
Abstract
Introduction
S
Many conservative treatments for rotator cuff diseases exist in the literature, including strengthening and stretching exercises, 9,10 progressive resistance training, 11,12 eccentric training, 13 shoulder joint mobilization, 14,15 kinesio-taping, 16,17 ultrasound, 18 transcutaneous electrical nerve stimulation 19 and shock wave therapy. 20 Pulsed Nd:YAG lasers have been used successfully in the treatment of musculoskeletal disorders. 21 The pulsed Nd:YAG laser, or neodymium: yttrium–aluminum–garnet laser, provides high-intensity laser therapy (HILT). It is a safe, painless, deep penetration method, and the short emission time and long rest periods prevent heat accumulation. 22,23
As with high-power pulsed lasers, HILT is postulated to have three main effects: photochemical, photomechanical, and photothermal. 24,25 Owing to these effects, HILT reduces pain, inflammation, and edema, thus allowing an early start for tissue healing and an early beginning for rehabilitation programs. 26 Further, the short-term effect of HILT has been proven to be an effective method for reducing pain and improving function in patients with rotator cuff tendinitis, bicep tendinitis, subacromial impingement syndrome, and frozen shoulder, 1,23,27 although there is a lack of knowledge regarding its long-term effects on rotator cuff tendinopathy. Thus, the aim of the current study was to explore the long-term effects of HILT on pain, shoulder function, and ROM in patients with rotator cuff tendinopathy.
Methods
Participants
Patients diagnosed with rotator cuff tendinopathy by a professional orthopedist were referred to the Rehabilitation Department of King Faisal Hospital, Makkah, Saudi Arabia. The mean age of the patients was 50.2 ± 3.6 years (mean ± SD).
Patient selection depended on history and examination. Patients were included if they had pain in the shoulder joint for more than 3 months; limitation of shoulder abduction; external and internal rotation; and positive results in diagnostic tests used for detecting abnormalities in the rotator cuff (Neer test, Hawkins test, Jobe test, and external rotation lag sign). Exclusion criteria involved previous shoulder surgery, neoplastic diseases, and systemic inflammatory disease (e.g., rheumatoid arthritis, shoulder calcification or osteoarthritis, the possibility of complete rotator cuff tears, neurological or structural defects affecting shoulder joint).
After first examination, all patients were provided a complete description of the treatment protocol and asked to sign written informed consent for their participation in the study and for results publication. The Departmental Council of the Faculty of Applied Medical Science, Umm Al-Qura University, Makkah, Saudi Arabia, approved the study with registration number 43409418.
Power analysis
Power analysis was utilized to determine the appropriate sample size of the study groups. G-power analysis version 3.1 was used after setting the effect size to 0.8 (large effect size depending on Cohen's d, and to determine even low differences between the study groups), high power of 0.8, and type I error (α = 0.05); a total of 52 patients were required.
Design of the study
The study design was a randomized pretest/posttest single blind. A total of 60 patients were randomly allocated to one of two groups using GraphPad software, with 30 patients in each group. Group 1 (the control group) received an exercise program for rotator cuff tendinopathy in addition to sham laser treatment of three sessions per week for 4 weeks. Group 2 (the treatment group) received HILT of three sessions per week for 4 weeks in addition to an exercise program.
Pain assessment
Pain was assessed using the standard 100 mm visual analog scale (VAS). The patients graded their pain on the VAS with 0 representing “no pain” at 1 end and 10 representing “unbearable pain,” or pain as bad as it could possibly be, at the other. 28 Pain severity was assessed by a blinded-testing therapist. Each patient was asked to indicate the level of his shoulder pain on the scale at the end of the baseline and posttreatment sessions, and at 3 and 6 months after the end of treatment.
Shoulder ROM assessment
Passive and active shoulder abduction, external rotation, and internal rotation were assessed by a blinded physiotherapist at baseline, posttreatment, and 3 and 6 months after treatment using a universal goniometer. For measuring ROM, the fulcrum of the goniometer was placed over the acromion for evaluating abduction and over the olecranon for evaluating external rotation and internal rotation, at 45° shoulder abduction and 90° elbow flexion. 29
Shoulder functional activity assessment
All patients were assessed before and after the study, and at 3- and 6-month follow-up points, for their daily activities and pain severity using the shoulder pain and disability index (SPADI). SPADI contains 13 points that utilize two scales; a five-item subscale that evaluates pain severity and an eight-item domain that assesses disability. SPADI is quick and easy to complete, scores do not alter significantly in stable subjects, and has both face and content validity for evaluating shoulder pain and disability. 30
Intervention protocol
Exercise program
ROM exercises in the form of a pendulum exercise progressed to active assisted ROM exercises with canes and active exercises in front of a mirror using opposite hands. Flexibility, postural, and strengthening exercises focused on the rotator cuff muscles using a Thera-Band and scapular stabilization exercises. Exercises were taught by a physiotherapist and participants were asked to perform the exercises daily at home. A family member confirmed that the patient performed the exercises at home.
High-intensity laser therapy
Patients in the treatment group received HILT, produced by HIRO 3 device (ASA, Arcugnano, Vicenza, Italy). The treatment consisted of initial, intermediate, and final phases. The initial and final scanning phases involved fast scanning in the initial phase and slow scanning in the final phase, over the rotator cuff muscles, the upper fibers of the trapezius, deltoid, and pectoralis major muscles, with total energy of 1000 J in each phase. In the intermediate phase, the laser probe was fixed to the predetermined trigger and tender points at 90° perpendicular to the skin with mean energy of 50 J. The total energy delivered to the subject during one session was 2050 J over three phases of treatment in ∼15 min. HILT was applied for 12 sessions in 3 sessions each week for 4 weeks. HILT was calibrated for constant output throughout the experiment at the Department of Physical Therapy, Faculty of Applied Medical Science, Umm Al-Qura University, Table 1.
HIRO 3 device (ASA, Arcugnano, Vicenza, Italy).
Outcome measures
Pretreatment assessment of the measured variables was performed at the baseline and this assessment was repeated at the end of treatment and at 3- and 6-month follow-ups. The measured variables were shoulder pain measured by VAS, shoulder function assessed by SPADI, and passive and active shoulder abduction, external rotation and internal rotation measured by a universal goniometer.
Statistical analysis
Data analyses were performed using SPSS version 20 for Windows. Power analysis and sample size calculation were performed by G-Power 3.1 for Windows, while randomization was carried out using GraphPad for Windows. Analysis of variance (ANOVA) with repeated measurements was used to compare the same group's pre- and posttreatment ROM and during follow-up periods, and Wilcoxon test was used to compare VAS and SPADI. At each measuring point, an unpaired t-test was used to compare ROM between groups and a Mann–Whitney test to compare VAS and SPADI.
Results
There were no missing data throughout the study or follow-up loss. The mean age of the study population was 50.2 ± 3.6 years (mean ± SD) with no statistically significant difference between the study groups at the baseline (p = 0.14, F = 0.011). The baseline comparison of the treatment variables showed no statistically significant difference between the study groups (Tables 2, 3). An independent t-test was performed after treatment and at 3 and at 6 months posttreatment, and showed highly statistically significant differences between the study groups in all measured ROM movements (Table 2 and Figs. 1 –5 6). Further, a Mann–Whitney U test showed highly significant differences between the treatment groups in VAS and SPADI immediately posttreatment and at 3 and at 6 months after the end of the treatment (Table 3 and Figs. 7, 8).
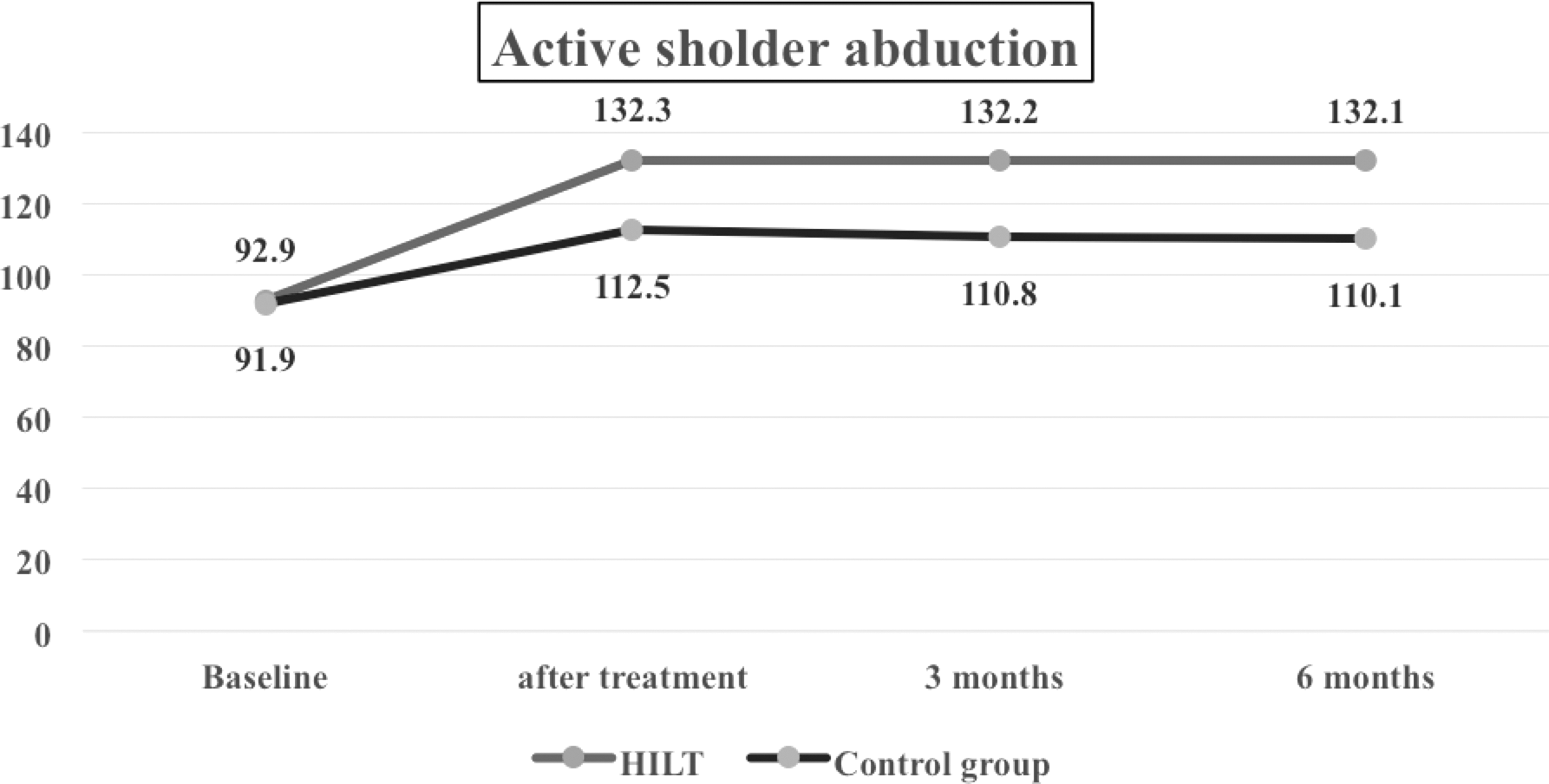
Active shoulder abduction showing the statistical difference between the study groups after treatment and during follow-up periods and the consistency of the results in the treatment group over time. HILT, high-intensity laser therapy.
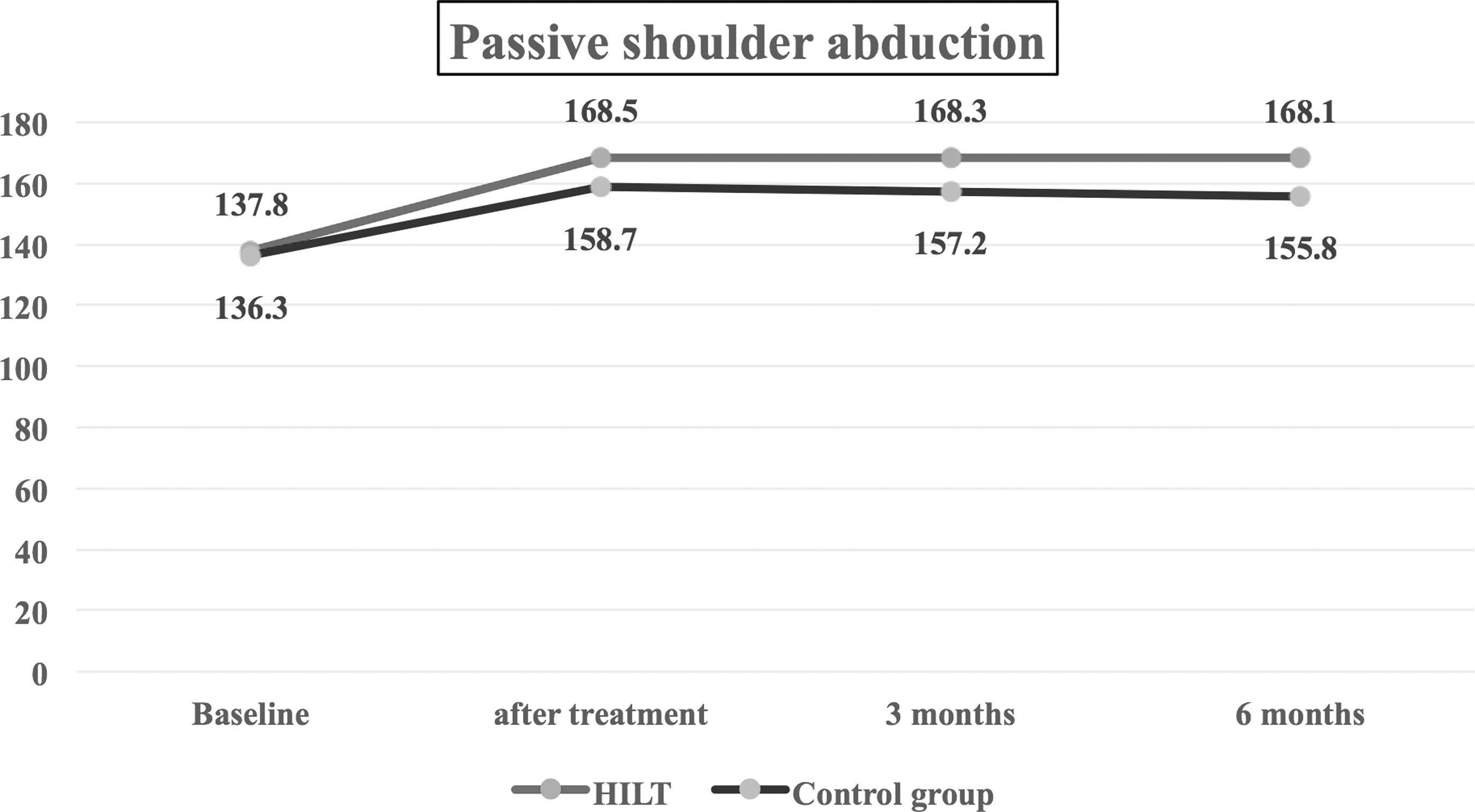
Passive shoulder abduction showing the statistical difference between the treatment groups after treatment and during follow-up periods and the consistency of the results in the treatment group over time. HILT, high-intensity laser therapy.
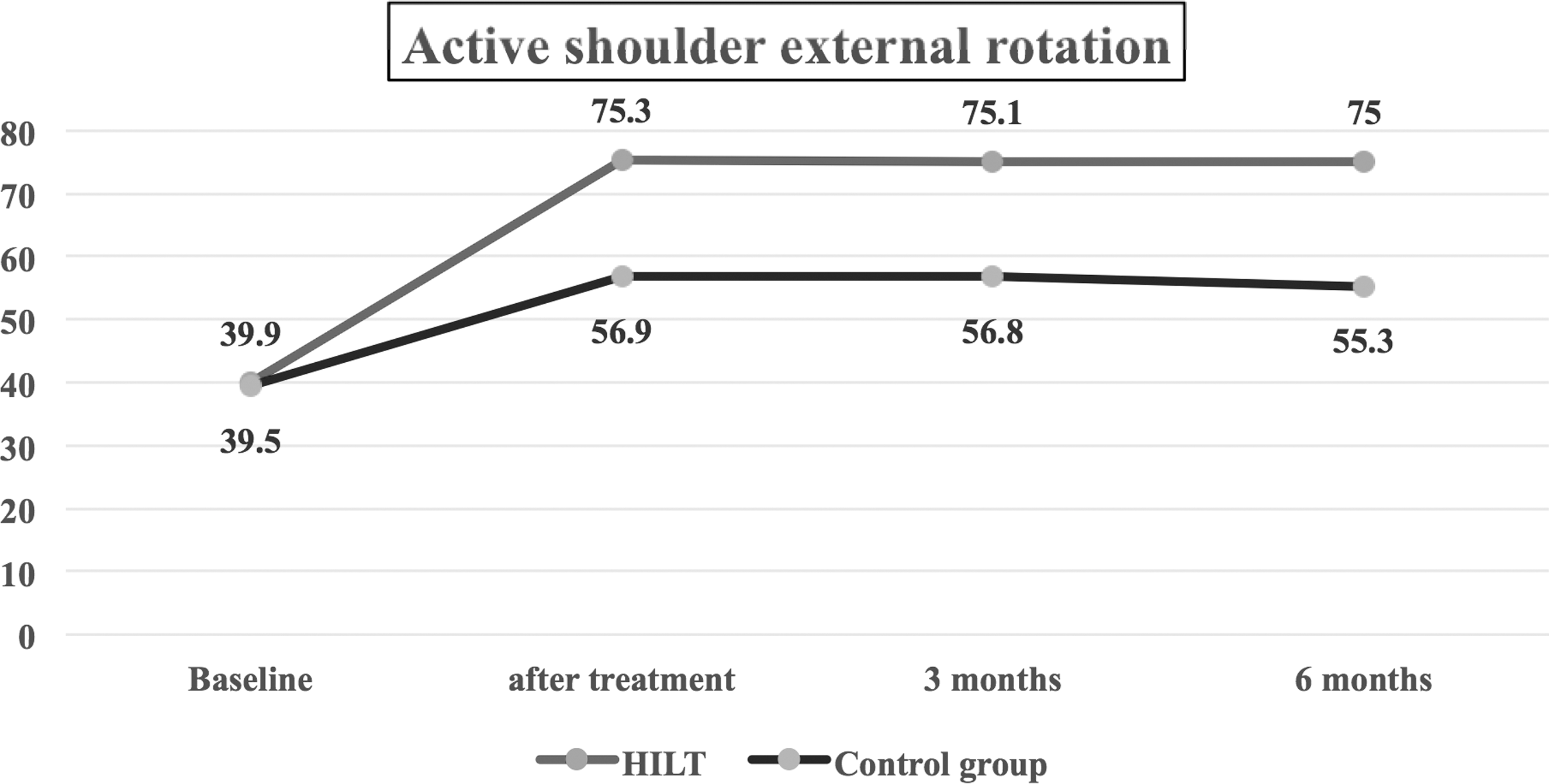
Active shoulder external rotation showing the statistical difference between the treatment groups after treatment and during follow-up periods and the consistency of the results in the treatment group over time. HILT, high-intensity laser therapy.
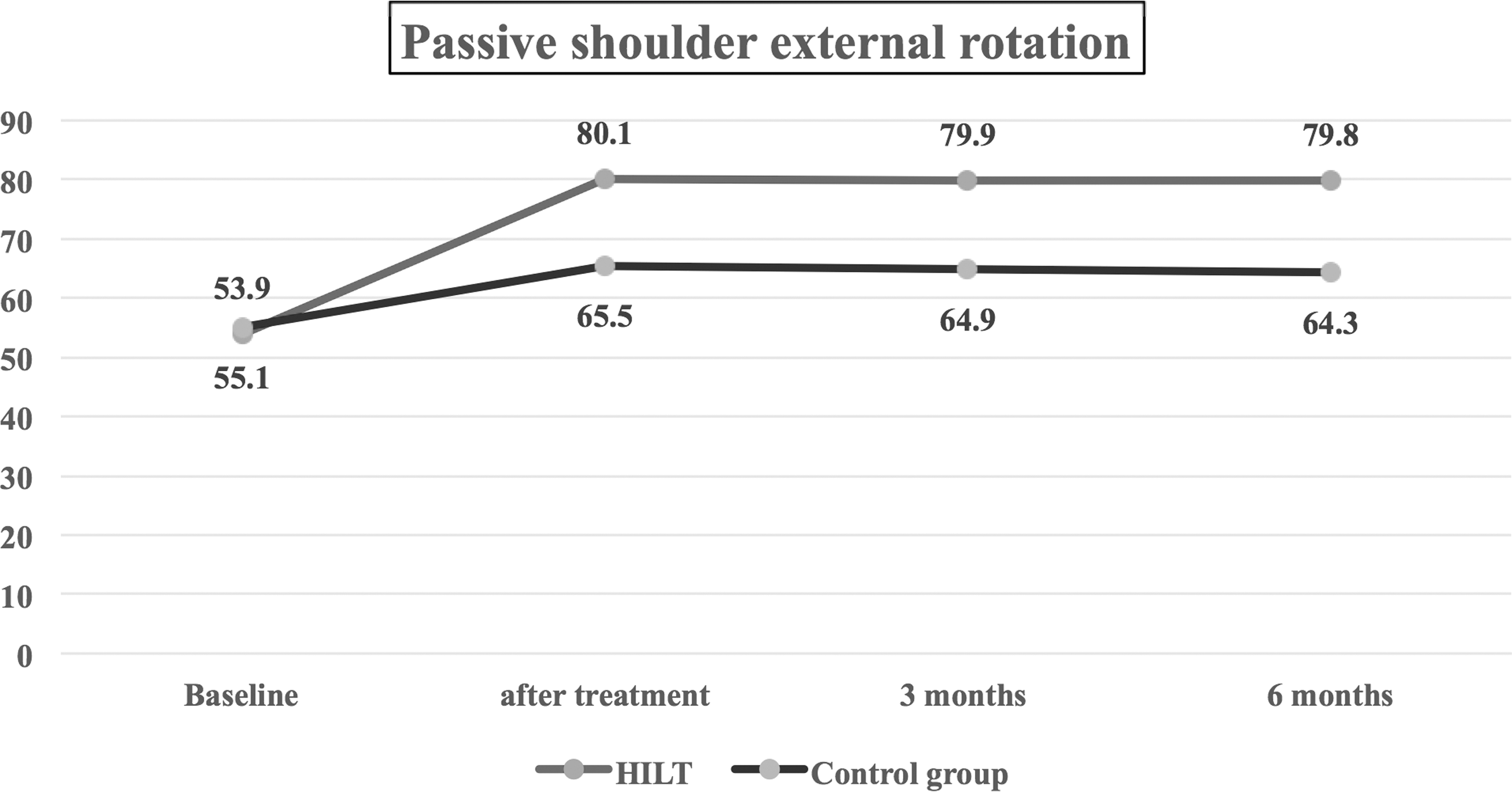
Passive shoulder external rotation showing the statistical difference between the treatment groups after treatment and during follow-up periods and the consistency of the results in the treatment group over time. HILT, high-intensity laser therapy.
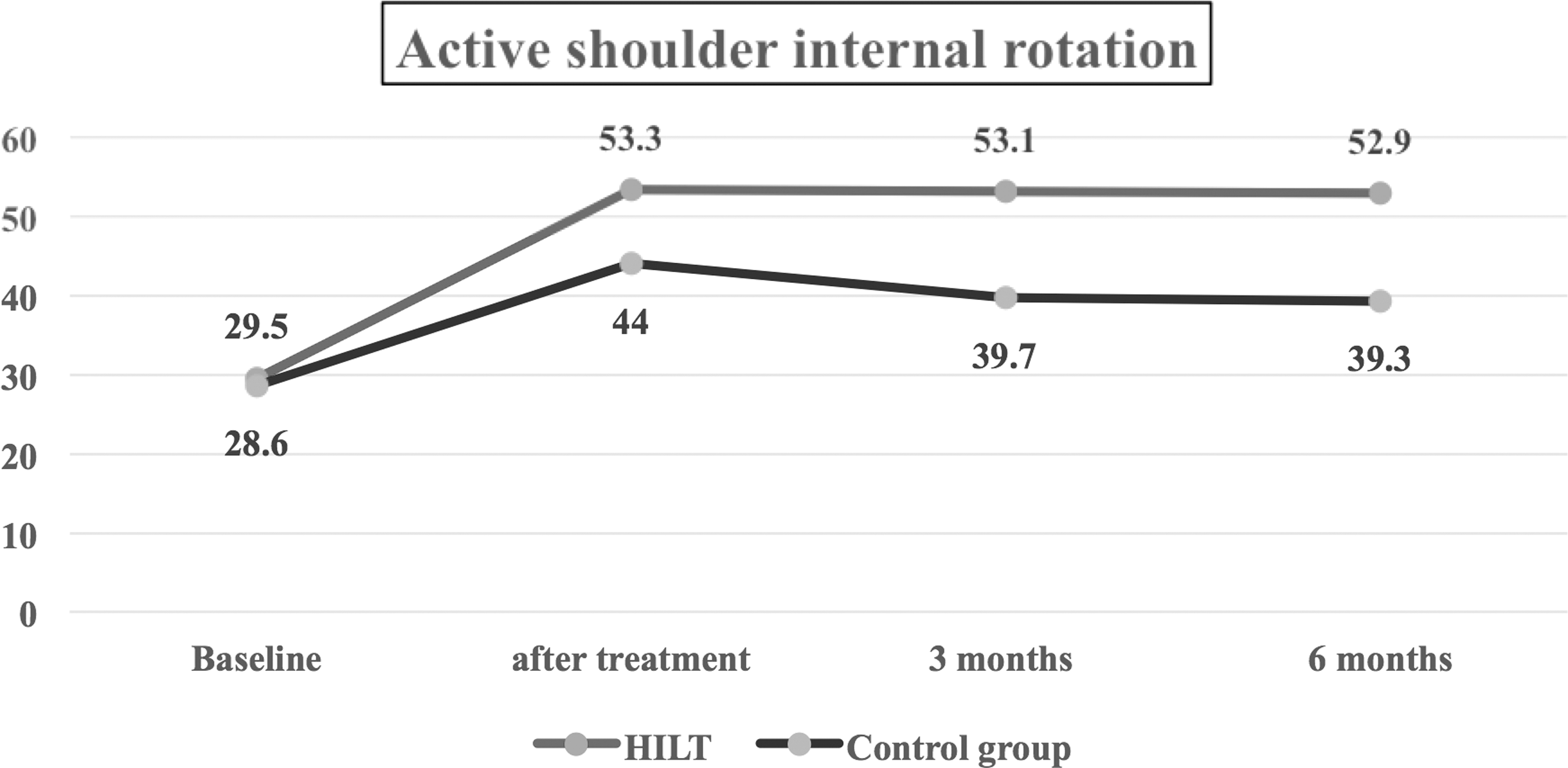
Active shoulder internal rotation showing the statistical difference between the treatment groups after treatment and during follow-up periods and the consistency of the results in the treatment group over time. HILT, high-intensity laser therapy.
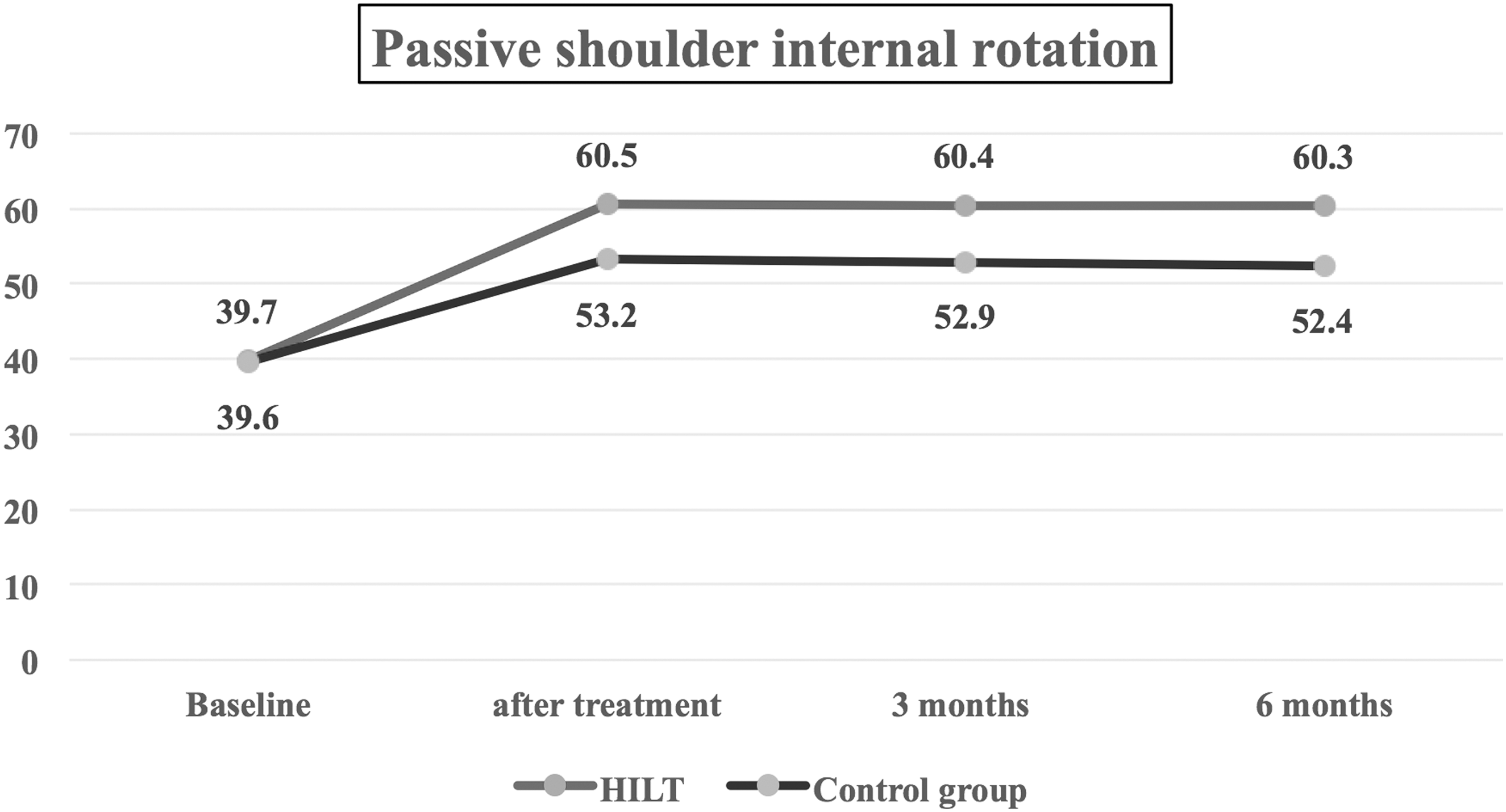
Passive shoulder internal rotation showing the statistical difference between the study groups after treatment and during follow-up periods and the consistency of the results in the treatment group over time. HILT, high-intensity laser therapy.

Visual analog scale showing the statistical difference between the study groups after treatment and during follow-up periods and the consistency of the results in the treatment group over time. HILT, high-intensity laser therapy.
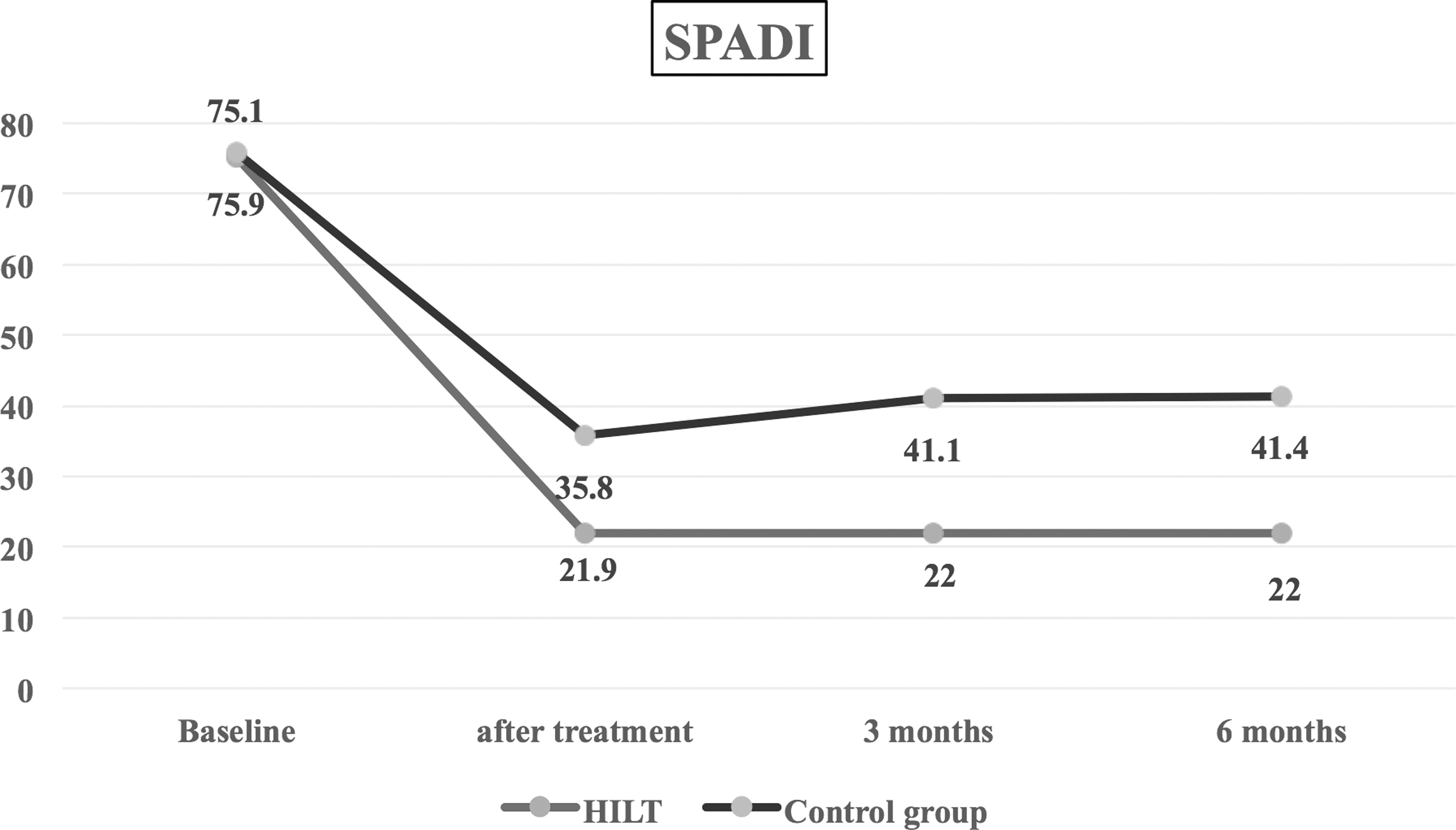
SPADI for shoulder function showing the statistical difference between the study groups after treatment and during follow-up periods and the consistency of the results in the treatment group over time. SPADI, shoulder pain and disability index; HILT, high-intensity laser therapy.
Nonsignificant difference, **significant difference.
p Value probability value.
HILT, high-intensity laser therapy.
Nonsignificant difference, **significant difference.
p Value probability value.
HILT, high-intensity laser therapy; SPADI, shoulder pain and disability index; VAS, visual analog scale.
Within-group analysis using ANOVA with repeated measurements revealed statistically significant differences between the measured ROM movements in both groups in terms of time. Post hoc tests revealed that there were statistically significant differences between baseline ROM measurements, posttreatment measurements, and follow-up measurements. Post hoc tests also revealed consistency between the results posttreatment and during follow-up, with no statistically significant difference between them in the HILT group. On the contrary, post hoc tests showed significant differences between the posttreatment ROM and each follow-up ROM measurement, and also between the two follow-up measurements in the control group (Table 2 and Figs. 1 –6).
In addition, a Friedman test showed statistically significant differences in VAS and SPADI in both study groups between measurement points. To compare two time intervals, the Wilcoxon signed-ranked test was used and revealed statistically significant differences posttreatment and during follow-up measurements in comparison with the baseline measurements, with the best improvement observed posttreatment (Table 3 and Figs. 7, 8).
Discussion
The purpose of the present study was to explore the long-term effects of pulsed Nd:YAG laser on pain, shoulder function, and ROM in patients with rotator cuff tendinopathy. The results of the current study showed great improvement in pain, function, and ROM of the shoulder joint in the treatment group and control group, with more improvement in the treatment group posttreatment and during the follow-up periods.
Low-level laser therapy is a successful method currently used in the treatment of patients with subacromial syndrome, 1 supraspinatus, or bicipital tendinitis. 31 Nowadays, pulsed Nd:YAG laser therapy, a form of HILT, is used for many different musculoskeletal conditions. It is being used to relieve symptoms associated with frozen shoulder, 32 ankle pain, 33 knee arthritis, 34 –36 and chronic lower back pain. 37
In the treatment of shoulder pain, HILT has been proven to be an effective method for reducing pain and disability after treatment 38 and at short-term follow-ups. 27 Laser therapy is commonly thought to change cellular and tissue activity, relying on the nature of the laser itself (e.g., wavelength, coherence). 39 The pulsed Nd:YAG laser has a wavelength of 1046 nm and acts in a therapeutic window that permits it to pierce deeply and extend readily within tissue, as the concentration of endogenous chromophores in the skin is too low to absorb this wavelength. 22 Laser therapy has a photochemistry effect in which light diffusion occurs in all directions as a result of tissue absorption of laser light, and this leads to enhancement of mitochondrial oxidative reaction and consequently raises adenosine triphosphate, RNA, and DNA outputs. This photochemistry effect also results in the stimulation of tissue, a photobiology effect. 22
The particular waveform of pulsed Nd:YAG laser, with a peak power of 3 kW, and the very short cycle do not allow heat accumulation in the deep tissue, but rapidly provoke deep tissue photochemical and photothermal effects. 22 These features result in greater procreation in the treated tissues with negligible histological risk, resulting in a probability of increasing healing at deep tissue level. By adjusting the HILT intensity and frequency, the photothermal effect can be coordinated for patient safety and comfort. 40,41
The anti-inflammatory, antiedema, reparative, and sedative effects of HILT are all responsible for its efficacy in the treatment of musculoskeletal disorders. 41 The sedative effect of HILT results from its ability to delay the transmission of pain impulses along pain fibers and to raise the level of morphine-mimetic substances in the tissues. 22 The treatment may also have a straightforward impact on nerve structures, which could enhance the rate of recovery from conduction block. 42 Laser treatment also enhances blood supply, vascular permeability, and cell function. 43
In the present study, the combined effect of HILT with exercise was superior to that of the placebo HILT with exercise. It has been proposed that placebo interventions are vital tools that can be used by medical researchers to complement regular treatments, and most physicians supposedly admit to their use being ethically allowable. 44 Nevertheless, the use of placebo interventions in clinical medicine remains controversial. 45
The findings of the present study are in line with results of other studies that HILT is superior to a sham laser for reducing pain and disability after treatment 38 and at short-term follow-ups in patients with subacromial impingement syndrome. 27 In addition, several studies demonstrated the positive effects of low-level laser therapy (LLLT) in the treatment of rotator cuff disorders. 1,31,46,47
On the contrary, Kim et al. 48 found that although their HILT group had a lower pain VAS score at 3 and 8 weeks, no statistically significant difference in the VAS was detected between the groups at the 12-week follow-up. Further, no statistical difference in the ROM or the satisfaction VAS was observed between the two groups at serial follow-ups in patients with frozen shoulder. 32 Relatedly, other research showed no difference between LLLT placebo laser therapy in combination with superficial cold and progressive exercises 49 or in combination with home exercises. 50 The HILT used in the present study differed from the LLLT in these trials in wavelength, power density, fluency, frequency, dosage, intensity, and penetration, which could explain the conflicting results.
The current results prove that exercise therapy has a positive effect on improving pain, function, and ROM of the shoulder joint, which is consistent with data that exist in the literature. It confirms that a combination of active exercise therapy with HILT is of clinical significance for improving symptoms associated with rotator cuff tendinopathy and this positive impact lasts for 6 years.
A simple 6-week exercise program intended to increase the rotator cuff muscle strength and elasticity of the posterior shoulder capsule, and encouraging upper thoracic extension and a retracted head posture may result in better muscle and force, and in pain reduction, in patients with shoulder impingement. 51
Conclusions
A pulsed Nd:YAG laser is a more valuable physical therapy approach for patients with rotator cuff tendinopathy in combination with exercise for pain, function, and ROM, than a sham laser with exercises.
Footnotes
Author Disclosure Statement
No competing financial interests exist.