser application of different laser systems in the dental root canal, just a few studies are available. This would be an interesting issue for further studies to investigate.
Lasers in Dentistry 19
How great is the risk to the longevity of a tooth resulting from microcracks that are generated by endodontic treatments in the dental hard tissue? This question has not yet been sufficiently investigated and represents an interesting topic for future research. The present results are based on the use of a 970-nm diode laser with the settings described. No statements can therefore be made regarding the amount of microcracking generated in the dental root canal with other laser systems with different parameters, which is again a topic requiring further research. Sodium hypochlorite is an alternative to calcium hydroxide for chemical disinfection of the root canal system. The impact of sodium hypochlorite to the risk of generated microcracks was not investigated in the present study. However, as all teeth in the present study were rinsed with sodium hypochlorite, the impact of the solution on microcrack formation was similar in all groups, allowing an intra-experimental comparison of the study groups.
Conclusions
The laser settings described by Gutknecht et al. for endodontic disinfection of the root canal, used with a 970-nm diode laser in interval irradiation mode, do not lead to a greater amount of microcracking in comparison with the standard chemical procedure using calcium hydroxide. On the basis of the laser settings used in this study, it can be concluded that an irregular laser irradiation should be avoided to prevent unnecessary microcracking of the root canal dentin during laser disinfection protocols.
Footnotes
Acknowledgments
The authors are grateful to Dentsply Sirona for providing the laser device used in the study.
Author Disclosure Statement
No competing financial interests exist.