
Abstract
Objective:
This study investigated light emitting diode (LED) treatment for patients with melasma on darker skin types.
Background:
Melasma is a common disfiguring skin condition in women which is difficult to treat and is refractory. The cause of melasma remains unclear.
Methods:
In this study, 60 female participants aged between 25 and 60 years, who presented with melasma, were enrolled (n = 39.85). They were purposely assigned to two groups according to their skin types. Both groups received a total of 36 LED light treatments over a period of 9 months.
Results:
Both subjective and objective results indicated a significant improvement of melasma. Statistical analyses revealed significant improvements in both groups.
Conclusions:
The results of this study suggest that LED is effective in managing melasma. These results will provide a basis for future therapeutic use of phototherapy to improve melasma.
Introduction
M
Being a multi-faceted skin disorder, melasma has resulted in a plethora of treatment modalities. 7 Treating melasma of skin types V and VI is challenging and often results in poor prognosis. 8,9 Most documented attempts have primarily relied on the use of invasive therapy, drugs, and creams which have been found to produce suboptimal results and undesirable side effects and risks. 8,9 Despite numerous attempts to resolve the problem, there is still uncertainty about treatment when dealing with skin types V and VI.
Toward addressing the problem, the study investigated the use of Omnilux™ light emitting diode (LED) as an alternative treatment modality for melasma on patients with skin types V and VI. LED is a quasi-monochromatic, nonlaser light which stimulates the cells athermally, and it is currently used effectively in a variety of skin ailments and abnormalities, including acne, skin rejuvenation, photorejuvenation, certain superficial skin cancers, cellulite reduction, hair stimulation, pain relief, and wound healing. 10 –14 It is based on the principle called the “by stander effect.” 15
Materials and Methods
Female participants between the ages of 25 and 60 of skin types V and VI who presented with facial melasma were enrolled into the study. A written consent was obtained from all willing participants. The exclusion criteria were as follows: Patients under dermatological treatment for the past 6 months, use of corticosteroid treatment, tretinoin or use of hydroquinone or any prescribed or over-the-counter skin lightening creams, hormone therapy, pregnant, breast feeding, sun bathing, on phototoxic drugs, medical history of epilepsy induced by the strobe light effects and/or idiopathic photophobia.
The protocol for this study was approved by the University of Johannesburg Academic Ethics Committee (AEC 01-05-2014) and the Higher Degrees Committee (HDC 01-05-2014). The study was conducted on participants who were purposely assigned to two equal groups (n = 30 each group): group A (skin type V) and group B (skin type VI). The study was conducted at an aesthetic laser clinic, LaserTouch at Life Bedford Gardens Hospital in Bedford View, Johannesburg.
After recording the participant's medical history and demographics, the face was cleansed. Melasma Severity Melasma Area Severity Index (MASI) was measured and scored accordingly. MASI measured the darkness of melasma (D) when compared with the normal skin on a scale of 0–4. It also measured the homogeneity of hyperpigmentation (H). To measure any possible visual difference, Visia® complexion analysis, a computerized pictographic technology was used to capture images. Skin punch biopsies were harvested on the area of most involvement after which they were sent for melasma histology investigations. Melasma Histology Grading Scale (MHGS) evaluated the difference in deposition of pigment on the skin by numbering the pigment globules and the intensity of pigmentation in the zones of pigment in the skin biopsy histology. Numerical values scoring the pigment globules and the pigment intensity were interpreted as follows: 0 = normal, 1 = slight, 2 = moderate, and 3 = severe.
Eye protection protocol for administering the light therapy was observed (Fig. 1). A photorejuvenation protocol was followed for irradiation. 16 Participants in both groups attended a total of 36 LED irradiation treatments over a period of 9 months. LED 633 nm light treatment was followed by an 830 nm treatment 2 days later for a period of 12 weeks, then once a month for 6 months. Each treatment session was preset at 20 min. In this study, LED Omnilux was used. Its characteristics as well as treatment parameters and irradiation protocols are described in Table 1.

Illustration of Omnilux Medial LED eye protection and positioning of the treatment head before irradiation. LED, light emitting diode.
Adapted from Reference 16 . Manufacturer: Phototherapeutics model designed from Manchester Institute of Science and Technology.
Unit dimensions: H × W × D.
Head dimensions: L × W.
LED head active dimensions: L × W.
LED, light emitting diode.
After completion of the study period, participants were asked to evaluate if they perceived any difference. Numerical values were given where 1 = Improvement (excellent), 2 = Improvement (good), 3 = Improvement (fair), 4 = Improvement (poor), 5 = No Improvement, and 6 = Worsening.
A plastic and reconstructive surgeon and a pathologist performed all assessments and measurements which were taken at baseline and at completion of the study period. Statisticians from STATKON, University of Johannesburg's Statistics Department, performed statistical analysis. All statistical analyses were completed at the 95% level of significance (α = 0.05). If the p-value as reported was <0.05, a statistically significant result was declared.
Results
Study population consisted of 60 female participants of skin types V and VI ranging from 26 to 57 years of age. The mean age of participants was 39.85 years, maximum age was 57, and minimum age was 26 with a standard deviation of 8.787. Although groups had a similar ethnic distribution, black participants were more 35 (58.3%), followed by Indian 14 (23.3%), and then colored 11 (18.3%). Most participants (30%) reported to have noticed melasma after sun exposure. Overall, unknown causes (26.7%) and pregnancy (26.7%) were considered as the main causes of melasma. Most participants presented with centrofacial pattern, 28 (46.7%), followed by those with malar pattern, 20 (33.3%), and then mandibular pattern, 12 (20%). Study findings indicated that 42 (70%) of total participants did not use sun protection as they had no significant reason for its use. However, 18 (30%) used sun protection daily as they understood the importance of its use.
Statistical measurements
The Kolmogorov–Smirnov test (a nonparametric test of the equality of continuous, one-dimensional probability distributions used to compare two samples with a reference probability distribution) was used. As most variables were not normally distributed, nonparametric test (Wilcoxon Signed-Ranks Test) was used to perform intragroup analysis, whereas a Mann–Whitney U test was used to perform intergroup analysis.
MASI—intragroup
The results of the Wilcoxon Signed-Ranks Test shown in Table 1 indicate that there was a statistically significant difference in the MASI scores before (MASI_Bef) and after treatment (MASI_Aft) as shown by the p-value of 0.000 < 0.05 level of significance (Table 2).
MASI, Melasma Area Severity Index.
Wilcoxon Signed Rank Test.
Based on positive ranks.
MASI—intergroup
A Mann–Whitney U test was conducted to compare the MASI scores for skin types V and VI. Table 3 indicates a statistically significant difference between skin types V and VI in MASI scores before treatment indicated by a p-value of 0.013 at a significance level <0.05. It is also shown in Table 2 that there was no statistically significant difference in MASI scores recorded after treatment between skin types V and VI as indicated by a p-value of 0.994 at >0.05 significance level.
Grouping variable: group.
Melasma Histology Grading Scale
Study findings in Tables 4 and 5 reveal that there was a statistically significant difference in the MHGS scores before and after treatment as shown by a p-value of 0.000 at <0.05 level of significance.
Patient Self-Evaluation Scale
Upon self-evaluation (Self Ev) at completion of the study, all participants (100%) indicated some difference in melasma. Having established that most participants noticed a remarkable difference in the treatment of melasma, it was important to check how many participants with skin types V and VI noticed such differences by means of a cross-tabulation analysis (Table 6).
Self Ev, self-evaluation.
Having recognized that skin type V participants considered themselves to have improved much better than skin type VI participants, it is ideal to analyze if there is an association between skin type and perceived improvement in the treatment of melasma. Chi-square test of independence will be conducted to test for such association. According to Table 7 below, it is evident that there is a statistically significant association between skin type and perceived improvement in the treatment of melasma as the p-value = 0.026 at <0.05 significance level.
0 cells (.0%) have expected count <5. The minimum expected count is 5.50.
Participants with skin type V had a perceived mean of 5.03, and participants with skin type VI had a perceived mean of 4.20. These results corroborate with what is revealed by the cross-tabulation analysis that skin type V participants consider themselves as having noticed excellent and good improvement, respectively, more than those with skin type VI.
Visia complexion analysis and histology images
Both pictographic data showed significant improvement. There was a notable decrease in melasma intensity and pigment granules count in melasma histology images when compared with baseline measures (Fig. 2). Visia complexion analyses also showed significant improvement (Figs. 3 and 4).
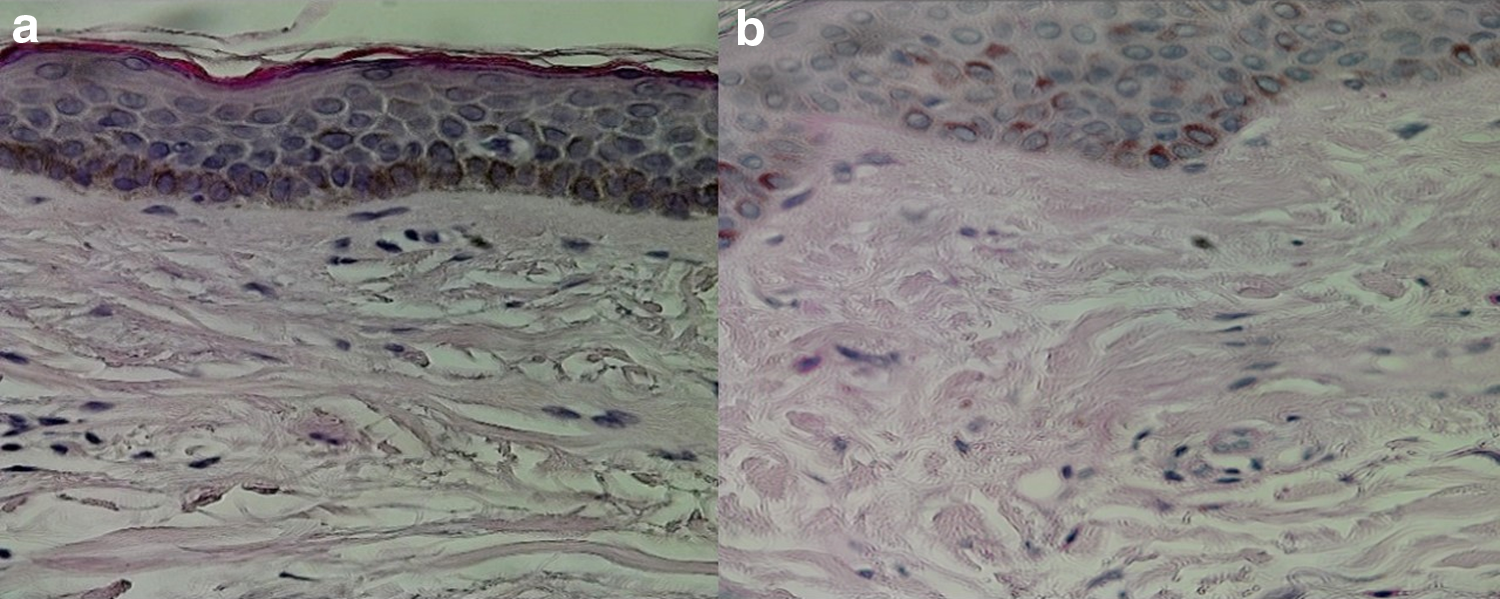
Skin type V melasma histology images illustrating comparison of skin biopsy images at baseline (
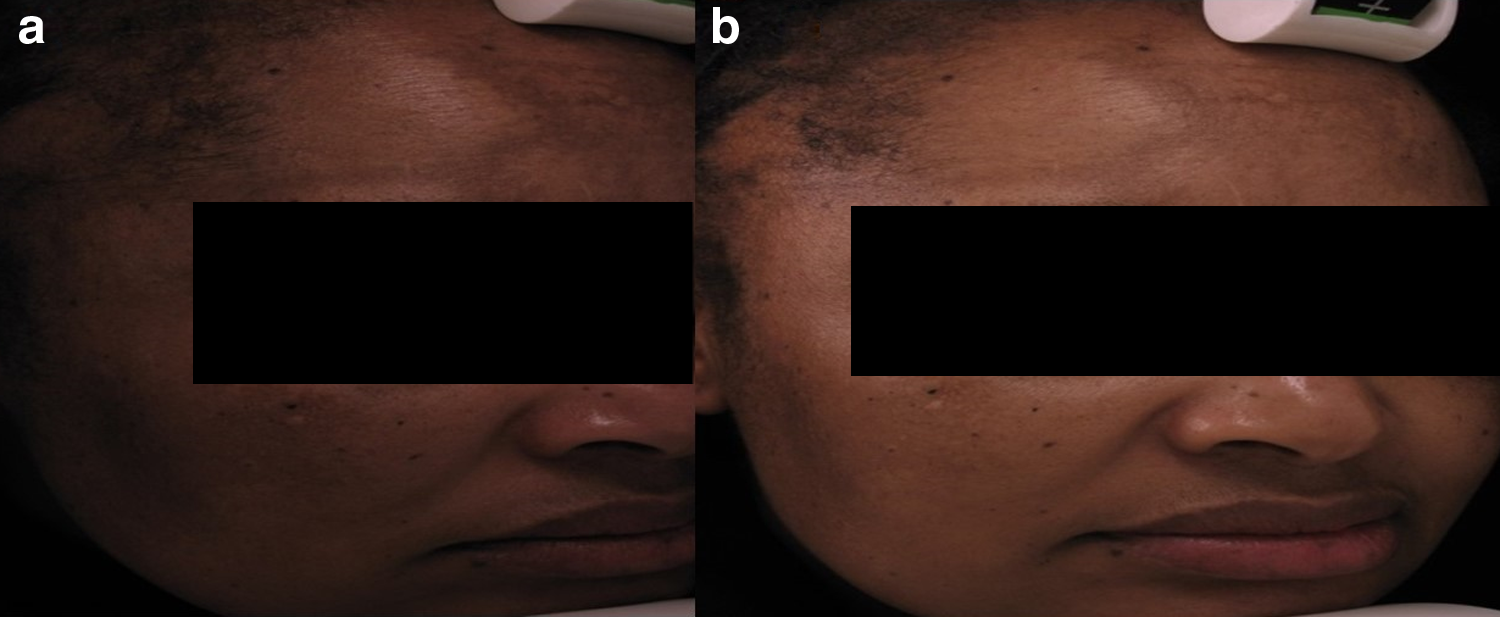
Illustration of pictographical responses from skin type V captured from the Visia® complexion analysis. Images captured at baseline before the first session (
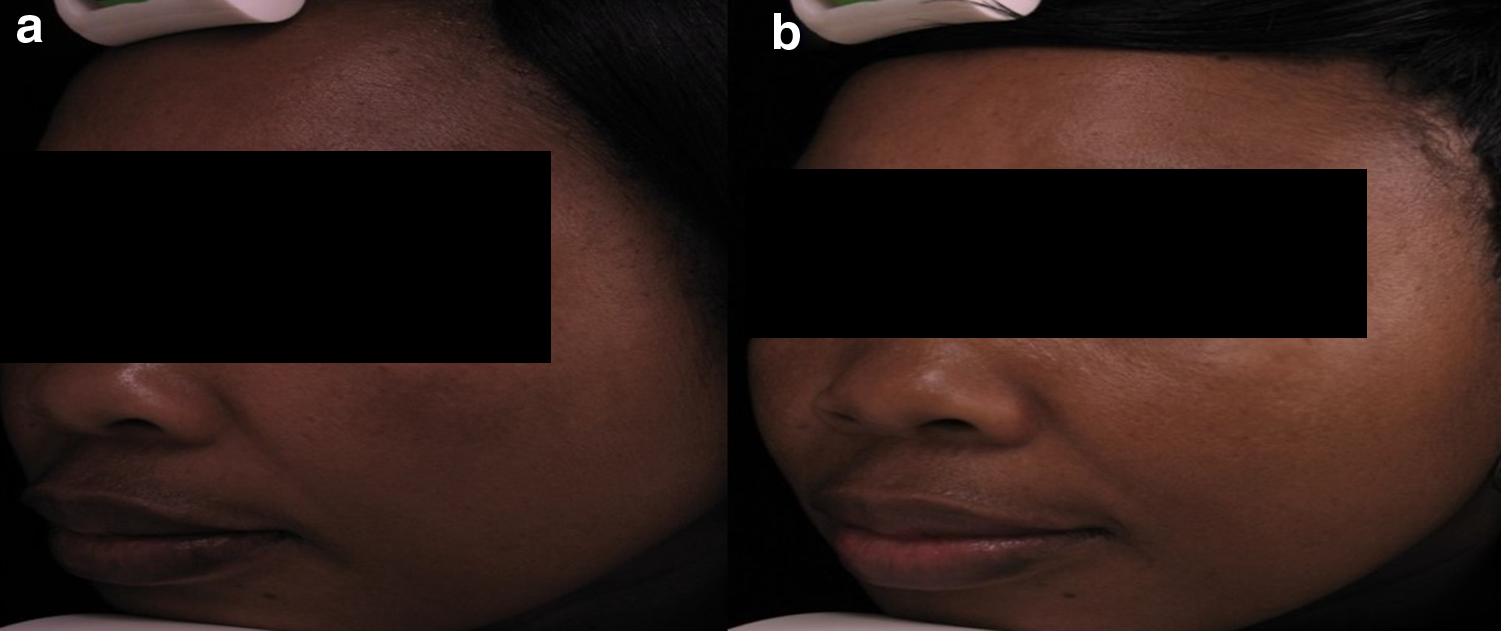
Illustration of the left malar pictographical responses from skin type VI captured from the Visia complexion analysis. Images captured at baseline before the first session (
Discussion
Only adult female participants (26–57 years) were enrolled into the study. Their mean age in this study was 39.85. This was similar to the study performed by D'Elia et al., 17 where the mean age of participants with melasma was 39. Yalamanchili et al. 18 reported a mean age of 37 concurring with KrupaShankar et al., 19 who also reported a similar mean age of 37.2 in their study. However, Leeyaphan et al. 20 reported a higher mean age of 47.8. Another study in Singapore reported an average mean age of 42.3. 21 This could be due to a large number (1169) of participants in their study. Since the incidence of melasma is more prevalent among females, this study only recruited female participants. 6,22 Although melasma is known to develop over time, 23 –25 it can start from a young age as well. 26 Men also get affected by melasma; hence recent studies are seeking to address melasma in men. 7,19,26,27
In this study, ethnicity was considered an important variable as the study pursued treatment for darker skin phototypes. Ethnicity association is also cited in the literature. 17,19,28 –34 As there has been paucity of data on studies performed with black skin phototypes, recent literature has embarked on inclusion of black skin types as well on melasma investigations. 35 –38 Given the history of South Africa, dark-skinned women were often perceived as agricultural workers or maids who consequently could not afford office work away from the sun. 39,40 According to the literature, it is evident that melasma worsens after exposure to heat conditions. 41 –44 In recent times, skin treatment has become more common and requires more effective treatment interventions for all skin types. 45 –47
In this study, the most common melasma distribution was centrofacial. This finding concurs with most other studies investigating facial melasma. 19,22,26,48 However, studies in Singapore and South India have observed that malar distribution was the most common. 21,49 This variation could be due to regional or environmental differences. A greater percentage of participants in this study could not account for what caused their melasma. However, all participants in this study (100%) indicated that melasma had developed over time. This association has been found with most documented studies in melasma where the literature cites unknown causes and acquired. 22,31,44,48,50 –52
Similar to the findings of this study, previously conducted studies have demonstrated a greater correlation between hormonal changes and occurrence of melasma. 26,19 Some studies argue that hormones do not have a significant contribution to melasma. 53,54 However, Achar and Rathi 26 found an association between thyroid dysfunction and melasma.
The majority of participants in this study (42 of 60) were not aware of irreversible photodamage and did not use sun protection. This finding brings about an opinion that maybe darker phototypes regard themselves as being free from sun damage given their darker skin phototypes which do not show immediate photodamage. Another argument could be related to sociopolitical issue. Explicably, most people in South Africa have been historically disadvantaged by racial segregation, and they prioritized matters relating to their survival, maybe putting no effort to other facets of their existence such as skin care. 39,40 The use of skin care cosmetics would have been regarded as taboo and a waste of scarce financial resources.
Tropical climates and heat have been cited to aggravate dyschromias. 41 –44,51,55 –58 South Africa presents with very hot summer climatic conditions that often exceed and reach 32°C reaching close to 48°C, 57 and therefore daily use of sun protective measures is a necessity. Safe sun protective measures are encouraged rather than complete sun avoidance. Inadequate sun exposure has been indicated to cause depletion of vitamin D which, in turn, leads to altered DNA methylation leading to death. 59,60 Sun protection should form part of basic skin care routine for all people. A good sun protection should have a broad spectrum and also have an ability to protect from the harmful short wavelengths. 35,61 Additional sun protective measures should include limited time outdoors, and the use of protective clothing and hats.
MASI scoring is widely used when investigating hypermelanosis skin concerns. 7,18,20,62 In this study, at baseline the MASI mean was 40.66 against 26.85 at the completion of the study period. This finding suggests a statistically significant difference in MASI; however MASI scoring of melasma poorly represents the severity of the disease as the nose is included as part of the cheek area. 63,64 To overcome MASI scoring limitations, Melasma Severity Index (MSI) score is the newly proposed melasma grading score. It is calculated by multiplying the area of involvement with the square of pigmentation. 63 The formula is as follows:
MSI = 0.4 (a × p2) l + 0.4 (a × p2) r + 0.2 (a × p2) n. In the formula, a stands for area of involvement, p for severity of pigmentation, l for left face, r for right face, and n for nose.
Comparison of MHGS revealed a notable difference in melasma. At the follow-up session, melasma deposition was observed as being less compared with baseline grading (Table 5). Recent studies have also found the difference in melasma when comparing histology findings. 43,44 In this study, an independent histopathologist evaluated and graded the difference in the appearance of melasma in the histology micrographs. A comparison was made between baseline and post-treatment histology micrographs. The use of an independent specialist is a common practice in skin care studies when evaluation of results is needed. 52,65 –69
Upon completion of the treatment period, participants were asked to respond to their perceived response of the treatment through Self Ev scale. All participants (100%) from both skin types showed improvement in the appearance of melasma (Table 6). Self Ev is a common practice in skin care studies. 6,10,67,70 –72 The results of the Self Ev scale concurs with the images from the Visia complexion analysis as they revealed a significant visual improvement of melasma from both skin types. Most studies use Visia for pictographic data owing to its reliability. The use of Visia complexion analysis in this study to collect visual data concurs with most melasma studies. 73 –76
It is noteworthy that the Visia Complexion Analysis equipment though accurate is inadequate for use in all skin types. In participants of dark skin phototypes, there is a lack of contrast, and therefore hyperpigmentary disorders and sun damage are not discernible on UV-detecting examination. 77 –80 It is important that skin diagnostic tools are manufactured, so that they can be beneficial to all skin phototypes.
Comparison of histological examination of the skin biopsies showed significant decrease in pigment granules and intensity at completion of the treatment (Fig. 2). Although this study observed histology changes, it was however limited to investigating cellular activity due to the laboratory equipment insufficiency.
Conclusions
In sum, this study demonstrated the effectiveness of LED (633 and 830 nm) on melasma when dealing with skin types V and VI. This was statistically demonstrated for both the subjective and objective measurements. No side effects were reported by the participants during the study period. This study provided evidence that LED treatment for melasma is effective, safe and causes no side effects when treating darker skin types. Use of latest measuring scales is highly recommended in future studies.
Footnotes
Acknowledgments
We are indebted to LaserTouch and its staff for use of its equipment during the study period and to Dr. Harry from Lancet Laboratories for his expertise in histopathology. This work is based on the research supported by the South African Research Chairs Initiative of the Department of Science and Technology and National Research Foundation of South Africa (Grant No. 98337).
Disclaimer
The material in this article, submitted to Photomedicine and Laser Surgery, has neither been published, nor is it being considered for publication elsewhere.
Author Disclosure Statement
No competing financial interests exist.