
Abstract
Objective:
The purpose of this literature review was to evaluate the effectiveness of using Er:YAG (erbium-doped yttrium/aluminum/garnet) laser or Er,Cr:YSGG (erbium, chromium-doped yttrium/scandium/gallium/garnet) laser on calculus removal and their effect on the topography and roughness of root surface in comparison with the conventional instruments in the nonsurgical periodontal therapy.
Background data:
One of the most challenging problems in treatment of periodontal disease is the elimination of plaque and calculus, leaving a clean and smooth root surface to decrease plaque and calculus retention, and for good gingival reattachment.
Materials and methods:
PubMed and Google Scholar were searched for available literature. The electronic search was limited to articles published in the period between January 2007 and April 2017, in the English language.
Results:
A total of 47 publications fulfilled the inclusion criteria of this systematic review and screened according to the research questions. Calculus removal using the ultrasonic instrument showed remaining calculus compared with the hand instrument, whereas, on the contrary, erbium lasers revealed no remaining calculus or smaller amounts compared with the conventional instruments when used in appropriate settings. The results of this review showed that ultrasonic instrumentation produced effects on the root surface almost similar to that of hand instrumentation. Er:YAG laser and Er,Cr:YSGG laser clarify a little more surface roughness when compared with conventional instruments.
Conclusions:
The present systematic review indicates that a combination of scaling and root planing (SRP) using the erbium lasers as an adjunctive therapy at certain parameters can be appropriate to remove residual debris from the root surface and at the same time have little or no negative thermal effect on the root surface. The Er:YAG laser also seems to be the most suitable for nonsurgical periodontal therapy. Additional new good-designed studies are needed to evaluate the effectiveness of erbium lasers with SRP in nonsurgical periodontal therapy.
Introduction
When the calculus and biofilm are on the enamel surface, scaling alone is sufficient to remove them completely from the enamel surface, leaving a smooth and clean surface, but when the calculus is on the root surface it is often embedded in the cementum irregularity. Therefore, scaling alone is unsatisfactory to remove it. 1 The superficial layer of root surface must be removed to eliminate the embedded part of the deposit, and in some cases where the cementum is thin, that may lead to unavoidable and recommended dentin exposure. 2 Sonic and ultrasonic devices were used to remove heavy calculus layers from supra and subgingival areas, with different types of tip design. Water was used to decrease heat generated from friction and to clean out the deposits from the pocket. Ultrasonic tip provides better access to the subgingival area than accessibility only with hand instrument. 3 However, both methods of instrumentation give a good result when used to remove plaque and calculus or bacterial reduction and reduce the symptoms of periodontitis. 4 It is well known that traditional treatment is useful to remove heavy deposits and stain more quickly with less trauma to the tissue, therefore resulting in less postoperative pain and discomfort. Many new technologies are being used for the periodontal procedure, including laser; laser was newly introduced, since three decades, in dentistry to be used for many therapies in hard and soft tissue. 5,6
In periodontology, laser has an indication in surgical therapy, in nonsurgical treatment of periodontal disease, and in pathological changing in all periodontal diseases. When applying a laser in periodontology, the following advantages can be incorporated into the treatment: enhance decreasing of bacteria, reduce bleeding, improve access to complex anatomical structures, as well as increased patient comfort and biostimulation of the healing process. Several types of laser are used, for example, Er:YAG (erbium-doped yttrium/aluminum/garnet) and Nd:YAG for nonsurgical periodontal therapy pockets of up to 8–10 mm. A randomized, double-blinded, clinical study compared the effect of scaling and root planing (SRP) alone versus SRP plus diode laser using clinical, microbiological, and inflammatory analyses in patients with aggressive periodontitis. The result showed significantly more improvement in probing depth levels and providing clinical attachment level (CAL) gain, after a single treatment, using SRP plus diode laser at 12 months compared with SRP alone. However, it did not significantly reduce the percentage of bleeding sites compared with SRP treatment alone. 7
For good results, the surgical periodontal procedures use the Er:YAG laser for calculus removal as the first step and then use diode or Nd:YAG lasers to support decontamination, biostimulation, and de-epithelialization. A study proved that the wound-healing time after 980 nm diode laser-assisted surgical treatment of the lateral periodontal cyst was shorter than that with conventional surgical treatment. Furthermore, the study results showed a significant reduction in postoperative complications and improvement in the periodontal parameters assessed after a 12-month follow-up. 8 Also, in people with uncontrolled diabetes, who are generally at danger for hyperglycemia, which can result in increased inflammation leading to an increased risk of periodontal disease, in a split-mouth study, the clinical benefits of photobiomodulation (808 nm GaAlAs diode laser with an energy density of 4.46 J/cm 2 on days 1, 2, and 7 after SRP), in type 2 Diabetes Mellitus (D.M.), in nonsurgical periodontal treatment were evaluated. In this study, it was pointed out that photobiomodulation acts as an adjunctive therapy to nonsurgical periodontal treatment, improving periodontal healing in type 2 D.M. 9
Disinfection of periodontal pockets can be done very effectively using the neodymium laser. 10 The advantage of the neodymium laser compared with diode lasers in periodontal treatment is the laser light penetration into the tissue of more than 10 mm. Hence, all microorganisms penetrating the marginal periodontium can be reached and killed. While the Er:YAG laser is a helpful tool used to remove plaque, calculus debride safely of the periodontal pockets. 10 The purpose of this systematic review was to compare the effect of using Er:YAG laser or erbium, chromium-doped yttrium/scandium/gallium/garnet (Er,Cr:YSGG) laser and conventional instruments on calculus removal and their effect on the root surfaces after treatment.
Research questions
Is there a difference in the amount of plaque and calculus removed using Er:YAG laser or Er,Cr:YSGG laser in comparison with the conventional instruments?
Is there a difference between Er:YAG laser or Er,Cr:YSGG laser in comparison with conventional instruments regarding the effect on root surfaces after treatment?
Materials and Methods
Study selection strategy
PubMed and Google Scholar were searched for available literature. The electronic search was limited to articles published in the period between January 2007 and April 2017, in the English language.
The review should only consider studies that meet all inclusion criteria and do not violate any of the exclusion criteria to answer the research questions mentioned above.
Inclusion criteria
The inclusion criteria were as follows: (1) included were in vitro and human studies, (2) erbium lasers, hand, and ultrasonic periodontal instruments, (3) to answer the research questions, the search was just restricted to patients with periodontitis, (4) the systematic literature review was conducted in Google Scholar and PubMed, (5) the search was restricted to English articles and limited the time from 2007 to 2017, (6) 4 mm or more pocket probing depth and1 mm or more clinical attachment loss or alveolar bone loss, and (7) the following criteria: (i) efficiency of plaque and calculus removal of different periodontal instruments and (ii) the effect of use of different periodontal instruments on the topography and roughness of root surface.
Exclusion criteria
The exclusion criteria were as follows: (1) the exclusion included animal studies and literature reviews, (2) research articles in which patients with systemic diseases or conditions that affect healing, those smoking, and patients taking antibiotic therapy when there is a medical condition, (3) articles that did not have sufficient information on laser settings, (4) further excluded were such studies, despite calculus detection, (5) study outcomes with a specific focus on specific diseases such as studies on the treatment of periodontitis, abscesses, peri-implantitis, periodontitis associated with endodontic lesions, or developmental or acquired deformities were also ruled out, (6) studies considering surgical interventions (frenectomy, vestibuloplasty, excisional procedures, crown lengthening, incisions, and drainages; implant exposures during second-stage surgery) vestibuloplasty, (7) studies examining measures and interventions on damage occurring to the adjacent tissues such as bone by using the erbium lasers, (8) to answer the research questions, all types of publications were included, only the following criteria were excluded from the review: (i) pain and thermal side effects during and after periodontal therapy with erbium lasers and (ii) healing time required after treatment of periodontal disease.
Results
Original research articles resulted in a total of 2619 records. The literature search was carried out for articles between January 2007 and April 2017, using the following search keywords “nonsurgical periodontal therapy,” “root surface debridement,” “periodontitis therapy,” “ultrasonic periodontal instrumentation,” “Er,Cr:YSGG laser,” and “Er:YAG laser.” With an additional electronic database search in ResearchGate, electronic search was conducted by one reviewer (M.A.A.).
A total of 2619 records were found (Fig. 1). After reading, analyzing, and removing duplicates and assessing the titles of the publications, 193 titles could be included because they remained relevant to the research questions. By initial reviewing of the received abstracts of the remaining studies, 146 further publications were excluded. This exclusion was founded on 57 studies that presented data on clinical evaluation of periodontal disease probing pocket depth, CAL, and bleeding on probing. Thirty-one literature reviews were excluded as well as 44 animal studies; they did not meet the inclusion criteria. Fourteen were excluded from this review because they did not assemble the search criteria and the given information on antibacterial activity of the erbium lasers or conventional instruments. Forty-seven suitable full-text articles were read and evaluated independently by one author (M.A.A.) and confirmed by other authors (R.N. and N.G.).
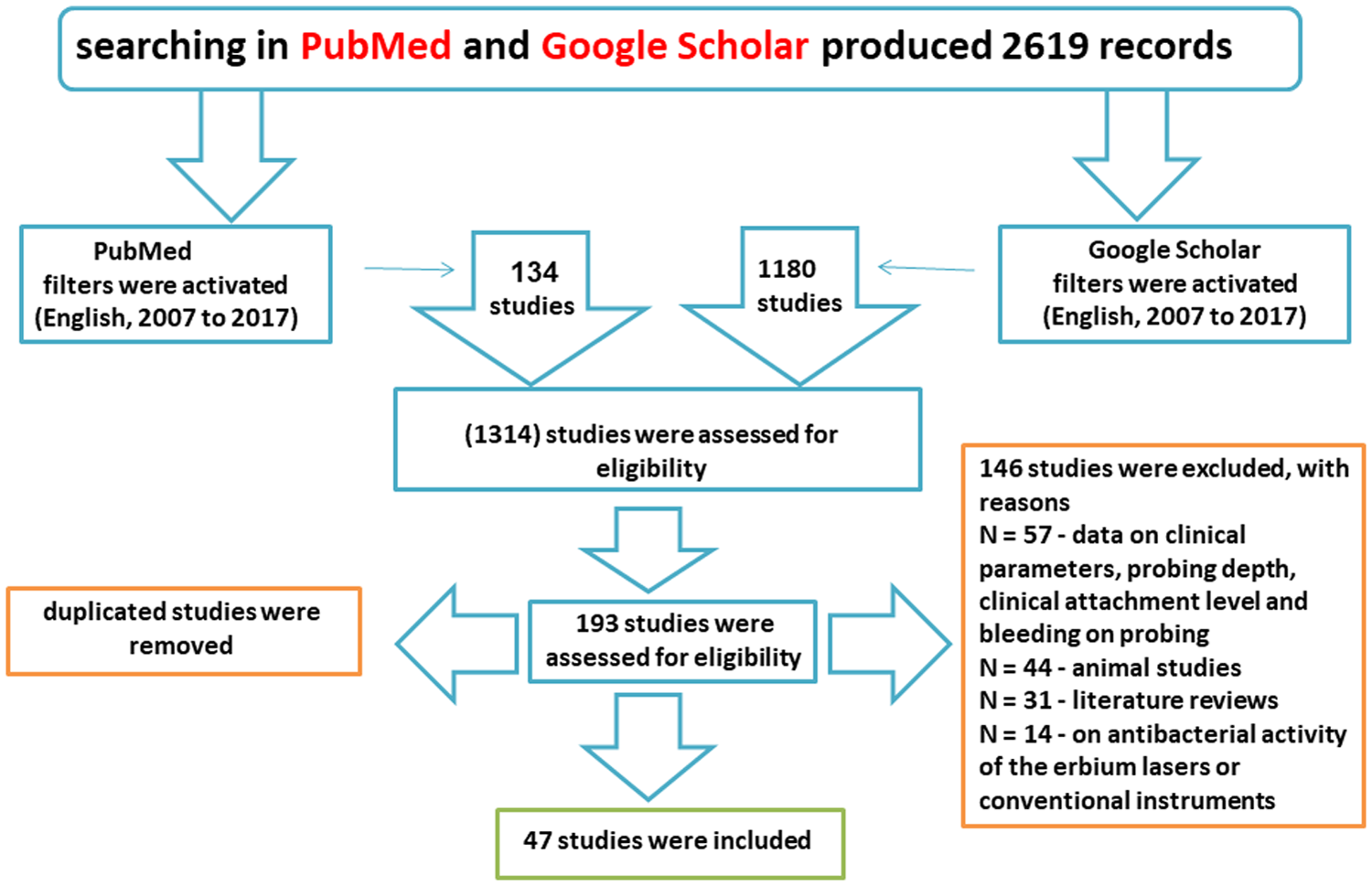
Description of selection process of the included publications.
Assessment and evaluation criteria for the efficiency of calculus removal and the effect on the topography and roughness of root surface of different periodontal instruments were based on reviewing the collected results and conclusions from each reviewed study. Further, presenting all available evidence and scoring according to explained criteria. Individual estimation of the reviewer (M.A.A.) in this method is patently susceptible to inaccuracy. However, after taking great care to find all relevant studies, basically assess each study, combining the findings from individual studies in an unbiased manner (Tables 1 and 2). Two reviewers (R.N. and N.G.) evaluated all the included articles and assessed the proposal to make sure to minimize the risk of bias. Moreover, the previously defined inclusion and exclusion criteria were used to select the definitive studies to be included, and the Preferred Reporting Items for Systematic Reviews guideline was followed.
Efficiency of Plaque and Calculus Removal of Different Periodontal Instruments
DIs, diamond-coated ultrasonic inserts; HIs, hand instruments; Er,Cr:YSGG, erbium, chromium-doped yttrium/scandium/gallium/garnet; PIs, plain ultrasonic inserts; PU, piezoelectric ultrasonic; SEM, scanning electron microscope; US.
Effect of Using Different Periodontal Instruments on the Topography and Roughness of the Root Surface
Er:YAG, erbium-doped yttrium/aluminum/garnet; HC, hand curettes; HD, hand instrument debridement; SRP, scaling and root planning; VA, vector system with abrasive fluid; VOU, vertically oscillating ultrasonic; VP, vector system with polishing fluid.
Study evaluation
Articles were evaluated based on the same idea as in the study by M.A.A., R.N., and N.G. Antibacterial effect of using the Er:YAG laser or Er,Cr:YSGG laser compared with conventional instrumentation method—a literature review. Lasers in Dental Science 2017. 11
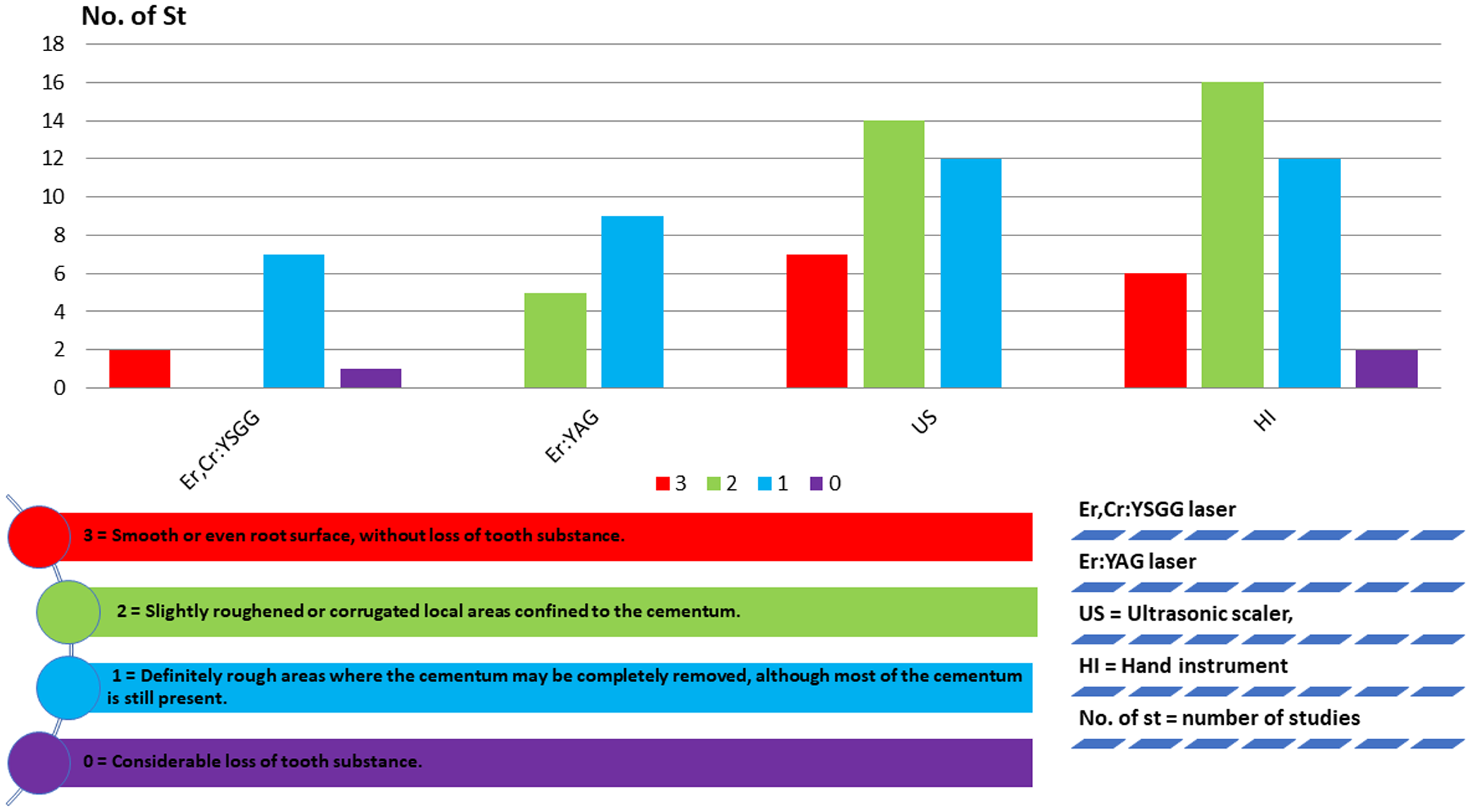
The data were recorded using the following indices: Remaining calculus and roughness or loss of tooth substance index (Figs. 2 and 3).
12,13
Efficiency of plaque and calculus removal. Effect of different periodontal instruments on the root surface. 3 = No calculus remaining on the root surface and smooth, or even root surface without loss of tooth substance. 2 = Small amount of material probably consisting of calculus and slightly roughened or corrugated local areas confined to the cementum. 1 = Definite amount of calculus confined to smaller areas and definitely rough areas where the cementum may be completely removed, although most of the cementum is still present. 0 = Considerable amount of remaining calculus appearing on the treated surface and high roughness with considerable loss of tooth substance.

Discussion
Efficiency of plaque and calculus removal of different periodontal instruments
The basic treatment of periodontal disease is the removal of the underlying problem of causing the disease. The elimination of plaque and calculus is considered an essential aim in the treatment of periodontal disease, and the success of healing of this disease depends on the amount of plaque and biofilm efficiently eliminated from the root surface.
First, in nonsurgical periodontal therapy, hand instrument scaling was most used until studies showed an increasing amount of evidence that ultrasonic instruments were effective in removing calculus, with significantly less time required to remove the calculus from root surfaces and leave the treated root surfaces smoother for better healing and reattachment. In the recent past was reported that Er:YAG laser and Er,Cr:YSGG laser could offer sufficient removal of subgingival calculus without thermal side effects in the level that appears to be the same to that yielded by ultrasonic scaler and hand instrument. 14,15 In agreement with the current findings, the Er:YAG laser demonstrated a relevant difference in efficiency of calculus removal compared with the Er,Cr:YSGG laser. 16
Efficiency of plaque and calculus removal using Er,Cr:YSGG laser
Laser treatment for periodontal disease reduces patient trauma, postoperative complications, and healing time. It was concluded that the use of Er,Cr:YSGG laser for root scaling with a 1.0-W power output setting may be done without any morphological change of root surface and with the acceptable efficient removal of calculus. 17 Data from an in vitro study have also shown that both hand instrumentation and erbium laser treatments were effective in calculus removal from root surfaces without any observed thermal changes in the form of melting or carbonization, when the effectiveness of erbium, Cr:YSGG laser and conventional treatment on calculus removal was examined. The results of this study recommended that the laser procedures, when used in appropriate parameters, are able to achieve SRP in the treatment of periodontitis. 18
Efficiency of plaque and calculus removal using Er:YAG laser
The objective of using laser in nonsurgical periodontal therapy is to be at least as effective as the conventional treatment to clean the root surface especially in the periodontal pocket area. Studies evaluated the removal of subgingival calculus. In the first study with fluorescence feedback-controlled Er:YAG laser, they found that the amount of remaining calculus following laser irradiation depends on the fluorescence threshold level for a feedback-controlled Er:YAG laser. By lowering the laser fluorescence threshold, the amount of remaining calculus decreased. The second study demonstrated that the erbium laser compared with the Er,Cr:YSGG laser appears to have an advantage in terms of time and efficiency of periodontal disease treatment. 19,20
Efficiency of plaque and calculus removal using conventional instruments
The effectiveness of two ultrasonic devices (two piezoelectric ultrasonic Scalers) was compared with the hand instrument and it was found the remaining calculus index did not differ significantly among the three instrument groups. 21 Ultrasonic scaling is as effective as hand instrumentation in plaque removal. 22 In an attempt to increase the speed and efficiency of deposit removal, an in vitro study was done to see the difference in speed and efficiency between hand instrument and magnetostrictive ultrasonic instrument with plain inserts (PIs) and diamond-coated inserts (DIs) and found that the surfaces treated with hand instrument show less residual calculus, but on the contrary, the DIs were faster in calculus removal followed by sharp Gracey curettes [hand instruments (HIs)] and PIs. 23 In the same context, data from an in vitro study have shown that all the three instruments were effective in removing calculus and achieving a clean root surface; Gracey curette left a cleaner surface compared with the standard smooth ultrasonic tip. DIs were equal to the Gracey curette in the removal of calculus from the root surface. Root surface irregularity and damage of tooth hard substance with diamond-coated ultrasonic tip were significantly greater in contrast to the other two instruments. 24 Further, it was observed in a study that none of the root surfaces treated with any of the modalities of hand and ultrasonic instruments was completely free of calculus, but hand scaling with Gracey curettes gives better outcomes in terms of remaining calculus on the root surface. 25 Relatively more plaque was residual in the ultrasonic scaler (VEC) and little remaining plaque was found after use of the sonic device (AIR) and the ultrasonic scaler (TIG). 26 A study pointed out that using ultrasonic scalers for periodontal disease treatment is more efficient in the treatment of periodontal pocket but unable to remove complete endotoxins from root surfaces to achieve regeneration. 27 It is commonly assumed that less experienced operators tend to work with a higher power level of the powered device or to apply higher pressure to get higher efficacy. 28 Numerous factors may influence the efficiency of calculus removal such as the extent of periodontal disease, the instruments used, and the experience and skills of the operator. 29,30 An in vitro study has been different, comparing the periodontal disease treatment by use of conventional treatment in the hands of experienced versus less experienced. The study has shown that the Gracey curette, a piezoceramic ultrasonic scaler, and a sonic scaler were effective in mechanical root debridement, and surface roughness was higher with Gracey curettes followed by a sonic scaler and then a piezoceramic ultrasonic scaler, regardless of operators' experience. 31
Comparing the efficiency of plaque and calculus removal using different periodontal instruments
The objectives of periodontal pocket debridement are not only for cleaning but also for disinfection. For this reason, the efficiency of scaling after applying erbium laser and Er,Cr:YSGG laser was investigated and despite the general acceptance of surface roughening after laser treatment, several other studies applying erbium:YAG laser at 40–160 mJ and 10 Hz showed a similar periodontal pocket treatment competence of both laser and ultrasonic debridement. 16,32 The results of a study showed that erbium laser with feedback control allows a selective elimination of calculus without any alteration of the root surface, with more capacity to remove calculus. 32 Moreover, prior studies have usually not succeeded in presenting a general conclusion, and the outcomes of laser efficiency in root surface cleaning are not similar considering the extensiveness of laser types. 33 In an in vivo and in vitro study, calculus was efficiently removed with Er:YAG laser, but compared with ultrasonic scaler, the Er:YAG laser leaves a more rough and irregular surface, free of carbonization and melting. 34 In another study, by comparing the scaling effect utilizing manual instruments, ultrasonic tools, and Er:YAG laser on the reattachment of connective tissue cells of the gums to the root surface of the severe periodontitis diseased teeth, it was shown that although several dental surface cleaning procedures may differ in other aspects, they are the same regarding fibroblast morphology. 35
Effect of using various periodontal instruments on the root surface
The roughness of the root surface can affect the calculus and plaque accumulation. Therefore, smooth root surfaces are required to minimize plaque accumulation, reducing the occurrence of periodontitis. 36,37 Regardless of the instrument used for SRP treatment, conservation of tooth structure is very important. Because of the eradication of cementum layers and sometimes dentin layers, this leads to other complications in scaling procedure. 38 It is well accepted that roughness of the root surface does not negatively influence periodontal healing after periodontal treatment. 39,40 The degree of roughness, after calculus elimination, is not very important, but after root planing, it is very important to obtain healthy surfaces with minimal craters and holes after treatment, which will facilitate bacterial colonization and plaque formation on the root surface. 41
Effect of Er:YAG laser on the topography and roughness of root surface
Effects of laser irradiation depend on the wavelength, power output, pulse duration, spot size, and irradiation time, also dependent on the optical density, structure, and maximal absorption of tissue. 42 The potentiality of the Er:YAG laser in SRP was investigated, very long pulses (750–1000 μs) of Er:YAG laser give a smoother surface in general and provide a superior efficiency compared with a pulse duration of 140–400 μs, with the same energy densities. In this study, it has been irradiated with high power, and the water irrigation was not clear. Also, to get a completely smooth surface by just decreasing the energy to less than 22.6 mJ at the finishing period of treatment. 43
Effect of conventional instruments on the topography and roughness of the root surface
The production of smooth root surface with less alterations is the essential goal of SRP, which can be obtained with ultrasonic and hand instruments. 44 To examine the performance of different conventional ultrasonic debridements (piezoelectric ultrasonic device, magnetostrictive ultrasonic device, hand instrument) on the root surface, studies were conducted, which concluded that the devices were similar. The root surfaces appeared unequal, just the loss of dentine substance was observed with piezoelectric devices less than with magnetostrictive. Also, rougher root surfaces were found after treatment with curettes and more root surface tissue was removed than with the ultrasonic device. 45,46
Generally recognized as the gold standard of therapy in the management of periodontal diseases is the mechanical debridement of calcified deposits from the root surface. Sonic and conventional ultrasonic debridements were first designed for the periodontal pocket treatment and extrinsic stains. 19 When manual and ultrasonic instrumentations were combined, the root morphology was totally different from that observed when they were single handedly resulting in some cases in the complete removal of the smear layer and the exposure of collagen fibrils. 47 That will promote the integration between the healed connective tissue and root surface, and assist in the attachment of gingival fibroblasts. 48
In one investigation, it was established that the efficiency of calculus removal of the vector system with abrasive fluid (VA) and metal curette did not differ significantly from that of the HI, and conventional ultrasonic system with an “IS” tip. Root surfaces were smoother in the VA and vector system with metal curette insert and with hydroxylapatite containing polishing fluid (VP) groups than those in HD and Satelec groups; on the contrary, the calculus removal effectiveness of the (VP) and metal curette groups was significantly less compared with the HD and Satelec groups, because some scratches were clear on the root surfaces treated by HD or the Satelec ultrasonic system. 49 Another study evaluated and compared using confocal microscopy and scanning electron microscopy (SEM), the root surface roughness after using Gracey curettes, diamond burs, a piezoceramic ultrasonic scaler, and a piezosurgery ultrasonic scaler. Also was found that a smoother root surface was left after using the piezoceramic ultrasonic scaler and piezosurgery ultrasonic scaler; the diamond burs produced a rougher surface than the ultrasonic instruments and hand curettes, and the piezosurgery ultrasonic scaler created the smoothest surface. 50
The presence of smear layer production and irregular root surface affects periodontal attachment. A third study came to the same results when evaluating the morphology and adhesion of blood components on root surfaces instrumented with piezoelectric ultrasonic and hand instrument; piezoelectric ultrasonic showed irregularities of root surface with the presence of smear layer more than with manual curette treatment. 51 One of the most important criteria to explain the success of the different periodontal treatments is the evaluation of root surface roughness. Results of an experiment are in contradiction to other studies that have confirmed that approximately similar roughness on the root surface was earned after scaling with Periotor inserts, followed by Gracey curette and ultrasonic tip. 52 In contradiction to that, a uniformly smooth surface is likely to facilitate better adhesion and healing of periodontal tissues following mechanical debridement. After estimation of the surface profiles of healthy and periodontal treated roots, it was found that after manual and ultrasonic instrumentation following root planing treatment, the Gracey curettes and ultrasonic scaler are capable of reducing roughness critically, although Gracey curettes yielded smoother surfaces than ultrasonic scalers. 53 Extensive cementum and dentin removal appear to be not necessary to achieve efficient healing. 54 Damage to the root surface is a major concern of the dentist. If the dentist removed the root surface, a new environment may be created for retention of subgingival plaque. The topography of untreated single-rooted teeth was compared in vivo with a root planing with a curette, a piezoelectric ultrasonic scaler (PU) or a vertically oscillating ultrasonic scaler (VOU). The device (VOU) achieves a lower roughness value than the other two instruments, and it is concluded that ultrasonic devices are therefore a valid alternative to manual instrumentation with a curette. 55
Another study investigated the surface roughening of root produced by hand and conventional ultrasonic instrumentation with different power settings (10%, 50%, and 100%). The result showed no difference between manual and conventional ultrasonic instrumentation at 10%, 50%, and 100% power settings; manual instrumentation produced a similar defect on the root surface to that of ultrasonic instrumentation. 56 Recently, the same author reported that ultrasonic instrumentation with a high-power parameter produced a rougher root exterior than ultrasonic instrumentation with a lower power parameter, also manual SRP with curettes creates lower roughness than ultrasonic instrumentation independent of power parameters. 57 The conclusion of this study did not support the observation of another study which observed that the lowest surface roughness was seen on the samples where SRP was accomplished with ultrasonic scaler at medium-power parameters. In the group where SRP was with ultrasonic scaler at high-power parameters, the root surface roughness was almost similar to that when SRP was carried out with a curette. 58 The technique by which the adherent material on root surfaces can be eliminated with the ultrasonic scaler instrumentation is through the mechanical chipping action, when in contact with the root surface. However, the oscillating probe may also harm the tooth surface, especially in visibly restricted regions. 59 Magnetostrictive probes oscillate with greater vibration displacement amplitude and cause significantly greater defect depths and volumes than piezoelectric probes. 59 The efficiency of SRP conventionally, with various hand instruments, was examined. A similar research was also examined and compared hand devices, as the specimen was instrumented with new Gracey curettes 5/6 from many different brands (carbon steel, stainless steel Neumar, stainless steel Millenium, premium steel Neumar, Hu-Friedy). They determined, according to the methodology applied, the group of curettes that presented a high-grade smoothness of root surface following the SRP was premium steel Neumar. 60
Comparing the effect of different periodontal instruments on the topography and roughness of the root surface
The effects of erbium laser and neodymium laser on the surfaces of root were evaluated. Also compared them with those produced by using conventional ultrasonic debridement; in all groups treated with Er:YAG laser (RR 10 Hz, E 80, 100, and 120 mJ, PD 250 μs) dentin tubules were exposed and cementum layers were removed. 61 Evaluation of root surface irregularity following scaling by Er:YAG laser (120 mJ, 12 Hz, 75–100 μs, VSP mode, Ro7 handpiece, water cooling) was by the ultrasonic device and hand instruments. It was noted that a minimal surface roughness was inspected under SEM in specimens managed by Er:YAG laser and discussed that to create less surface roughness, it depends basically on the laser settings. 62
In the majority of studies that state the influences of Er:YAG laser irradiation, the Er:YAG laser may ablate not only dental calculus but also the external part of the underlying cementum in such investigations, the resulting surface topography was similar to microscopic acid etching. 63,64 The water cooling applied with Er:YAG laser irradiation can lead to minimal cementum ablation and thermal changes with characteristic microstructure and degradation of the external layer. 65 Examination of the conditioning effects of the CO2 or Er:YAG laser on periodontally unhealthy root surfaces following SRP in terms of the morphological alterations. In a comparison between CO2 laser and erbium laser for the treatment of peritoneal pocket and effect on the root surface, it was found that the CO2 laser has some deleterious effects on root surfaces, but Er:YAG laser may constitute a useful conditioning significant tool to periodontal pocket treatment by enhancing the periodontal ligament cells without notable undesirable effects. 66 To study the microscopic effects of Er,Cr:YSGG laser, when applied on root surface tissues with different energy settings, a study was performed and pointed out that Er,Cr:YSGG laser SRP has some advantages compared with the conventional treatment procedure and this was statistically significant. The teeth also resemble the microscopic surface structure of an intact tooth. The disadvantage was increased surface roughness of the root surface due to use of high peak power density; moreover, not enough water spray during the treatment procedure. 67 Checking the effects of Er,Cr:YSGG laser irradiation on the root surfaces resulted that in SRP, all specimens had a smear layer and scratches, but in the majority, smooth (90%), only (10%) of specimens had a very rough surface without exposure of dentinal tubules. In Er,Cr:YSGG laser and in SRP-assisted Er,Cr:YSGG laser, the photomicrographs showed that all (100%) specimens were very rough, without the presence of a smear layer. 68 The root surface morphology of the teeth instrumented by curettes, piezoelectric ultrasonic scaler, and Er,Cr:YSGG laser was assessed. Samples from this curette group showed smooth root surfaces in most cases. The samples treated with piezoelectric ultrasonic scaler or curettes+piezoelectric ultrasonic scaler revealed that the root surface was rough with the presence of grooves produced by the instrument, smear layer, and blocked dentin tubules were also present. In groups managed with Er,Cr:YSGG laser or curettes+Er,Cr:YSGG laser, it was determined that all samples of the root surface were rough, with no smear layer, with open dentin tubules, and the absence of thermal damage. 69
A recent in vitro study reported that all modalities, that is, curettes, ultrasonic scalers, and the Er,Cr:YSGG laser, increase root surface irregularity. In addition, the laser has generated rougher surfaces and most changes in the root surface profile; on the other hand, the smoothest surface was observed after hand instrumentation. 70 A secondary consequence is the elimination of cementum and exposure of dentinal tubule after periodontal disease treatment. Even though the mass of cementum on the root surface is very variable and depends on factors such as patient age and previous periodontal treatments, this enabled us to analyze and compare more precisely the influence of both Er:YAG laser and ultrasonic scaling on the root surface. Ultrastructural alterations, which appeared after treatment of the root surfaces with ultrasonic and hand devices followed by Er:YAG laser irradiation, determined that the root surface changes were more clear in laser-treated groups compared with hand instruments and ultrasonic scaler and the hand instrumented samples were smoother than other groups. 71
Morphological examination and roughness analysis were accomplished and showed also in conclusion that root planing with a manual curette is the most efficient method to reduce surface roughness, but they also showed that Er:YAG laser as an adjunctive therapy to conventional SRP can reduce root surface roughness. 72 The received results of another study showed the same, that application of Er:YAG laser for SRP was not different from the hand instrument in terms of surface roughness, but led to greater surface roughness compared with the ultrasonic system. 73 Root surface roughness and loss of tooth substance were created after instrumentation with (1) hand instrument, (2) ultrasonic scaler, and (3) hand instrument+diode laser application. It was revealed that despite all the three instruments being used for routine debridement of root surfaces, ultrasonic scalers were found to be more efficient than hand scalers. Whereas the roughness caused after laser application was more when compared with the other groups, significant roughness was made on irradiation. 74 SEM provides valuable data regarding root surface morphology after SRP treatment. In the previous years, laser radiation has been presented as an alternative or a coadjutant to conventional, mechanical root surface debridement. The effects on root surface morphology irradiated with Er,Cr:YSGG laser (2.78 μm) or Er:YAG laser (2.94 μm) laser were assessed by SEM; it was found that Er,Cr:YSGG laser-irradiated specimens showed irregular root surface with the appearance of microroughness, with exposed dentinal tubules and no smear layer. The same in the samples irradiated with Er:YAG laser irradiation showed irregular root surface with craters, with exposed dentinal tubules and without a smear layer. 75 The appearance of the smear layer on the treated root surfaces can act as a physical barrier between the periodontal tissues and the root surface inadequate for reattachment of the periodontal tissue. 76
Conclusions
Based on the systematic review results, it can be concluded that the beneficial effects of erbium lasers as an adjunct to SRP have been established. Although all periodontal instruments were efficient in calculus removal from the root surfaces, hand instrument showed much less remaining calculus compared with an ultrasonic instrument. Whereas, on the contrary, calculus removal using the ultrasonic instrument was approximately faster compared with the hand instrument. Erbium lasers revealed no remaining calculus or smaller amounts compared with the conventional instruments when used in appropriate settings. The ability of the Er:YAG laser to eliminate the calculus is comparable with ultrasonic and hand instruments. The efficiency of calculus removal with Er:YAG laser seems to be much higher compared with Er,Cr:YSGG laser. The results showed that ultrasonic instrumentation produced effects on the root surface almost similar to that of hand instrumentation. Er:YAG laser clarifies a little more surface roughness when compared with conventional instruments. Er,Cr:YSGG laser exhibits also rougher surfaces than conventional instruments. The erbium laser-treated root surface was relatively rougher than the conventionally scaled root without important thermal elevation. However, in comparison with conventional instruments, there is an increase in amount of cementum removed when erbium lasers are used.
Further, according to the severity and progression of periodontal disease, the settings of erbium lasers can be adjusted. The results of this review indicate using erbium lasers as an adjunctive therapy to SRP with the following parameters:
Er:YAG laser: 2940 nm, power output of 0.5–1.8 W (50–120 mJ and 10–15 Hz), pulse duration “200 to 400 μs,” 1.5–2 mm noncontact mode, 10°–40° tip angle to the root surface, and 50% air and 70% water irrigation.
Er,Cr:YSGG laser: 2790 nm, power output range of 1.25–1.5 W, short pulse duration “140 to 200 μs,” 1.5–2 mm distance noncontact mode, radial firing tip, 10°–40° tip angle to the root surface, 30–50% air/water irrigation.
These parameters according to this review can be appropriate to remove residual debris from the root surface and at the same time have little or no negative thermal effect on the root surface.
Footnotes
Author Disclosure Statement
No competing financial interests exist.