
Abstract

N
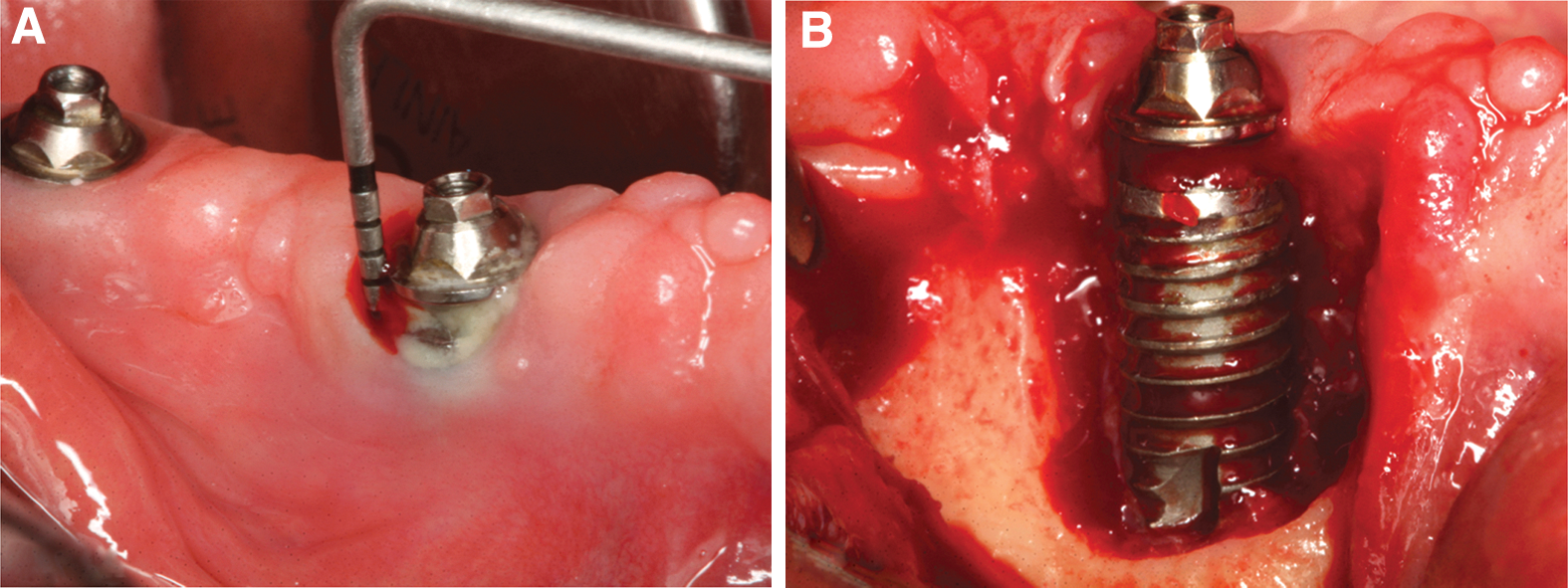
Peri-implantitis (Fig. 1) is an inflammatory process from a microbial origin that causes bone loss and if not treated could lead to the loss of the implant-supported restoration. 1 The etiology of peri-implantitis is associated with a complex bacterial biofilm 2 and risk factors such as smoking and diabetes. Other potential risk factors such as occlusal overloading, osteoporosis, and local factors related to the surgical peri-implant site might increase the severity of the peri-implant tissues destruction.
Intriguingly, there is no specific and predictable treatment for peri-implantitis, although several surgical and nonsurgical therapeutic strategies have been proposed to manage this complex multifactorial disease. 1 These strategies to treat peri-implantitis can be divided into anti-infective and regenerative therapeutic approaches. Control of the bacterial plaque in subgingival environment and the removal of the contaminants and hard deposits on implant surfaces are sine qua non to restore the peri-implant tissue health. Further, mechanical and chemical methods change the implant surface topography, as well as the oxide layer, avoiding peri-implant bone regeneration and consequently the new bone reformation on the previously contaminated area (also called reosseointegration).
Physical methods using lasers have been employed in both anti-infective and detoxification methods in the past decades. 3,4 Anti-infective therapy using photodynamic therapy (PDT) utilizes a low-power laser after photosensitizing molecules application such as toluidine blue and methylene blue. The mechanism by which PDT kills periodontal pathogenic microorganisms such as Agregatibacter actinomycetemcomitans, Porphyromonas gingivalis, Fusobacterium nucleatum, and Prevotella intermedia is currently under active investigation. Previous data showed that this mechanism may involve alterations, such as oxidation of biomolecules in membranes and/or plasma membranes of oral pathogens, and DNA damage which can be mediated by the singlet oxygen. PDT offers some advantages over the use of conventional antimicrobials (antiseptics and antibiotics), as prevention of several target periodontopathogens resistant to the photochemically generated reactive oxygen species (ROS), which is thought to be responsible for bacterial killing; moreover, it would not be necessary to keep high concentrations of the photosensitizers in peri-implant defects for long periods. Hence, PDT may be a useful alternative to antibiotics for the local infection treatment by eradication of target cells since the PDT protocol uses an appropriate photosensitizer, well-known laser parameters, and light wavelength for generation of ROS.
Sterilization and cleaning/decontamination of dental implant surfaces by means of high- and low-intensity laser therapy using CO2, Nd:YAG, Er:YAG, Er,Cr:YSGG, and GaAlA have also been employed. Laser irradiation removes the inflammatory soft tissue around the peri-implant pocket and removes contaminates from the implant surface without damaging or altering the titanium surface topography. Taken together, this approach allows a better stabilization of the blood clot with or without adding some bone graft materials during the guided bone regeneration. An elegant review 5 has also pointed out that additional decontamination and detoxification effects may impact positively on wound healing of the treated peri-implant site and offer several advantages over conventional mechanical treatment using curettes, prophy jet power, and burs. Complementarily, it could be speculated that laser irradiation of the dental implant surface could provide an antimicrobial effect and inhibit bacterial attachment/colonization after irradiation.
Finally, photobiomodulation (PBM) produced as secondary effect after high-level laser therapy positively modulates wound healing. 6 This effect is induced by promotion of cell proliferation and differentiation, as well as anti-inflammatory effects playing a pivotal impact on peri-implant tissues. Recent study 7 on PBM showed that low doses of infrared laser-induced ROS generated pathways that increase the levels of transforming growth factor (TGF) beta-1 next to wound healing lesions. This increase on TGF beta-1 after PBM plays an important role on human beta defensin-2 expression, the antimicrobial peptides that present a positive effect against microbes. In addition, PBM treatment affects directly cell receptors as opsins, which could modulate cell tumors.
Previous data have suggested that lasers did not show additional benefits over others treatment. However, these studies did not take into account the severity and extension of the peri-implant lesion, allowing a similar effect between lasers and other cleaning methods of the contaminated implant surface topography. The clinical end-point used in most of the published studies about peri-implantitis treatment is based on reduction of probing depth and absence of bleeding on probing and/or suppuration and not peri-implant bone regeneration or bone filling defect. Osseointegration was based on the bone tissue anchorage around dental implants under occlusal function. This is not fair enough to be compared to the achievement of healthy peri-implant tissues without new bone-to-implant contact around ailing implants (also called re-osseointegration) that restores enough bone tissue anchorage to maintain the implant supported restoration for long-term periods. Consistent data have shown that periodontally treated teeth with reduced periodontium after surgical and nonsurgical treatment of periodontitis were able to maintain their healthy status on well-maintained subjects, nevertheless this analogue situation might not be expected for the implants after peri-implant disease bone loss.
This provocative insight should lead the clinicians and periodontists thinking over the paradigm that laser equipments are expensive and did not add additional clinical outcomes to peri-implant treatment. As previously described, peri-implant lesions are a complex multifactorial disease that needs a simple and predicable strategy to reach the favorable clinical outcomes without damaging the implant surface, improving the wound healing. To this end, is the laser the best choice for the treatment of peri-implantitis? Surely, yes, it is.