
Abstract
Objective:
Laser-assisted paraspinal microdiscectomy for far lateral lumbar disc herniation (LDH) enables direct access to the foraminal or far lateral zone with minimal tissue injury and preserves facet joints, thereby preventing postoperative segmental instability. We demonstrated the clinical outcomes of this technique and discussed the pros and cons of laser use in lumbar disc surgery.
Background:
The microdiscectomy technique for L5-S1 far lateral zone may be difficult due to the limited surgical field with narrowed disc space, hypertrophied facet, and sacral ala. Thus, we used carbon dioxide (CO2) laser for sophisticated decompression.
Methods:
Eighty-four patients who were treated with microdiscectomy for far lateral LDH at the L5-S1 level were evaluated. Among them, 40 patients were treated using CO2 laser-assisted microdiscectomy, and the remaining 44 patients using conventional microdiscectomy. Perioperative and postoperative data were compared between the two groups with 2 years of follow-up. Clinical outcomes were assessed using the visual analog scale (VAS), Oswestry disability index (ODI), and modified Macnab criteria.
Results:
VAS and ODI significantly improved in both groups. An excellent or good outcome was rated in 80% and 77.3% of the laser and conventional group, respectively. There was no significant difference in global outcomes. However, hospital stay and time to return to work were significantly shorter in the laser group (p < 0.05).
Conclusions:
CO2 laser-assisted paraspinal microdiscectomy is effective for treating far lateral LDH. The pinpoint laser scalpel enables delicate and complete decompression in a limited surgical field with minimal tissue trauma.
Introduction
F
Since Reulen 9 and Wiltse and Spencer 10 first reported a microdiscectomy technique via the paraspinal transmuscular approach, it has been used as an effective surgical treatment option for far lateral LDH. 11 –17 This technique enables direct access to the foraminal or far lateral zone with minimal tissue injury and preserves facet joints, thereby preventing postoperative segmental instability or the need for further fusion surgery. 17,18 However, postoperative leg pain and dysesthesia caused by incomplete decompression or excessive neural manipulation of the foraminal or far lateral LDH have been commonly reported. 11 –17 This problem is more prominent in the L5-S1 far lateral zone because of the peculiar anatomical characteristics such as its narrow passage, longer foraminal zone, and more prominent crowding. 19,20
A variety of laser beams have been used to remove disc material or osteophytes and reduce intradiscal pressure via vaporization. 21,22 The microscopic carbon dioxide (CO2) laser has also been applied in minimally invasive spinal decompression under microscopic visualization. 23 –27 Lee and Lee reported laser-assisted microdiscectomy for far lateral LDH. 26
To our knowledge, there has been no study to evaluate the effectiveness of laser surgery for far lateral LDH compared to the conventional microdiscectomy technique. Here, we compared the clinical characteristics and surgical outcomes of far lateral LDH between laser-assisted microdiscectomy and conventional microdiscectomy groups and discussed the benefits of laser use in paraspinal lumbar microsurgery.
Materials and Methods
Patient population
Eighty-four consecutive patients with symptomatic far lateral LDH at L5-S1 were treated by the authors from January 2012 to November 2014. Patients were prospectively entered into the clinical database and their records were retrospectively reviewed. The study was approved by the institutional Ethical Committee.
The inclusion criteria for this study were (1) far lateral LDH at L5-S1 level as demonstrated on both computed tomography (CT) scan and magnetic resonance imaging (MRI), (2) radicular symptoms consistent with the radiological findings, and (3) failed conservative therapy of at least 6 weeks or symptom deterioration to the extent of being unbearable. Patients with segmental instability, spondylolisthesis, concomitant intracanal stenosis, or previous history of lumbar spine surgery were excluded.
For the given criteria, the surgical technique was selected according to the preference of the surgeon on call. Of the patients, 40 patients were treated using laser-assisted paraspinal microdiscectomy (Drs. Ahn Y and Keum HJ), while 44 patients were treated using conventional paraspinal microdiscectomy (Drs. Lee U and Lee YJ). The ease or feasibility of surgical technique did not play a role in the selection of surgery type.
Outcome measurements and statistical analysis
Patients' outcome data were obtained during outpatient clinic follow-up visits using a patient-based outcome questionnaire or through telephone interviews. Clinical outcomes were evaluated using the visual analog scale (VAS) for pain intensity and the Oswestry disability index (ODI) for functional status. 28 Global outcomes were classified into excellent, good, fair, or poor based on the modified Macnab criteria. 29 A comparison between the two groups was performed using the independent two-sample t-test for continuous variables. Fisher's exact test was performed for categorical variables. A p value of <0.05 was considered significant.
Operative technique
The operative procedures were performed in two steps. First, a standard paraspinal transmuscular approach was performed; second, the CO2 laser-assisted selective microdiscectomy technique 26 or conventional microdiscectomy technique was conducted.
A 3 cm vertical paramedian skin incision was made 2.5–3.5 cm lateral from the midline according to the location of the triangular zone bordered by the L5 transverse process, the lateral margin of the L5-S1 facet joint, and the sacral ala, as seen on the axial CT and MRI images.
After a blunt dissection was performed on the bony landmarks, a self-retractor was applied to expose the far lateral zone. The margin of the triangular bony surfaces was exposed using a dissector and electrocautery and then carefully drilled out using a high-speed diamond-tipped burr under microscopic visualization. The lumbosacral ligament in the triangular space was then removed using Kerrison punches to expose the L5 nerve root, DRG, and far lateral disc space.
To prevent intraoperative bleeding, radicular arteries and veins are carefully dissected and cut after coagulation using bipolar cautery during the dissection of the L5 DRG and herniated disc. The exposed L5 nerve root was then carefully dissected from the herniated disc using fine dissectors. After the L5 DRG has been dissected and retracted, the far lateral LDH can be selectively removed.
The extruded disc fragment and surrounding bony stenosis were removed using pituitary forceps and various mechanical tools with gentle nerve root retraction in the conventional group. However, the pathologic disc fragments and osteophytes were gradually removed using a CO2 laser (Sharplan 30C, Lumenis, Yokneam, Israel) attached to a microscope in the laser group. After removing any sequestered disc fragments using pituitary forceps, a pinpoint-sized laser beam was applied to evaporate the disc material delicately with minimal nerve root retraction. Moreover, the laser could be used to lyse any adhesions or to sculpture osteophytes compressing the nerve root. The photocoagulation effect of the laser may reduce bleeding from the soft tissue and bone during the decompression procedure.
After adequate selective discectomy, further full-scale foraminal decompression was performed using curved foraminal punches and curettes in both groups. At the end of the operative procedure, the release and free mobilization of the nerve root could be confirmed. Finally, sophisticated hemostasis was achieved and the conventional wound closure technique was performed with adequate drain.
Results
Demographics and operative data
In the laser group, 14 were men and 26 women; mean age, 56.5 years (range, 39–73). In the conventional group, 16 were men and 28 women; mean age, 54.5 years (range, 22–79). There was no significant difference between the groups in gender, age, weight, height, and BMI.
The mean operative time of the laser group was 95.88 min (range, 50–175) and that of the conventional group was 93.86 min (range, 55–150). The mean blood loss of the laser group was 107.13 mL (range, 40–250) and that of the conventional group was 112.73 mL (range, 50–220). There was no significant difference between the groups in operative data. The demographics and operative data are presented in Table 1.
NS, not significant.
Clinical outcomes
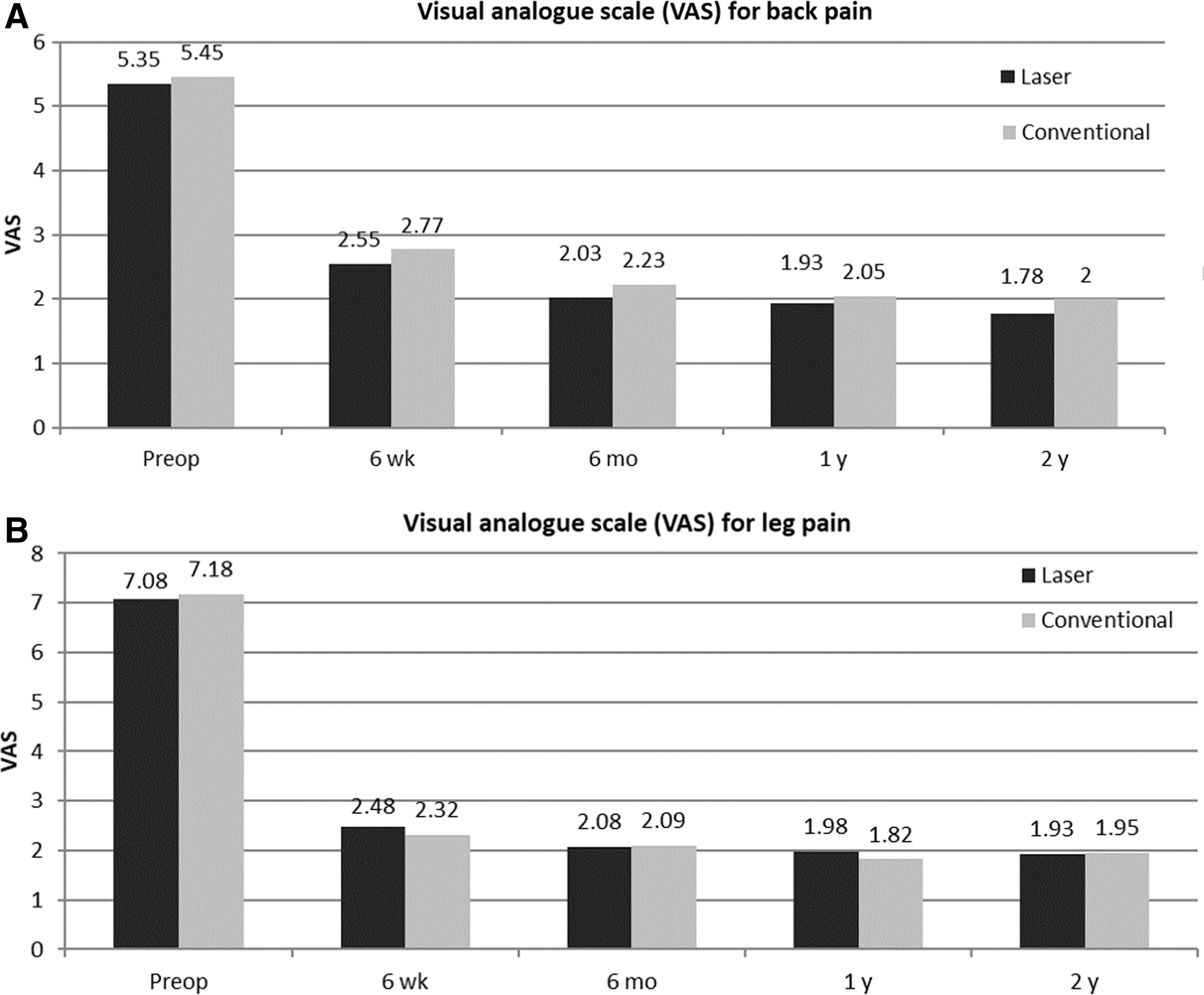
The mean VAS score for back pain improved from 5.35 ± 1.53 to 1.78 ± 0.83 in the laser group and from 5.45 ± 0.96 to 2.00 ± 0.76 in the conventional group (Fig. 1A). The mean VAS score for radicular leg pain improved from 7.08 ± 1.21 to 1.93 ± 1.38 in the laser group and from 7.18 ± 1.01 to 1.95 ± 1.17 in the conventional group (Fig. 1B). The mean ODI improved from 59.44% ± 15.95% to 15.43% ± 9.99% in the laser group and from 61.18% ± 19.33% to 17.83% ± 13.35% in the conventional group (Fig. 2). Based on the modified Macnab criteria, global outcome was found to be excellent or good in 32 patients (80%) in the laser group and in 34 patients (77.3%) in the conventional group (Fig. 3). There was no significant difference in clinical outcome between the groups.
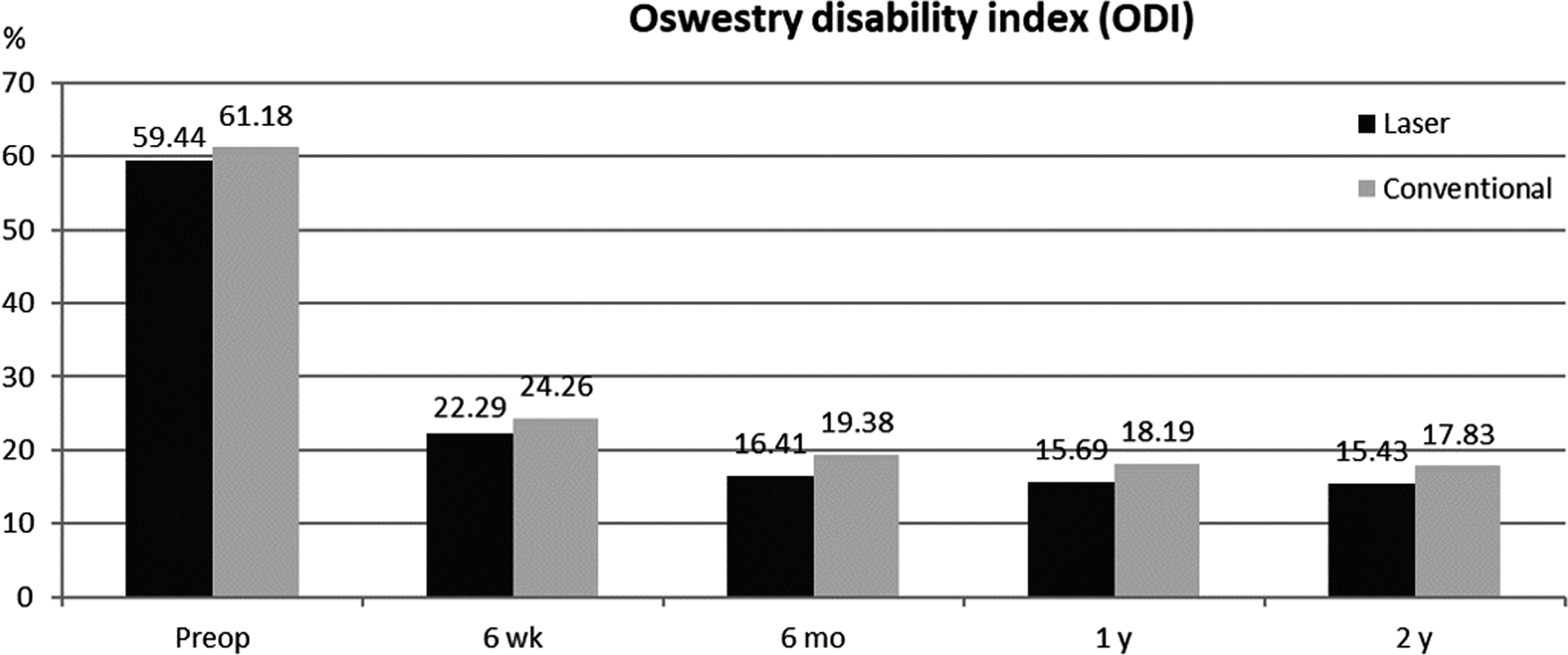
ODI preoperatively and at 6-week, 6-month, 1-year, and 2-year postoperatively. There were no significant differences between the groups. ODI, Oswestry disability index.
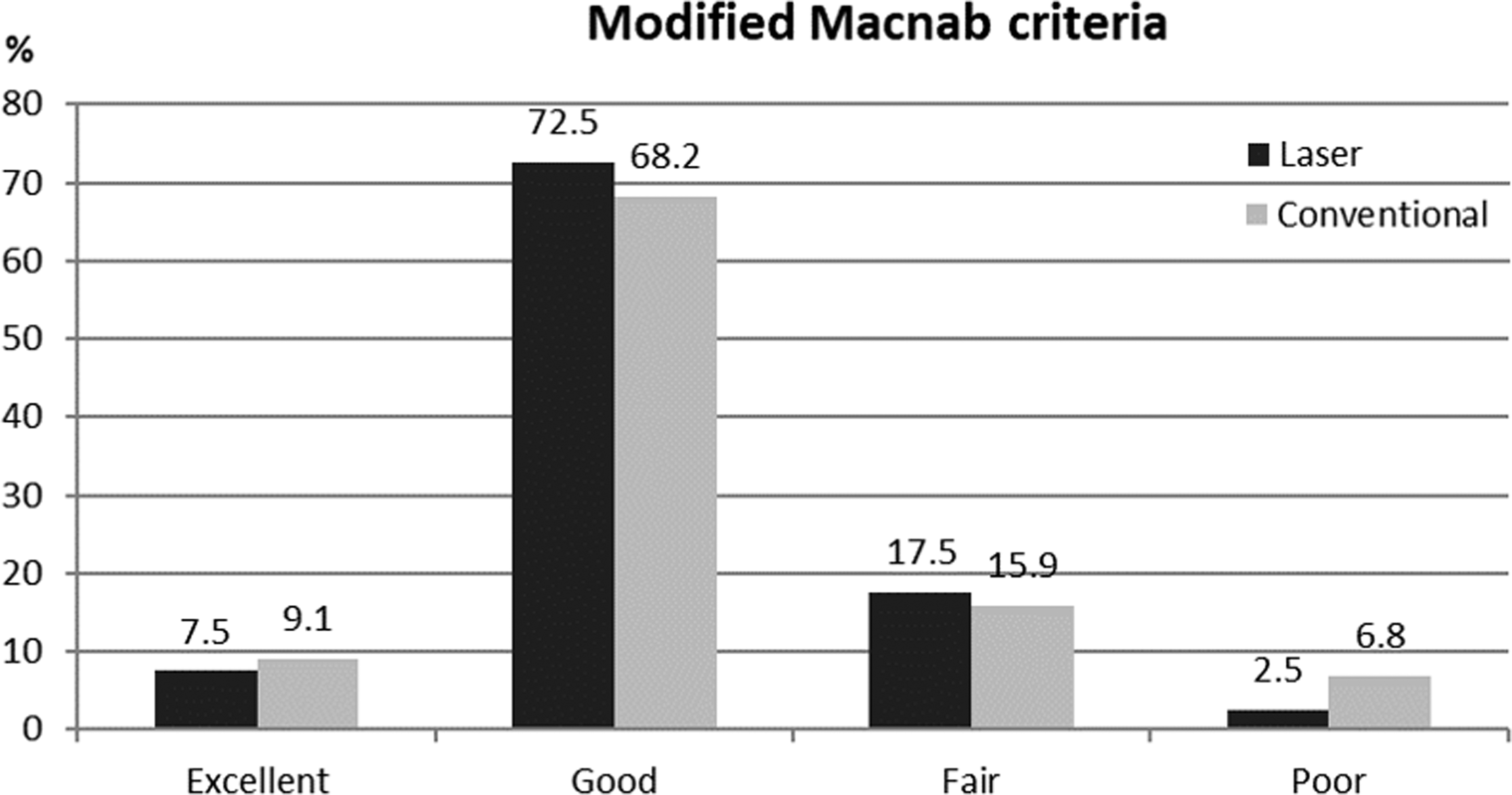
Global outcome according to the modified Macnab criteria. Excellent or good outcome was found in 32 of the 40 patients (80%) of the laser group and in 34 of the 44 patients (77.3%) of the conventional group. There were no significant differences between the groups.
The duration of hospital stay was significantly shorter in the laser group. The mean duration of hospital stay was 9.28 ± 5.26 and 12.32 ± 6.47 days in the laser and conventional group, respectively (p < 0.05, Fig. 4). The laser group also had a significantly shorter time to return to work (10.98 ± 4.60 weeks) than the conventional group (13.68 ± 5.72 weeks; p < 0.05, Fig. 5). Return to work was defined as resuming work tasks/work hours after a period of sick leave. 30,31 There was no significant difference in terms of the type of work between the groups.
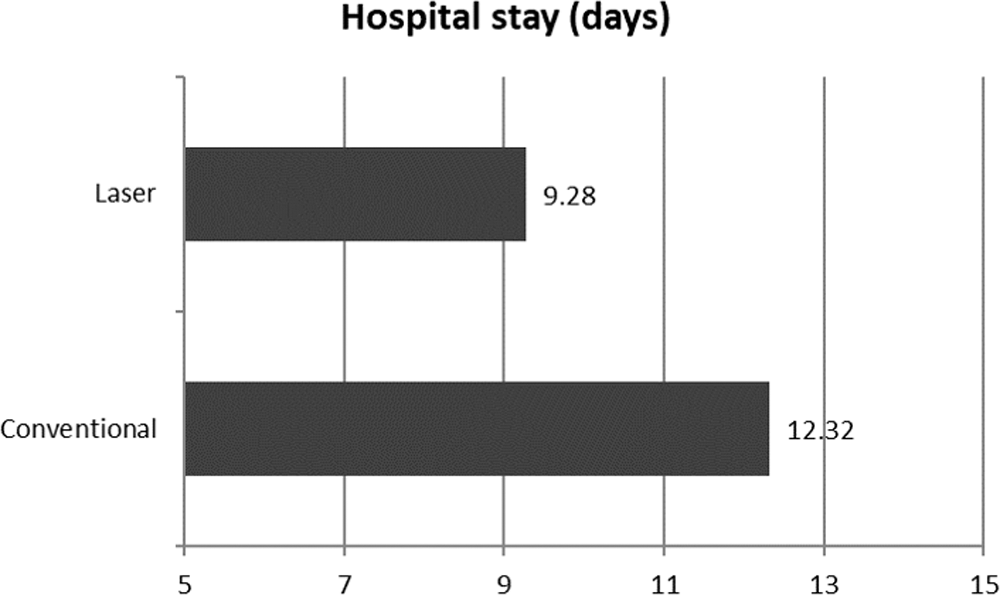
The duration of hospital stay was significantly shorter in the laser group (9.28 ± 5.26 vs. 12.32 ± 6.47 days; p ≤ 0.05).
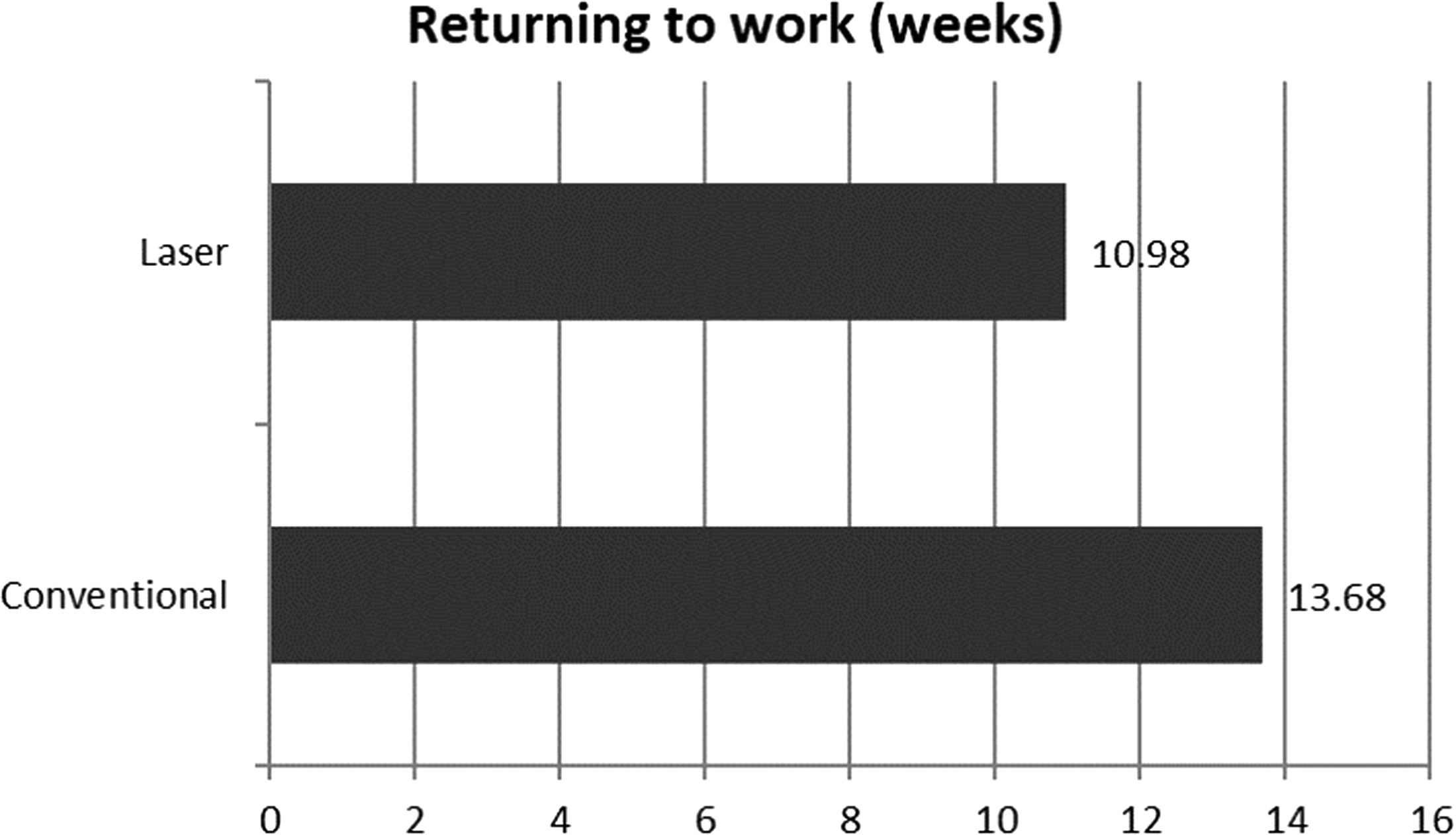
The time to return to work was significantly shorter in the laser group (10.98 ± 4.60 vs. 13.68 ± 5.72 weeks; p ≤ 0.05).
With regard to other complications, one dural tear that required intraoperative primary repair and two cases of transient dysesthesia that recovered within 6 months were reported in the laser group. Two cases of dual tear treated with intraoperative primary repair and three cases of transient dysesthesia were reported in the conventional group. Recurrent disc herniation occurred in two patients in each group. Of the four recurrence cases, one patient in the laser group had subsequent fusion surgery, and the remaining three patients improved with conservative treatments. One patient in the conventional group underwent wound repair of a wound with noninfectious fluid collection. There was no case of postoperative infection or segmental instability.
Discussion
Clinical outcomes
There were no significant differences in multiple clinical parameters between the groups. The operative data including the operative time, estimated blood loss, and intraoperative complications also showed no statistical difference.
However, the postoperative clinical course showed definitive differences. Duration of hospital stay and time to return to work were significantly shorter in the laser group. These findings can be attributed to the following reasons. First, the use of a laser scalpel in the microdiscectomy may reduce unnecessary retraction of the nerve root or DRG. Second, it may prevent excessive facet resection to obtain a wide surgical field for large forceps. Finally, it usually reduces epidural fibrosis and tethering of nerve root after decompression. For these reasons, laser microdiscectomy may result in less postoperative pain or flare and consequently, faster recovery to ordinary life.
Potential problems of paraspinal microdiscectomy for far lateral LDH
The gold standard surgical decompression technique for far lateral LDH or stenosis is facet-preserving microdiscectomy using a paraspinal approach. 9,10,17 The success rate of this paraspinal foraminotomy and microdiscectomy has been reported as ranging from 72% to 83%. 11,16,17 However, it has also been reported in considerable postoperative pain or failure cases. 11 –17 Some authors suggested that far lateral LDH showed poorer prognosis than intracanal (central or paramedian) LDH.
First, the DRG which is located in the foraminal or far lateral zone is vulnerable to mechanical or thermal irritation. Surgical manipulation of the DRG may cause postoperative flare or dysesthesia. 13,14 Moreover, the limited exposure of surgical field using the paraspinal approach may lead to incomplete decompression.
Second, far lateral LDH is frequently associated with additional pathologies within the intracanal zone at the same disc level (double herniation). 17,32 This phenomenon may cause confusion in distinguishing the exact pathologic point and requires a wider extent of decompression.
Third, a precise diagnosis of far lateral LDH is difficult. It can be easily overlooked on radiographic studies and lead to treatment failure or poor outcome. 16,33
Finally, the average age of far lateral LDH is generally higher than that of intracanal LDH and the global surgical outcome may be influenced by age. 5
The surgical field of far lateral LDH is usually narrow because it is frequently associated with foraminal stenosis, especially at the L5-S1 level. Further, the medial part of the facet joint should be preserved to maintain spinal stability after discectomy and decompression. Therefore, it is relatively difficult to remove the herniated disc fragment completely using mechanical tools alone.
Advantages and disadvantages of laser-assisted paraspinal microdiscectomy
A laser beam can be used to remove herniated disc material or bony spurs and reduce intradiscal pressure via vaporization. 21 –23 The CO2 laser-assisted lumbar microdiscectomy technique have been reported in various situations. 24 –27 Application of a laser surgical tool in microscopic decompression for far lateral LDH provides several significant benefits (Fig. 6).
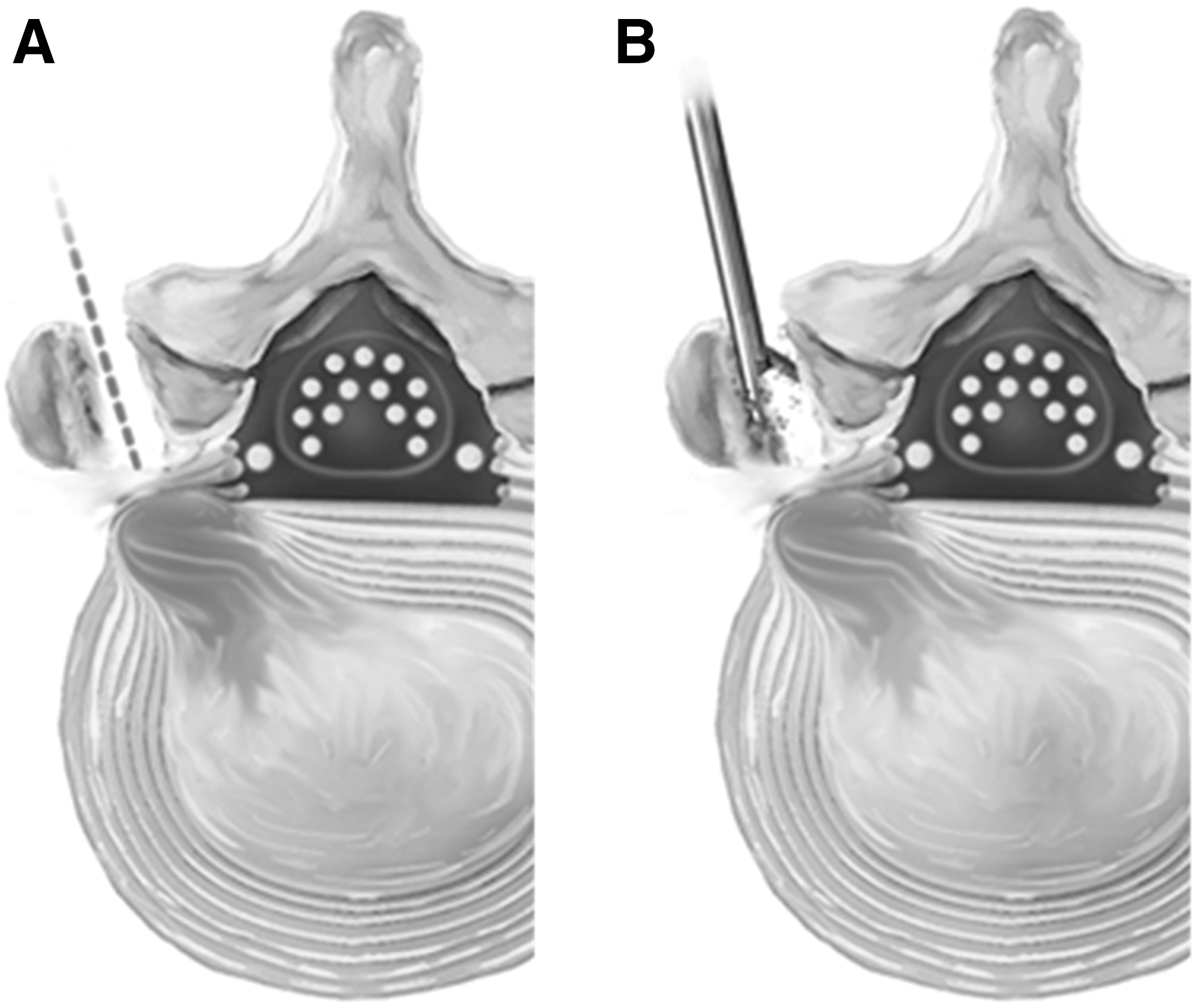
Schematic comparison of the laser microdiscectomy and the conventional microdiscectomy for L5-S1 far lateral lumbar disc herniation.
First, the pinpoint laser scalpel enables sophisticated and powerful disc ablation with minimal neural retraction in a narrow surgical field. The diameter of the focused laser beam is less than 0.5 mm, while the width of mechanical tools such as pituitary forceps is at least 5 mm. The long wavelength of the CO2 laser (10.6 μm) has high absorption in tissues and water, with rapid conversion of light energy into heat in a small volume of tissue. 34 These characteristics make the CO2 laser a powerful and precise cutting tool, and it causes minimal thermal conduction to adjacent tissues.
Second, a laser scalpel can also effectively evaporate bony stenosis or osteophytes. The vertical direction of the laser beam can tangentially resect any excessive bone growth compressing the neural tissues with no risk of instrument plunging.
Third, sophisticated tissue dissection is possible without damage to neural elements. Inflammatory fibrous adhesion or even scarring from a previous operation can be delicately dissected using CO2 laser. The use of laser may reduce the risk of dural breach, intraoperative bleeding, swelling, and trauma to normal tissues. 26,27
Finally, the laser intensity can be controlled according to the purpose of the procedure. It can be widely adjusted, using a low intensity for delicate tissue modulation or coagulation and a higher laser intensity for hard bone destruction.
The most important disadvantage of laser surgery is the risk of thermal injury to neural tissues. Any mechanical injury such as avulsion or tear of neural tissues can be recovered to some degree because some collateral innervation or the regeneration process may improve the neurological status with time. In contrast, excessive laser application to the dural sac or nerve root may cause some profound or even irreversible neurologic sequelae.
Thermal injury to other normal tissues by uncontrolled laser irradiation may cause unexpected tissue necrosis and degeneration in the skin, muscle, ligaments, bone, and disc. Therefore, laser irradiation should be strictly controlled by an expert surgeon during the entire procedure. Another problem of laser spine surgery is that the cost is quite expensive compared to conventional spine surgery, which is typically covered by a health insurance; hence, patients often bear most of the cost.
Limitations of the study
To our knowledge, this is the first study to compare the clinical results of paraspinal lumbar microdiscectomy between a CO2 laser-assisted group and a conventional group. There were some limitations to our study. Patient selection was not randomized; therefore, the risk of bias may be considerable. Second, there were no data on an evaluation of the relationship between the amount or intensity of laser energy and perioperative outcomes. Finally, this study lacked the analysis of radiographic parameters including postoperative disc space changes, extent of facet resection, and segmental range of motion. Therefore, our next issue will be a randomized controlled trial evaluating the effectiveness of laser-assisted lumbar discectomy on clinical, physical, and radiographic parameters.
Conclusions
CO2 laser-assisted microdiscectomy is a safe and effective surgical option for far lateral LDH with benefits of a minimally invasive spine surgery.
Footnotes
Acknowledgments
The authors would like to thank Jae Min Son and Jin Ah Kim for their valuable technical assistance.
Author Disclosure Statement
No competing financial interests exist.