
Abstract
Objective:
This study aimed to compare the efficacy of diode laser surgery and the scalpel surgery in the removal of inflammatory fibrous hyperplasia (IFH).
Background data:
Diode laser systems are proposed as an alternative to scalpel surgery on surgeries involving oral soft tissues. Some of the advantages of the laser systems are ease of application, adequate coagulation, reduced postoperative pain, and decreased scarring. In addition, there are increasing data on the antibacterial effects of the diode lasers in dentistry; however, the direct bactericidal role of the diode laser in oral soft tissue procedures has not yet been investigated.
Materials and methods:
A total of 22 patients were enrolled in this study. One side of IFH was randomly assigned for excision with scalpel blade or with diode laser. Perioperative bleeding, postoperative pain, wound healing, and bacterial counts were evaluated for both methods.
Results:
The bleeding on the side treated by diode laser was found significantly lower (p < 0.05). A notable reduction in total bacterial counts was observed in the laser group after the first postoperative day. However, this trend did not reach statistical significance. No significant differences were recorded regarding subjective postoperative pain between the groups (p = 0.065). The healing of the postoperative wounds was significantly faster in the conventional group at each time point.
Conclusions:
Diode laser has offered some advantages over conventional method in the management of IFH. However, large-cohort comparative studies are required to provide additional data regarding the wound healing capacity of the diode laser.
Introduction
Inflammatory fibrous hyperplasia (IFH) is an overgrowth of fibrous connective tissue placed over the soft tissues of the vestibular sulcus. 1,2 Although the cause of IFH is multi-factorial, some factors including ill-fitting dentures, poor oral hygiene, smoking, and periodontal disease are frequently associated with this lesion. 1,3 Elimination of the causing factors can lead to a reduction in the size of IFH, but the definitive treatment is surgical removal of the lesion. 4,5 The surgical excision can be performed either with conventional methods such as scalpel blade and electrocautery, or with various types of lasers, including carbon dioxide laser, Erbium:YAG laser, Neodymium:YAG laser, and a diode laser. 3,6
Scalpels have been the instrument of choice for many oral soft tissue procedures due to their ease of use, low cost, precise cutting ability, and favorable wound healing, but the disadvantages include lack of hemostasis of the surgical field and increased postoperative pain and edema. 4,7,8 In addition, in cases where the wound edges are opposed with sutures after the excision of IFH by scalpel, the vestibular sulcus depth and denture bearing area decrease, which may compromise the retention of dentures. Therefore, wound healing by secondary intention would be preferred to avoid the loss of vestibular depth. 1,9 However, since the oral flora involves a broad diversity of aerobes, microaerophilic and facultative anaerobes, the patient's endogenous microflora may contaminate the surgical wounds, particularly those healed by secondary intention, and cause postoperative infections. 10
Diode laser systems are suggested as an alternative to scalpel surgery on surgeries involving oral soft tissues. Diode laser wavelengths (810–980 nm) are highly absorbed by the pigmented tissue, while being poorly absorbed by water. This laser can be used in continuous wave or gated pulse and both in contact and noncontact mode depending on the procedure. 4,11 –13 Diode lasers have several advantages such as ease of use, excellent incision performance, adequate coagulation, reduced postoperative pain and edema, and decreased scarring. 13,14 Furthermore, the bactericidal effect of diode laser through local heating and production of an eschar layer might reduce the risk of postoperative infection during the secondary intention. 14 Therefore, the combination of postoperatively increased vestibular sulcus depth and decreased risk of infection makes diode laser a favorable treatment option for the surgical excision of IFHs.
There is an increasing body of literature on the antibacterial effect of the diode laser on periodontal and root canal treatments; 15 –20 however, the direct bactericidal role of the diode laser in oral soft tissue surgical procedures was not investigated in detail. In this study, we aimed to compare the efficacy of diode laser surgery and scalpel surgery in terms of pain severity, bacterial colonization on wound sites, and wound healing after the removal of IFH.
Materials and Methods
This clinical study was conducted on patients diagnosed with anterior symmetrical IFH lesions who were selected from among those referred to the Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Gazi University. Subjects with systemic diseases that affect the wound healing or those with history of medication use that alters the oral microbial flora, or those who declined to participate were not included in the study. This randomized, split-mouth clinical trial was approved by the local ethics committee (ANK/2011/8-2), and written informed consent was obtained from all individual participants.
For each patient, the sides on which the excisions will be performed through diode laser or scalpel blade were randomly selected by a computer program (Microsoft Office Excel Software 2007, Redmond, WA) that generated random numbers and allowed each side of IFH to receive one of these treatments. The diode laser (Doctor Smile Diode Laser, Vicenza, Italy) was used with 400 μm-fiber tip, 808 nm continuous wavelength, 10 Hz pulse frequency, and 2 W power for ∼4 × 60 sec. Both procedures were performed under local anesthesia by the same trained oral and maxillofacial surgery resident during the same surgical session. While the laser system was in use, protective glasses were worn by the whole clinical team and the patient. The laser tip was initiated by rubbing a piece of articulating paper on the fiber to pick up some pigment. After the excision of IFHs, surgical specimens were fixed in 10% buffered formalin and submitted for histopathological examination. The necessary postoperative instructions were given to the patients. No antibiotics or antiseptic mouthwashes were prescribed. Postoperative controls were performed on the 1st, 2nd, 5th, 10th, 15th, and 30th days after the operation.
The following parameters were evaluated for both surgical methods: (1) perioperative bleeding, (2) postoperative pain, (3) wound healing, and (4) enumeration of bacteria.
Perioperative bleeding was recorded in a categorical (“yes” or “no”) manner. Postoperative pain was evaluated on the 1st, 2nd, 5th, and 10th postoperative day using a visual analog scale, wherein 0 indicates no pain and 10 indicates unbearable pain. The clinical assessment of the wound healing was performed through digital image analysis. The digital photographs of the surgical fields were obtained preoperatively and postoperatively on the 1st, 5th, 10th, 15th, and 30th day. All photographs were taken with Canon Powershot G3 (Tokyo, Japan) in macro mode, auto white balance mode, and maximum pixel resolution (2272 × 1704) under standard fluorescent light and perpendicular to the center point of surgical field with a distance of 30 cm. The digital images were then transferred to a computer and stored in tagged image file format.
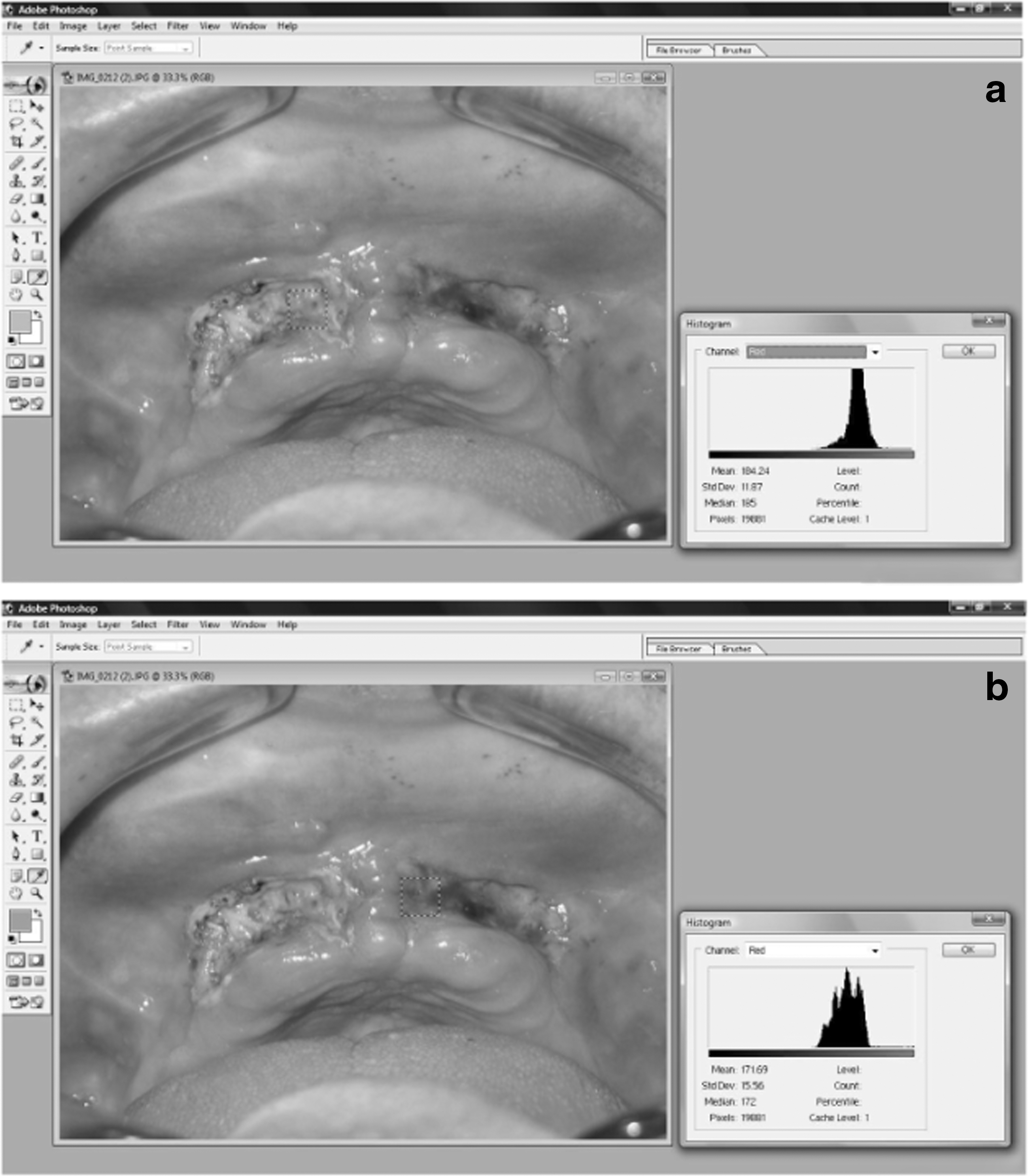
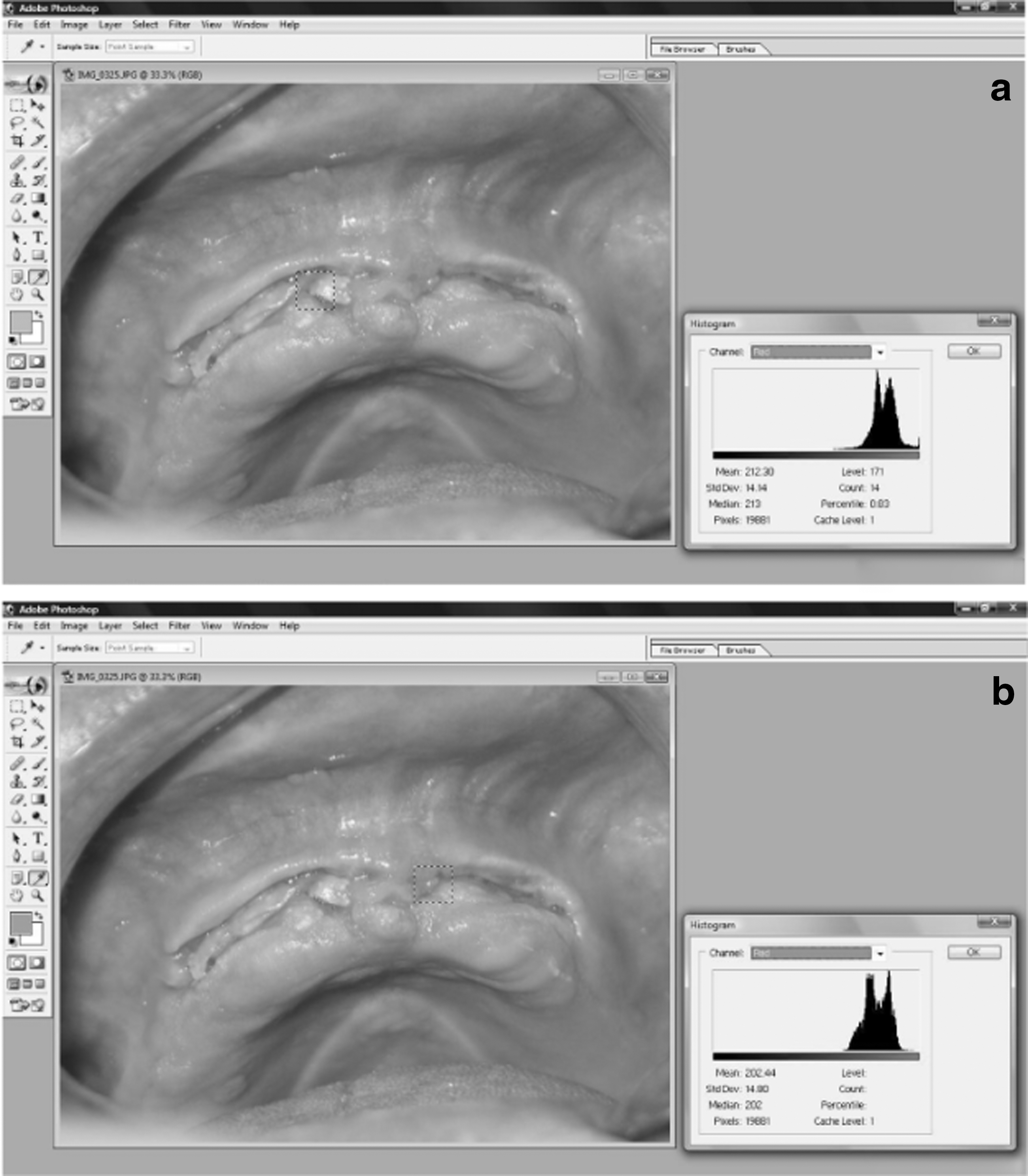
Macroscopic quantification of the wounds was performed using a digital color separation technique with Adobe Photoshop imaging software (CS5 Extended 12.0 × 32; Adobe Systems, San Jose, CA). On the images of surgical fields, regions of two square centimeters were marked with “Rectangular Marquee tool.” “Histogram” mode was opened from the “window-toolbar” menu. The red color channel was selected from “Channel panels menu,” and the values of each surgical wound were recorded. Thereafter, mean values of red color channels were calculated preoperatively from the digital images of surgical fields. According to these values, the healing rates of the tissues in both groups were compared during the follow-up visits. For calibration of the analysis, normal pink gingiva, which was not localized in the surgical field, was selected for each patient, and the pixel value of this area was measured preoperatively. This identical pixel value was checked before the photographs were used for image analysis for evaluating erythema, granulation tissue as well as epithelialized tissue in the surgical field.
For bacterial counts, samples from both surgical fields were collected using a sterile cotton swab at different time intervals as mentioned. The first sample was taken preoperatively, and the other samples were taken postoperatively on the 1st, 2nd, 5th, and 10th days. Initially, oral secretions and debris from surface of the wound were removed with a sterile gauze, then the cotton applicator was placed on the deepest portion of the surgical field and gently rotated on the affected area for 30 sec. The samples were placed into sterile screw-capped tubes containing 1 mL of thioglycolate broth (Merck, Germany) medium, and were delivered to the microbiology laboratory immediately. After vortexing for 1 min to elute the bacteria from the swab into the broth medium, serial dilutions (10−1 , 10−2 , and 10−3 ) were performed to provide a more reliable counting. One hundred microliters of original sample (nondiluted) and each dilution were incubated on the media of Colombia agar (Merck) supplemented with 10% sheep blood agar, vitamin K1 (1 μg/mL), and hemin (5 μg/mL), and tryptic soy agar (40 g/L) with yeast extract (1 g/L), bacitracin (75 μg/mL), vancomycin [5 μg/mL; Trypticase Soy-Bacitracin-Vancomycin agar (TSBV)] supplemented with 5% horse serum under the condition of 37°C and 5% CO2 (HealForce®, China) for 4–5 days for microaerophilic species. Schaedler agar (Merck) supplemented with 10% sheep blood agar, vitamin K1 (1 μg/mL), and hemin (5 μg/mL) at 37°C in an atmosphere of 10% H2, 10% CO2, and 80% N2 was used for facultative anaerobe species. After the incubation period, the grown colonies were counted. Aerobic strains were identified according to conventional microbiological tests (culture, colony morphology, Gram staining, catalase, coagulase tests, etc.). Anaerobic species' identification was carried out by the newly passaged cultivation on 5% sheep blood agar-supplemented Schaedler agar medium from the initial medium in an anaerobic chamber (Electrotek, United Kingdom) with an atmosphere of 10% H2, 10% CO2, and 80% N2. Chocolate agar medium was used for the aerotolerance testing of the growing colonies. Bacteria that were confirmed as anaerobes were classified according to the Clinical Laboratory Standards Institute criteria 21 on the basis of colony morphology, hemolysis on blood agar, Gram staining, pigment production, fluorescence production under long-wave ultraviolet light (λ = 366 nm), catalase testing (15% hydrogen peroxide), spot indole test (dimethylaminocinnamaldehyde; Becton Dickinson®), serological and biochemical properties, results of disk susceptibility testing [colistin 10 μg/disk, kanamycin 1000 μg/disk, and vancomycin 5 μg/disk (Bioanalyse®, Turkey)]. The number of bacterial colonies each that were grown in aerobic/microaerophilic and anaerobic atmospheric conditions was determined in colony forming units per milliliter (CFU/mL) and normalized by the coefficient of the dilution ratios.
For statistical analysis of the data, the Kolmogorov–Smirnov test was used to evaluate the distribution of measurement variables. Except for the bacterial count data, which were transformed to logarithmic scale to ensure a normal distribution, all data were normally distributed (p < 0.05). Repeated-measures analysis of variance (ANOVA) was used to compare the outcomes of the two treatment modalities, and the Duncan test was performed to compare the differences between the time points. In addition, the paired “t” test was used for the comparison of intragroup data with the first measured data. A p-value of <0.05 was considered statistically significant for all analyses. All analyses were performed using SPSS Version 17.0 (SPSS, Inc., Chicago, IL).
Results
A total of 22 patients were enrolled in this study (14 females and 8 males). The ages of the participants ranged from 38 to 79 years. Almost all the conventional surgery procedures were carried out under conditions of continues bleeding. On the sides treated with diode laser, no perioperative bleeding was recorded (p < 0.05).
Patients from both laser and conventional groups experienced a reduction in pain over time. No significant differences regarding subjective postoperative pain were noted between the groups (p = 0.065). Likewise, an improvement in the wound healing was observed with time in both groups. However, based on the mean values of the preoperative red color channels of the surgical fields obtained by digital image analysis the clinical healing of the postoperative wounds was found statistically faster in the conventional group at each time point; p = 0.018 on day 1, p = 0.024 on day 5, p = 0.014 on day 10, p = 0.015 on day 15, and p = 0.004 on day 30 (Figs. 1 –4).

Clinical aspect of a patient with IFH before treatment. IFH, inflammatory fibrous hyperplasia.

Two patients were excluded from the microbiological evaluation of the surgical wounds due to the improbable growth of their colonies in samples. Gram-positive bacterial species such as Staphylococci (Coagulase-negative Staphylococcus), Staphylococcus aureus (S. aureus, methicillin-sensitive S. aureus), α-hemolytic Staphylococci, Viridans Streptococci, and Diphtheroid bacilli were identified in the microbiological evaluation of the aerobic and microaerophilic commensal oral flora. The number of Gram-positive species was found to be higher compared with the facultative anaerobic Gram-positive species, such as Peptostreptococcus sp. and Actinomyces sp., and Gram-negative species, such as Prevotella sp., which have crucial potentials in the etiopathogenesis of the oral diseases. When the microbiological data from 20 patients were statistically evaluated, no significant differences were found in the number of facultative anaerobic (p = 0.819), aerobic (p = 0.197), and total bacterial load (p = 0.586) on the 1st, 2nd, 5th, and 10th postoperative days between the laser and conventional treatment groups (Figs. 5 –7).

Counts of the facultative anaerobic bacteria in the scalpel and laser groups (─: mean value).

Counts of the aerobic bacteria in the scalpel and laser groups (─: mean value).
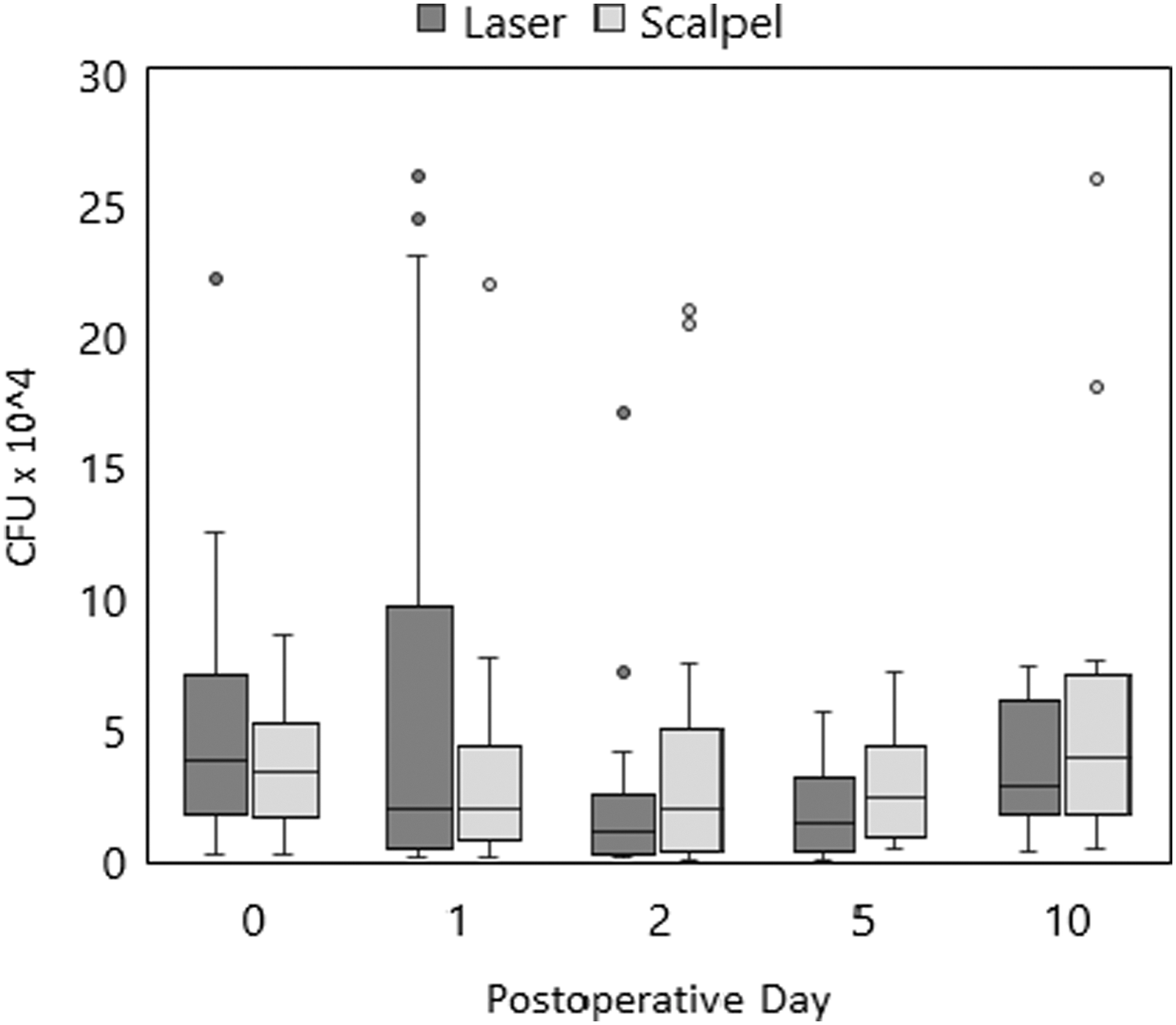
Total bacterial load in the scalpel and laser groups (─: mean value).
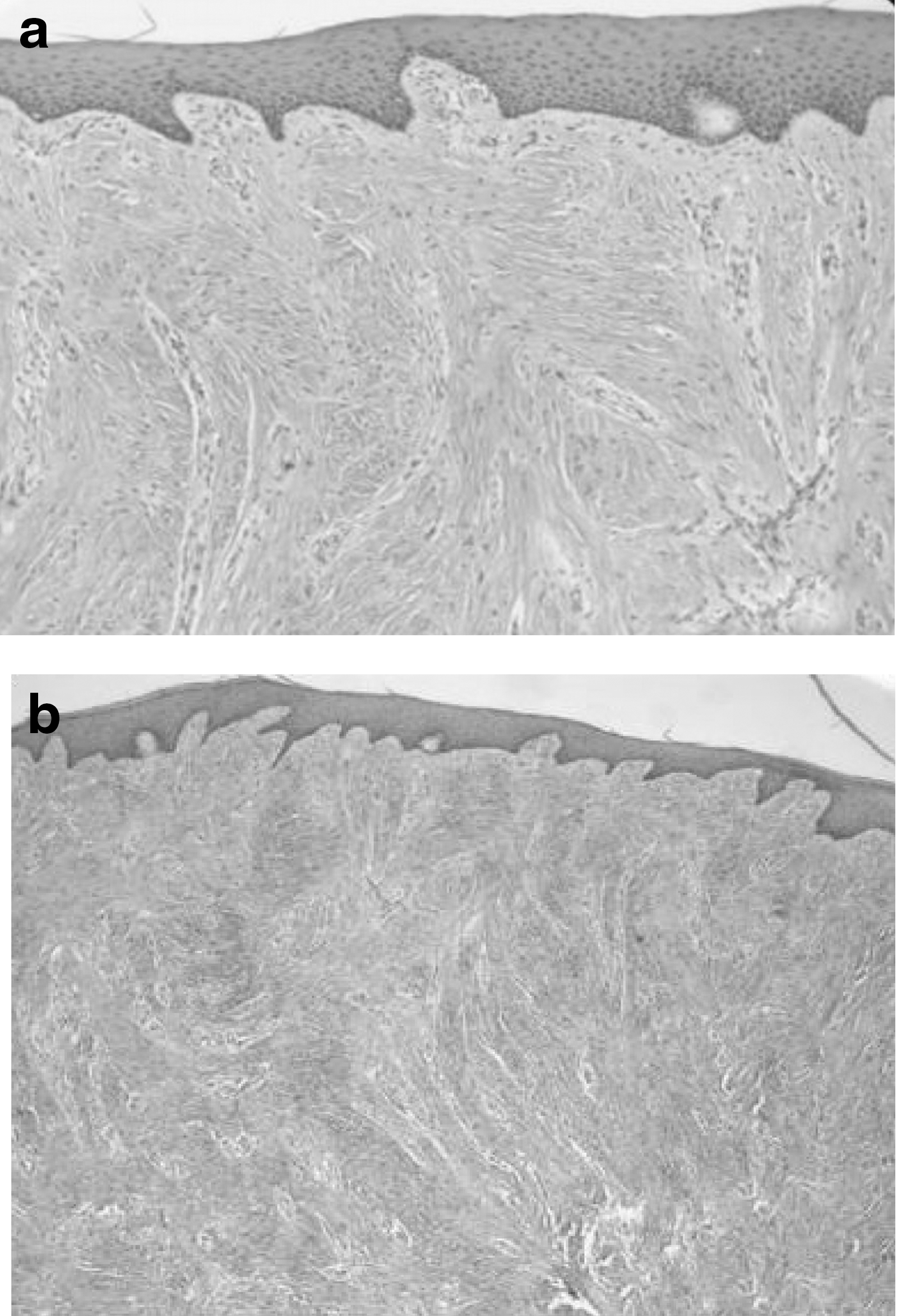
The histopathological examination of lesions revealed hyperplasia of stratified squamous epithelium, which was sometimes accompanied by surface ulcerations. The underlying connective tissue stroma showed thick collagen fibers in bundles with varying numbers of chronic inflammatory cells (Fig. 8). The preoperative diagnosis of IFH was confirmed histopathologically in all specimens. In addition, no significant thermal tissue damage preventing an accurate histopathological diagnosis of the specimens was noted in the laser group.
Discussion
This study aimed to compare the use of diode laser and scalpel surgery in the removal of IFH. The results of this study showed that both techniques were effective in the treatment of fibrous hyperplasia. However, a blood-free operation field, elimination of the need for sutures, and the antibacterial efficacy can make diode laser a favorable alternative to the scalpel surgery among oral soft tissue procedures.
Specific wavelengths of the diode laser are highly absorbed by the pigmented tissues. Thus, this laser system provides excellent hemostasis during the soft tissue surgeries. 11,22,23 In this study, the conventional surgery procedures were carried out under conditions of continues bleeding. No suturing was used to maintain the depth of vestibule sulcus and to be able to perform digital image analysis on the surgical wounds. Only in cases where hemostasis could not be achieved by compression with gauze, the bleeding focus was sutured with 4.0 polyglycolic acid without leading to a change in the wound surfaces.
By comparison, the laser surgery provided a blood-free operation field, and no additional hemostatic measures were required. The higher coagulation properties of the diode laser have been shown in several other studies. 4,12,13,23,24 Although the duration of the procedures was not measured in this study, no need for bleeding control shortened the duration of surgery in the diode laser group. This observation was confirmed by Amaral et al. 4 who compared diode laser surgery with conventional method in the removal of IFH.
In this study, postoperative pain was reduced gradually from the 1st postoperative day to 10th postoperative day, and all patients reported either no pain or only mild pain on the 2nd postoperative day. Moreover, no significant difference in postoperative pain was found between the groups. Since the removal of fibrous hyperplasia on both sides was performed at the same session, patients might not be able to distinguish the level of pain on different surgical fields. However, other recent studies, in which the laser and conventional surgery groups involved different patients with IFH, have also reported no significant differences in postoperative pain. 4,6
The elimination of bacteria and sterilization of the operation site are well-known benefits of the diode laser surgery. 25,26 Nonetheless, there is a lack of information on the direct antibacterial effect of diode laser after oral soft tissue surgeries. This study compared the efficacy of diode laser and conventional method in reducing the bacterial load of the surgical field after the removal of IFH through a detailed microbiological assessment. However, no significant differences were found between the groups regarding the number of aerobic and facultative anaerobic bacteria. This can be explained by the fact that each patient in this study served as his or her own control, and the bacterial colonies in both surgical wounds could easily contaminate each other, thereby may lead to similar count of bacteria in both groups. Nevertheless, a notable reduction in total bacterial counts was observed in the laser group after the first postoperative day, which may indicate an antibacterial effect of the diode laser. Besides, after the elimination of bacteria from the surgical field with laser irradiation, endogenous aerobes and anaerobes can recolonize the wound as part of normal oral flora. 27 This can also be noticed in this study with increasing bacterial count in the laser group after the fifth postoperative day.
Nowadays, diode laser has become a treatment of choice in many procedures in dental and oral surgery due to its potential clinical benefits. However, collateral tissue damage that can cause a delay in wound healing is one of the leading drawbacks of the diode laser surgery. 12,13 Generally, subjective assessment methods are used for the evaluation of wound healing in clinical studies. But quantitative measurements are crucial when comparing the effects of applied treatments. 28 Therefore, digital image analysis was preferred to assess wound healing in this study. This objective assessment enabled the authors to record the progress of healing and compare the therapeutic effects of both treatment modalities.
Some recent studies have suggested that using high power diode laser can deliver adequate doses of light into deeper tissue and induce photobiomodulation. 29,30 In brief, photobiomodulation works with improving mitochondrial energy production by stimulating the cytochrome c oxidase and leading to increased production of adenosine triphosphate, free reactive oxygen species, and nitric oxide. These heightened metabolic activities accelerate cellular proliferation and migration, and consequently promote wound healing. 31,32 However, in this study healing process was found significantly slower in diode laser group throughout the follow-up period. In some of our cases, charring of tissue was observed in the laser group. This was probably a result of inadequate hand speed of the resident surgeon since moving the laser tip throughout the surgical field very slowly can result in increased thermal damage to the tissues. 33 This may also explain the delayed healing with laser group in this study. Similarly, increased collateral thermal damage caused by diode laser irradiation on soft tissues leading to increased inflammatory reaction and delay in wound healing was also reported by other many studies. 4,7,11,13,34
The diversity of parameters associated with lasers (i.e., the wavelength, output power, frequency, and pulse duration), sample population in each study, types of surgeries performed, surgeon's skill, and/or assessment methods might be the cause of the differences in the results of these studies. Furthermore, the lesion sizes may play an essential role in the healing of the surgical field after the diode laser surgery. Some authors have advocated that the use of diode laser can give better results in surgical removal of small oral exophytic lesions. 12,13 Similarly, in a randomized clinical trial, the reason of slower healing process and more swelling with the surgical use of diode laser was explained by the fact that larger lesions can result in more thermal damage to the tissues. 4
To the best of our knowledge, this is the first report in the literature that evaluated the direct bactericidal effect of the diode laser on the surgical removal of IFH. Other important outcomes for use of diode laser in oral soft tissue surgery were also presented in this study. Nevertheless, some limitations must be noted. Due to the design of the study, the procedures of both sides were performed during the same operative session, and there was no group blinding. These factors might cause an outcome bias associated with the individual variables. Further studies are needed to evaluate the effect of different setting parameters and the size of the lesion in wound healing process after diode laser surgery.
Conclusions
In conclusion, diode laser has offered essential advantages over conventional method in the management of IFH: superior hemostatic ability, absence of suture need, and antibacterial efficacy. This less invasive treatment modality may also improve patients' compliance during the operation and increase their postoperative satisfaction. However, double-blind comparative studies with larger cohort are required to provide additional data regarding the wound healing capacity of the diode lasers with different parameters in oral surgery.
Footnotes
Acknowledgments
The authors would like to thank Prof. Dr. Serpil Cula for her assistance with statistical analysis.
Author Disclosure Statement
No competing financial interests exist.