
Abstract
Objective:
To evaluate the use of photobiomodulation therapy (PBM-T) in patients undergoing chemotherapy and/or radiotherapy and affected by oral mucositis (OM).
Background:
Few clinical studies have evaluated PBM-T, particularly in combination with photodynamic therapy (PDT), for the treatment of OM.
Methods:
Thirty-one patients were divided by convenience into two groups. One received PBM-T (n = 17) alone, consisting of low-intensity laser (LIL) irradiation (wavelength 660 nm, continuous mode, spot energy 4 J, energy density 142 J/cm2, irradiation time 40 s per spot), once weekly for 4 weeks. The other (n = 14) received a combination of PBM-T and PDT, with curcumin as photosensitizer. Patients were instructed to rinse their mouth with 20 mL of curcumin solution for 5 min. The oral cavity was irradiated with a blue light-emitting diode (power 1200 mV, wavelength 468 nm) for 5 min. LIL was applied as in the PBM-T group. After treatment, OM severity was reassessed. The results were analyzed by the Wilcoxon and Mann–Whitney tests.
Results:
Both PBM-T alone and PBM-T+PDT yielded significant reductions in OM grade (p < 0.01). PDT+PBM-T resulted in a significantly shorter healing time compared with PBM-T alone (p = 0.0321).
Conclusions:
Within the parameters of this study, PBM-T+PDT was an effective method to accelerate the OM healing process.
Introduction
Many cancer patients undergo radiotherapy and chemotherapy in an attempt to destroy tumor cells; however, such treatments may be associated with adverse effects. In cases related to head and neck cancer, the ionizing effects of radiotherapy may cause some degree of oral mucositis (OM) in 90–97% of patients. 1 OM is an acute inflammation of the mucosa caused by a decrease in basal cell renewal in the epithelium due to the effects of chemotherapy and especially radiotherapy. 2 The pathogenesis of OM involves the death of basal epithelial cells due to exposure to the free radicals generated by radiation or chemotherapy. Free radicals activate cell receptors that stimulate expression of proinflammatory cytokines and cause tissue injury and cell death, leading to mucosal lesions. Viral and bacterial pathogens present in the oral microbiota can increase the severity of these lesions. 3 The inflammatory picture caused by OM can lead to pain and difficulty with speech and swallowing, and ulcerations can lead to predispositions to local or systemic infections. 2 In more severe cases, lesions may interrupt radiotherapy treatment.
Cancer patients may use some prophylactic measures for pain, such as cryotherapy, chlorhexidine gluconate, oral hygiene, and mouth rinse. 4 However, these measures are not able to act directly on the biological mechanisms involved in each phase of OM. Meanwhile, photobiomodulation therapy (PBM-T) is able to penetrate the tissue and exert analgesic and healing effects for the patient, being an alternative for prevention and treatment of OM. 5
Currently, PBM-T is used for the control of OM in patients undergoing cancer treatment. 6 PBM-T is a form of nonthermal light therapy that utilizes nonionizing light sources, including lasers, light-emitting diodes (LEDs), and broadband light, in the visible and infrared spectra. It works by sensitizing endogenous chromophores that trigger photophysical and photochemical effects at a biological scale. 7,8 Energy absorption and transfer to cells and tissues are mediated by cytochrome c and an oxygen-independent extracellular pathway involving activation of growth factors, such as TGF-β1. 9,10 Other chromophores, such as ion-channel receptors, have recently been observed to increase ATP production and induce changes in mitochondria and calcium levels. The majority of cell chromophores, including flavins, iron/sulfur centers, and heme, are located in the mitochondria; thus, light/cell interactions are essentially light/mitochondria interactions. 11 These interactions achieve anti-inflammatory, analgesic, immunomodulatory, and biostimulant effects, speeding the healing of mucosal lesions, including OM. 6,7,12 The secondary effects of PBM-T can be short term, such as increased blood flow, greater oxygen consumption, and improved tissue ATP production, or can be more long term in nature, such as increased antioxidant defenses, activation of transcription factors, and alteration of the expression pattern of cytokines and growth factors. 12,13 Thus, PBM-T is an effective treatment and is indicated in the repair of oral tissues and analgesia when pain occurs as a manifestation of OM. 14,15 Brandão et al. 16 found that PBM-T did not impact treatment outcomes of primary cancer, recurrence rates, onset of new primary tumors, or survival in patients with advanced oral squamous cell carcinoma.
Another therapy that has proven to be effective in the treatment of OM is photodynamic therapy (PDT). 6 PDT is an interaction between a photosensitizing compound and oxygen, which reacts in the presence of light of an adequate wavelength, 6,17,18 resulting in the production of reactive oxygen species known as singlet oxygen and free radicals. 17,19,20 The high reactivity of singlet oxygen with biomolecules means that it is has generally been considered an endpoint in the cascade of oxygen-scavenging agents (Wentworth et al.). 21 These products are capable of irreversibly damaging cellular components of microorganisms, modifying their metabolic activities. Photosensitizers have a high degree of selectivity in killing microorganisms and show little toxicity to host cells. 22 Currently, methylene blue, toluidine blue, porphyrins, erythrosine, rose Bengal, and curcumin are among the most used photosensitizers. 18 Arany 23 reported that various forms of biophotonic treatments are used in oncotherapy, with slight differences in their ability to evoke underlying pathophysiological responses. The most well characterized among these is antitumor PDT, which uses an exogenous chromophore (usually a dye or antibody-conjugated nanoparticle). The chromophore-decorated tumor cell or stromal vasculature is then selectively destroyed by biophotonic illumination.
Curcumin is the main constituent of turmeric powder, extracted from the rhizomes of turmeric, a plant used in traditional Indian medicine. 24 It exhibits significant antimicrobial properties against gram-positive and gram-negative bacteria, 17 and has a direct application in dentistry as an important substance in the disinfection of the oral environment. 19 Low concentrations of curcumin do not cause damage to oral tissues; on the contrary, it is a photosensitizer indicated in the treatment of oral infections. 25,26 When curcumin is irradiated by light sources at a wavelength of ∼450 nm, it promotes a photodynamic effect that can destroy microbial pathogens. 27 –29
Among several forms of OM prevention, PBM-T stands out as an effective alternative in the prevention and treatment of this disease, proving to be a low-cost, nontraumatic therapy with good results. The combination of PBM-T with an antimicrobial therapy, such as PDT, can speed the OM healing process by promoting disinfection of the oral cavity.
Within this context, the aim of the present study was to evaluate the clinical application of PBM-T and PDT in cancer patients with OM. The null hypothesis was that PBM-T and PDT would not be associated with improvement in OM.
Materials and Methods
The present study was approved by the Ethics Committee of Pontifícia Universidade Católica de Campinas, Campinas, SP, Brazil (protocol number 1.823.296).
The study used a comparative, nonrandomized interventional design. Thirty-one patients were selected in the Oncology Sector of the Hospital of Pontifícia Universidade Católica de Campinas, Campinas, SP, Brazil, and an informed consent form was signed by patients or responsible parties. For patients to be included in this study, they had to meet the inclusion criteria. Patient selection took place prospectively between February and December 2017.
The minimum number of 14 patients per group was obtained from the sample calculation. ANOVA was used for the sample calculation, with a minimum difference between treatments, mean of 0.09, error standard deviation of 0.067, number of treatments 4, test power of 0.80, and alpha of 0.05. The minimum number of patients per group was determined to be 14.
Patients presented with oral mucositis with scores of 1 to 4 according to the classification of the National Cancer Institute, Common Toxicity Criteria (WHO) 1998
30
: Patients undergoing cancer treatment. Patients or responsible parties who were authorized participation in the study and signed an informed consent form. Patients who made use of other prophylactic measures for mucositis, such as use of oral glutamine, steroids, immunoglobulin, vitamins, and chlorhexidine, among others.
2
The patients were evaluated clinically by an oncologist, with experience in diagnosis of OM, who assessed the grade of mucositis present in the oral cavity according to the 1979 WHO classification (Table 1). Clinical examination focused on clinical signs (erythema, ulceration) and whether the patient was able to ingest solids or only liquids. Assessment of the grade of mucositis present in the oral cavity was done before and after PBM-T or PBM-T+PDT.
Scale Used for Evaluation of Mucositis
Source: National Cancer Institute, Common Toxicity Criteria (WHO). 16
The patients were divided for convenience into two groups (Fig. 1). The exclusion criteria for group PBM-T+PDT were as follows: inability to rinse the oral cavity with the photosensitizer (due to gag reflex or functional limitations caused by the tumor) and intubated patients; these were allocated to the PBM-T group.
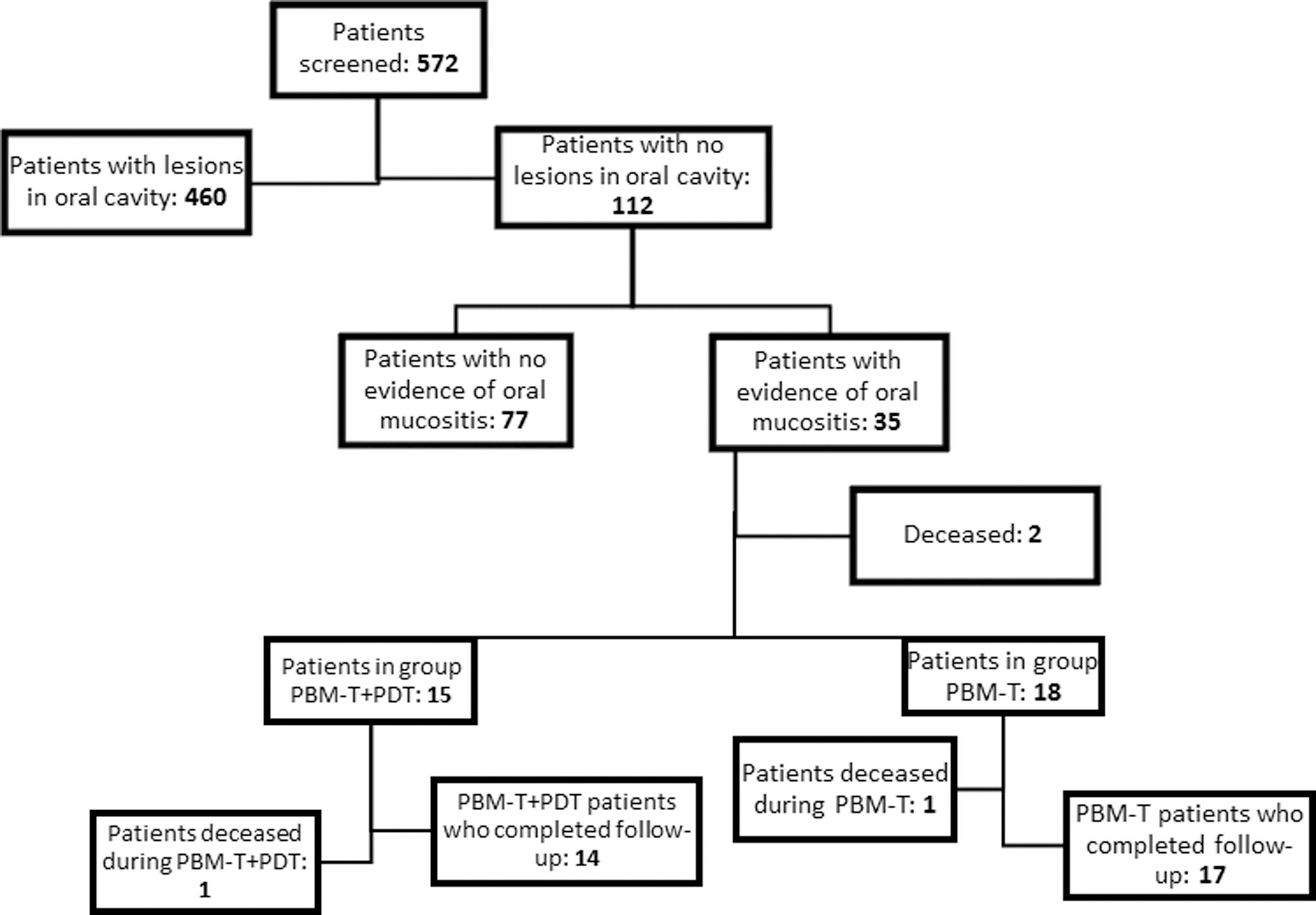
Flow diagram of patient inclusion and group allocation.
Group: PBM-T
PBM-T: low-intensity laser (LIL) (DMC, São Carlos, SP, Brazil) was applied at a wavelength of 660 nm, in continuous mode, with the following settings: spot size 0.028 cm2, mean power (output) 100 mW, spot energy 4 J, energy density 142 J/cm2, and irradiation time 40 s per spot. PBM-T was applied to the lips (4 points on the upper lip and 4 points on the lower lip, Fig. 2), labial commissure (1 point on each side), tongue dorsum (3 points), floor of mouth (1 point on each side), hard palate (3 points), soft palate (3 points), jugal mucosa (10 points on each side), and side of tongue (10 points on each side), totaling 61 points as shown in Figs. 3 –5. This protocol was followed once a week for 4 weeks. Many patients lived in cities far from the study hospital, which made it unfeasible for them to return exclusively for PBM-T. Thus, the once-weekly PBM-T sessions were timed to coincide with patients' scheduled medical follow-up appointments.

Clinical image demonstrating PBM-T. PBM-T, photobiomodulation therapy.
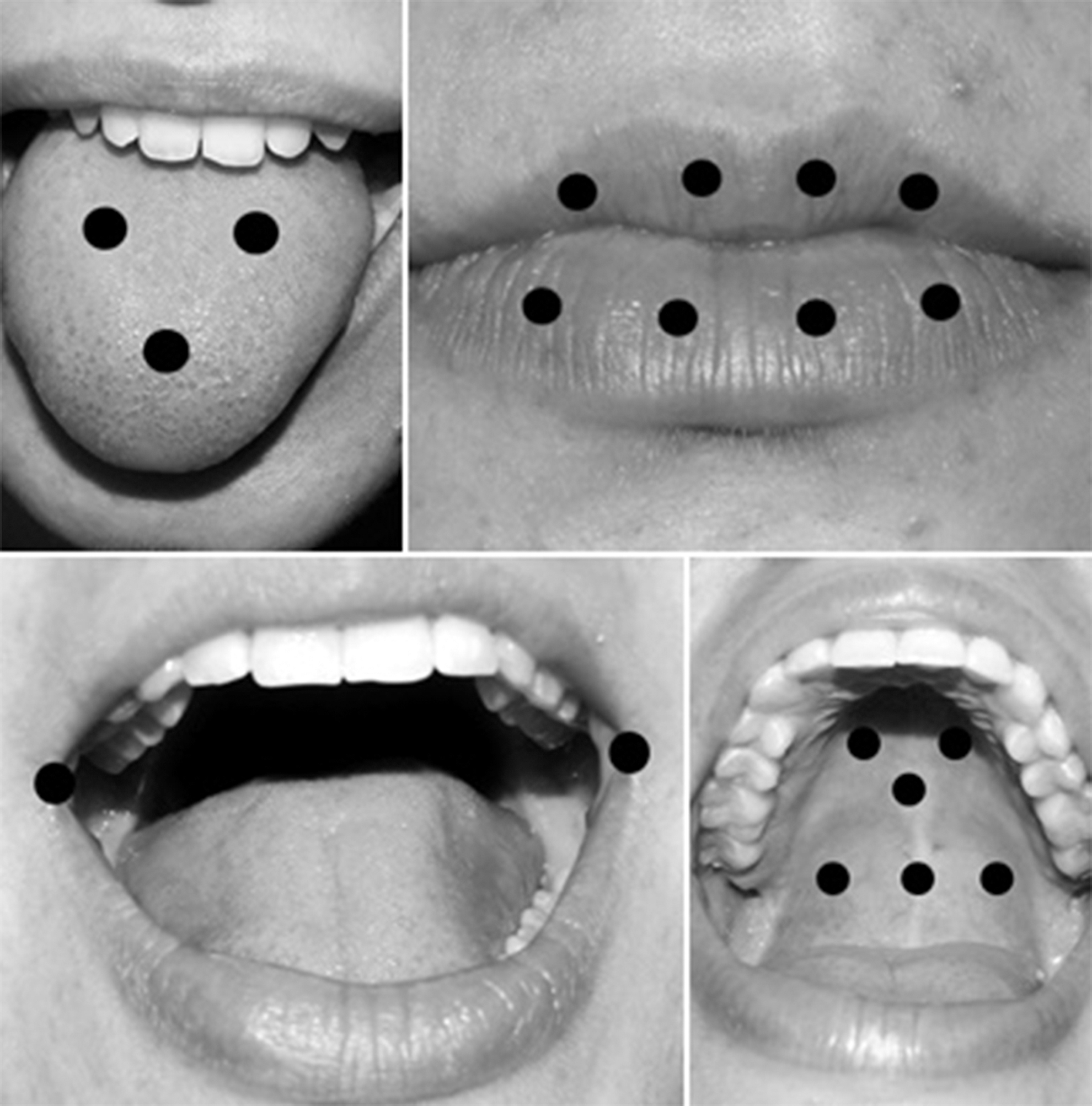
Clinical image demonstrating PBM-T irradiation sites. The laser probe is represented by black circles. Three points on dorsum of tongue; four sites on upper lip and four on lower lip (eight points); one point on each side of labial commissure (two points); three points on hard palate; and three points on soft palate (six points). PBM-T, photobiomodulation therapy.
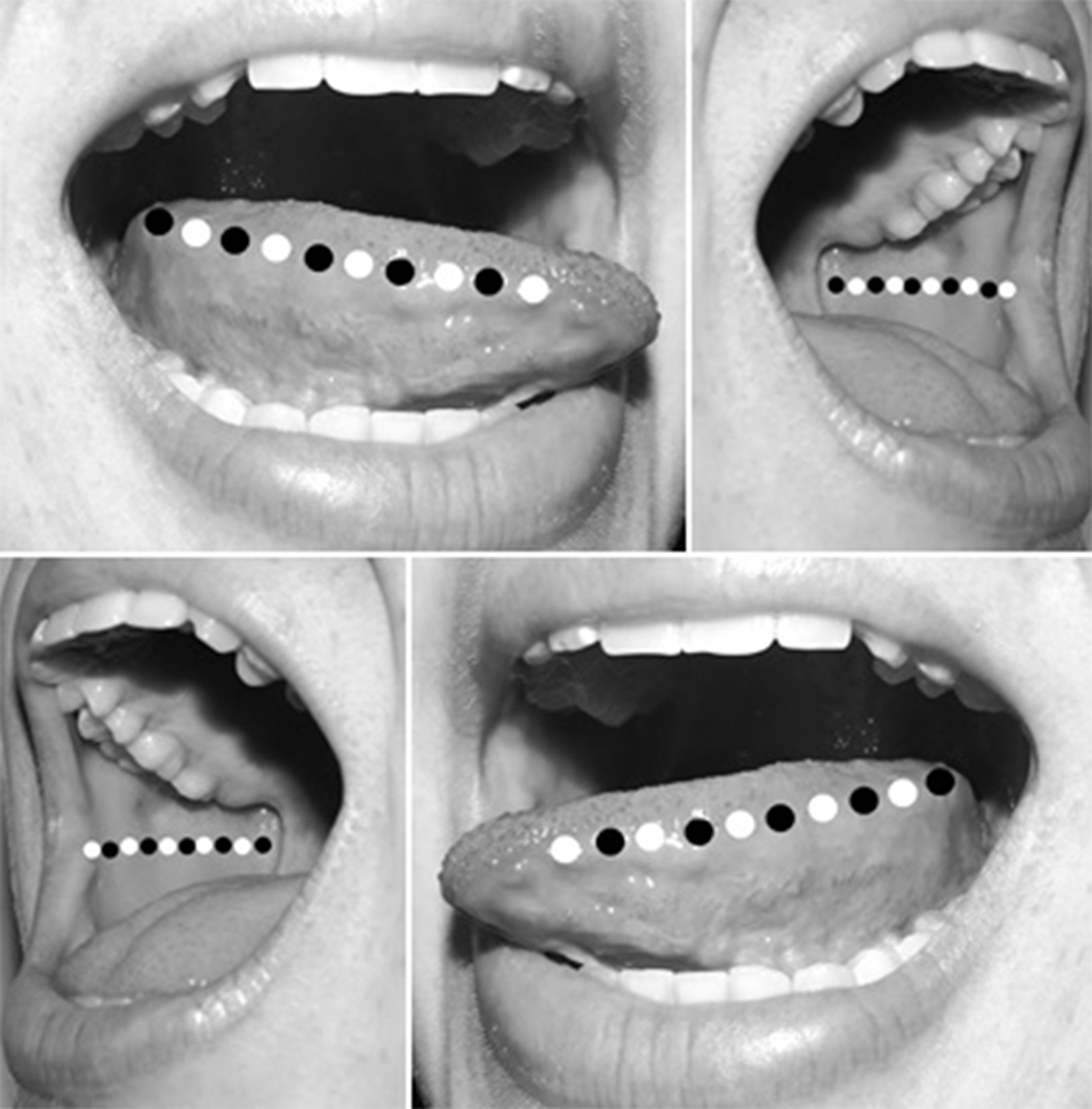
Clinical image demonstrating PBM-T irradiation sites. The laser probe is represented by black and white circles. Ten points on each side of the tongue (20 points) and 10 points on each side of the jugal mucosa (20 points). PBM-T, photobiomodulation therapy.
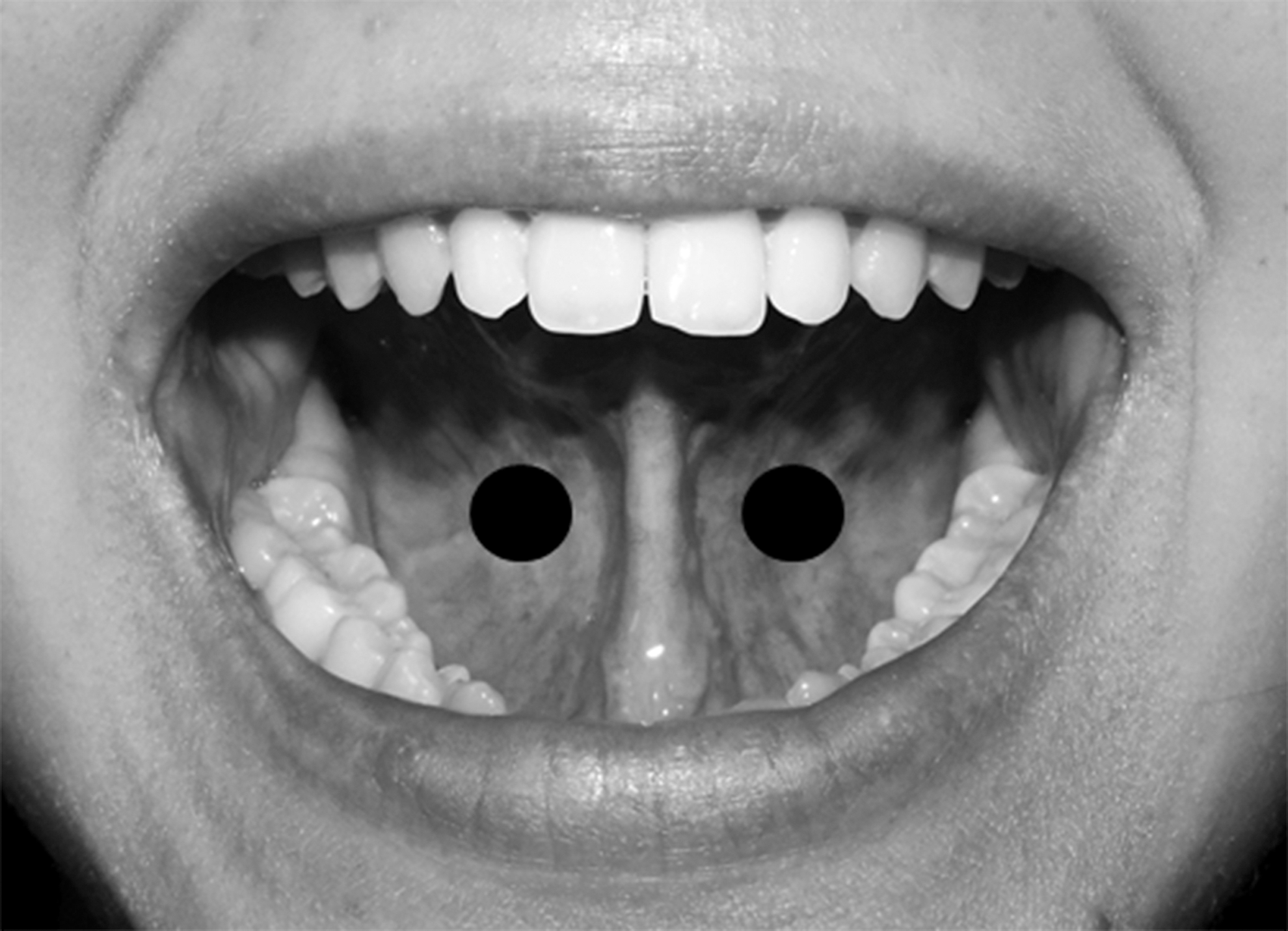
Clinical image demonstrating PBM-T irradiation sites. The laser probe is represented by black circles. One point on each side of floor of mouth (two points). PBM-T, photobiomodulation therapy.
Group: PBM-T+PDT
PDT was performed using curcumin as photosensitizer (concentration of 1.5 g/L) (adapted from Andrade et al.). 26 The patients were instructed to rinse their mouth with 20 mL of solution for 5 min, and then discarding it. The oral cavity was then irradiated with blue LED (Ultralumen SL; Sander do Brasil Ltda., MG, Brazil) with 1200 mV of power and wavelength of 468 nm, for 5 min. Subsequently, the application of PBM-T was combined with PDT according to PBM-T parameters (Fig. 6).

Blue LED irradiation after mouth rinse with curcumin (PDT). LED, light-emitting diode; PDT, photodynamic therapy.
After treatment, the OM grade of the patients was evaluated again according to the WHO (1979) 30 (Table 1). There were no cases of additional or second-look application of PBM-T to the patients included in the study. The follow-up period was 6 months, at which time patients underwent clinical reassessment, performed by the same experienced oncologist who carried out baseline evaluation, to ascertain whether OM had recurred and whether any adverse effects of photobiomodulation had occurred.
The results were analyzed in the Biostat 4.0 program and submitted to the Shapiro–Wilk test. The sample showed non-normal distribution. The results of OM grade before and after application of PBM-T or PBM-T+PDT were analyzed with the Wilcoxon test, while time to healing of OM was analyzed by the Mann–Whitney test, both with a significance level of 5%.
Results
Most patients included in the study had breast neoplasms (35.29% of the PBM-T group) and carcinomas (28.57% of the PBM-T+PDT group). The majority was female (70.59% in PBM-T, 57.15% in PBM-T+PDT). In descending order of frequency, the initial degree of mucositis in the PBM-T group was I in 41.17%, III in 35.29%, and II in 23.52%; in the PBM-T+PDT group, equal proportions had grade I and III (35.71% each), followed by grade II (28.57%) (Table 2). There were no patients with grade IV mucositis in the sample.
Demographic and Clinical Profile of Sample
OM, oral mucositis; PBM-T, photobiomodulation therapy; PDT, photodynamic therapy.
There was a significant reduction in OM grade after the application of PBM-T or PBM-T+PDT (p < 0.01) (Figs. 7 –10). There was no significant difference between using only PBM-T or PBM-T combined with laser in the remission of mucositis after irradiation (p > 0.05, Table 3 and Fig. 11). The likelihood of treatment success (OM score 0) was similar after PBM-T or PBM-T+PDT. Of the 17 patients treated with PBM-T, 15 achieved score 0; of the 14 patients who received PBM-T+PDT, 12 achieved score 0 (odds ratio 1.0294, p = 0.8337, 95% confidence interval 0.3647–2.9055, Table 4).

OM before PBM-T. OM, oral mucositis; PBM-T, photobiomodulation therapy.

OM after PBM-T. OM, oral mucositis; PBM-T, photobiomodulation therapy.

OM before PBM-T+PDT. OM, oral mucositis; PBM-T, photobiomodulation therapy; PDT, photodynamic therapy.
OM after PBM-T+PDT. OM, oral mucositis; PBM-T, photobiomodulation therapy; PDT, photodynamic therapy.

Arithmetic means of OM grade before and after application of PBM-T or PBM-T+PDT. PBM-T, photobiomodulation therapy; PDT, photodynamic therapy.
Medians (Md) and Quartile Deviations (D) of Oral Mucositis Grade Before (Pre) and After (Post) Application of Photobiomodulation Therapy or Photobiomodulation Therapy+Photodynamic Therapy
Different letters in row indicate statistically significant difference. Wilcoxon test, significance accepted at 5%.
D, quartile deviation; Md, median; PBM-T, photobiomodulation therapy; PDT, photodynamic therapy.
Estimative of Effective Treatment of Oral Mucositis Before (Pre) and After (Post) Application of Photobiomodulation Therapy or Photobiomodulation Therapy+Photodynamic Therapy
CI, confidence interval; Md, median; OM, oral mucositis; PBM-T, photobiomodulation therapy; PDT, photodynamic therapy.
In a manner consistent with the dose/response concept of hormesis, 31 the spot energy of 4 J was associated with improvement in OM grade, suggesting that the applied dose, irradiation time, and irradiation sites were all consistent with the PBM-T energy level needed to treat OM.
PBM-T+PDT resulted in a shorter healing time for OM compared with PBM-T alone (p = 0.0321, Table 5 and Fig. 12). Healing of OM averaged ∼17 days with PBM-T alone, whereas healing with PBM-T+PDT required ∼12 days.
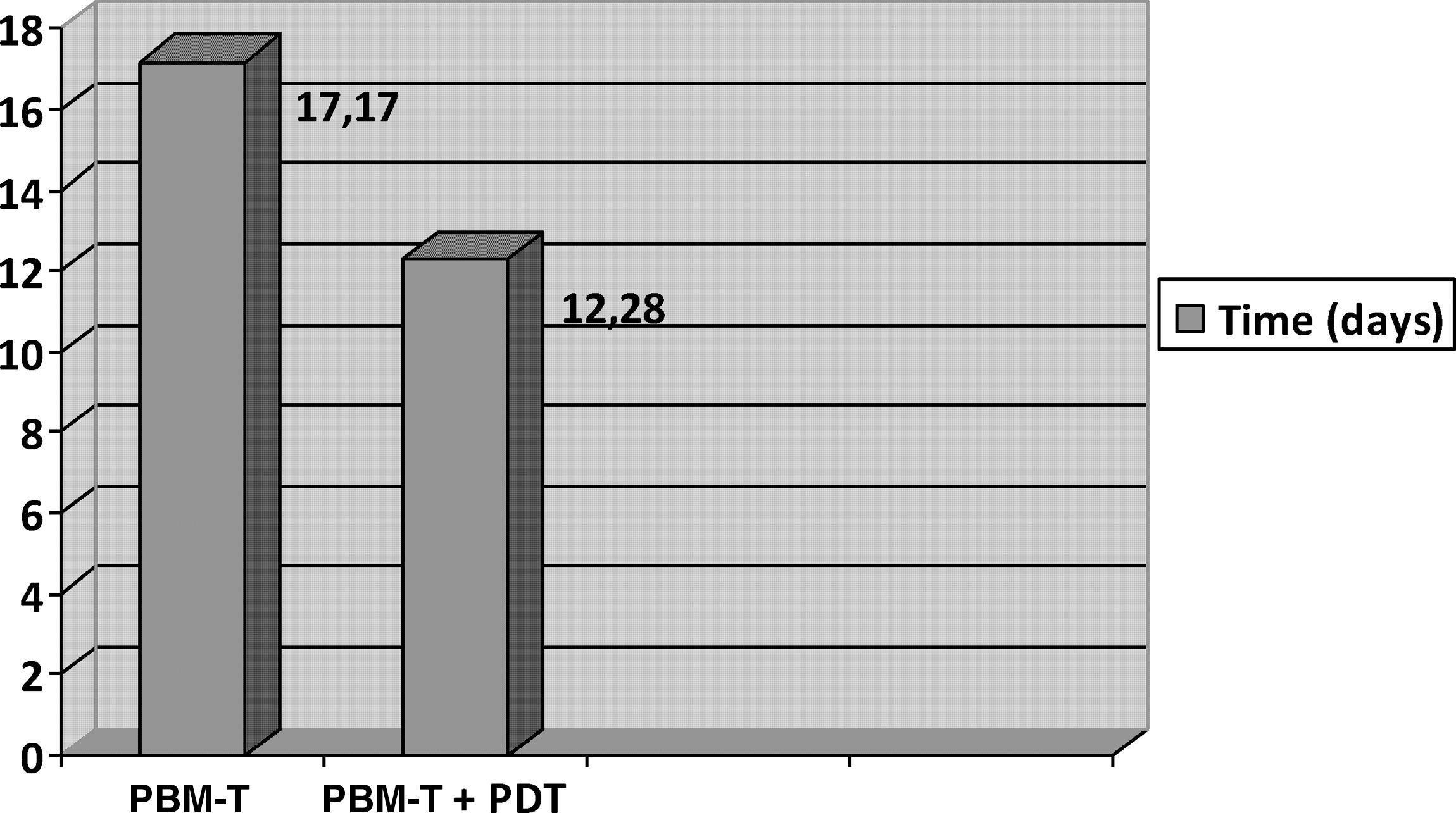
Arithmetic means of time needed for healing of OM (days) after application of PBM-T or PBM-T+PDT. OM, oral mucositis; PBM-T, photobiomodulation therapy; PDT, photodynamic therapy.
Medians (Md) and Quartile Deviations (D) of Time Needed for Healing of Oral Mucositis (Days) After Application of Photobiomodulation Therapy or Photobiomodulation Therapy+Photodynamic Therapy
Different letters in row indicate statistically significant difference. Wilcoxon test, significance accepted at 5%.
PBM-T, photobiomodulation therapy; PDT, photodynamic therapy.
In the PBM-T group (n = 17), seven patients had no signs, symptoms, or visible lesions of OM at final follow-up. Only one patient experienced recurrence of OM after an additional chemotherapy cycle. Four patients died and six were lost to follow-up.
In the PBM-T+PDT group (n = 14), four patients had no signs, symptoms, or visible lesions of OM at final follow-up. Of these, two experienced recurrence of OM; one after an additional chemotherapy cycle and the other due to underlying Sjögren syndrome, an autoimmune disorder characterized by abnormalities of the lacrimal and salivary glands, leading to xerostomia and xerophthalmia, and may ultimately cause mucositis. Five patients died and five were lost to follow-up.
There were no treatment-emergent adverse effects to either therapy (PBM-T and PDT) in either group.
Discussion
The present study evaluated the effects of PBM-T alone and combined with PDT on OM in cancer patients. PBM-T caused a significant decrease in OM grade, in agreement with Sandoval et al., 2 Nes and Posso, 14 and Medeiros-Filho et al. 6 The current study used PBM-T in the red spectrum (660 nm), as done previously by other authors. 2,6,20,22 One of the key study findings was that combining PDT and PBM-T led to faster improvement of OM, which suggests that the disinfection of the oral cavity achieved with PDT can play an important adjuvant role in the treatment of OM. As patients with OM lesions experience difficulty feeding and are immunosuppressed, remission of acute OM lesions quickly improves the patient's ability to feed properly. The faster improvement of OM achieved by patients who receive PDT+PBM-T may have a positive influence on survival.
One of the methodological limitations of the present study was the fact that patients were not distributed randomly between the two experimental groups. This was because patients unable to rinse the oral cavity with the photosensitizer (due to gag reflex or functional limitations caused by the tumor) and intubated patients were automatically allocated to the PBM-T group, leading to a non-Gaussian sample distribution. A larger sample size might have allowed us to obtain a more homogeneous and parametric distribution of results.
PBM-T is believed to exert a biphasic effect. The first phase is immediate and occurs as a result of direct irradiation of cell components, while the second is a delayed response that occurs after hours or days. 10 Its effects are the result of activation of endogenous chromophores (cytochrome c oxidase, TRP), light absorption by intercellular water, and several mediators: growth factors (TGF-β1), pro- and anti-inflammatory cytokines, matrix metalloproteinases, and small molecules, such as ATP and reactive oxygen species. 9,10,11,29 These mediators guide cell proliferation, differentiation, angiogenesis, and immune activation, modulate apoptosis, and improve cell survival, explaining the pain relief and significant reduction in OM grade obtained by patients in our sample.
PBM-T applications in this study were performed once a week for 4 weeks and timed to coincide with patients' return for chemotherapy treatment. The literature shows a variation of 4–10 days of applications 6,14,26 or applications until remission of symptoms. 2 Sandoval et al. 2 demonstrated healing and potential pain relief through increased cell division and modification of nerve conduction through the release of neurotransmitters, endorphins, and enkephalins with the use of PBM-T. The results agreed with the study by Nes and Posso, 14 who evaluated the effect of PBM-T on pain relief by subjecting 13 patients with OM to PBM-T applications for 5 days, where the results showed pain reduction by up to 47% on day 1 in agreement with the present study, in which there was partial relief of pain soon after the first application in the majority of cases.
The healing effect of PBM-T on OM in Wistar rats was studied by Silveira et al. 12 who evaluated mitochondrial activity by surgical removal of affected tissue and histological evaluation. This study showed that tissue healing was significantly better in the group that received PBM-T irradiation. Karu 5 stated that the action of PBM-T irradiation occurs in the mitochondria of cells, due to excitation of components of the respiratory chain, increasing their metabolism and collagen synthesis, providing a healing effect, and thereby explaining our results and those of Silveira et al. 12
Curcumin is a yellow pigment isolated from saffron, 27 which is nontoxic, derived from natural sources and very common in foods of countries such as India. 24 It also has antioxidant and antibacterial properties. 24,27 Curcumin absorbs light in the blue spectrum (468 nm, which was also used in the present study). 18
PDT can be used with curcumin as a photosensitizer and a blue light source of adequate wavelength, as in the present study. Energy transfer from the irradiated photosensitizer generates highly reactive molecules, such as singlet oxygen and superoxide anions, as well as by-products of these compounds such as peroxides and hydroxyl radicals. These substances are harmful to microbial pathogens and thus potentiate the disinfection process. 15,17,20,21,29 Najafi et al. 27 noted that PDT with curcumin is effective against periodontal diseases. In the present study, we found that there was a significant reduction in OM grade after PDT, using curcumin as a photosensitizer. PBM-T+PDT protocol included the use of 20 mL of curcumin mouthwash for 5 min, adapted from Leite et al. 25 Blue LED irradiation was done for 5 min, using a 468 nm wavelength, close to that used by Panhoca et al. 28 with 450 nm, Leite et al. 25 with 455 nm, and Najafi et al. 27 and Mahdi et al. 32 with a maximum of 480 nm.
The mechanism of action of curcumin as a photosensitizer, according to Epstein et al. 24 and Mahdi et al., 32 involves the reduction of free surface tension between curcumin and microorganisms, consequently increasing bacterial membrane permeability and resulting in bactericidal action. This double effect guarantees a greater concentration of photosensitizer within the cells, thus allowing a more effective action of PDT with curcumin, optimizing the disinfection of the oral environment. 17,19 Leite et al. 25 and Mahdi et al. 32 observed a significant decrease in the microorganisms present in the oral cavity with 2 h of PDT using curcumin as a photosensitizer, resulting in disinfection of the oral environment. Our findings that there was a significant decrease in OM and significantly shorter OM healing time with PDT compared with PBM-T are in agreement with those of Garcez et al. 20
Andrade et al., 26 along with Najafi et al. 27 and Leite et al., 25 emphasized that PDT with curcumin, mediated by blue light, caused a significant decrease in the number of microorganisms, such as Candida albicans and Aggregatibacter actinomycetemcomitans. Leite et al. 25 found in their study that even PDT alone showed a broad antimicrobial spectrum, was nontoxic to host tissues, and could reach sites in the oral cavity that are often inaccessible with other methods, besides having a low cost compared with its efficacy. Combination with curcumin allowed the potentiation of PDT, without great additional costs.
Medeiros-Filho et al. 6 evaluated the action of PBM-T combined with PDT in the treatment of OM in young patients and found that the action of PBM-T (660 nm, 4 J and 100 mW), using 0.005% methylene blue as photosensitizer in the oral cavity for 5 min before PDT, was greater compared with PBM-T alone, in agreement with the results of the present study. These authors observed a greater decrease in the diameter of OM lesions and OM grade in the PDT+PBM-T group. Medeiros-Filho et al. 6 obtained similar results as Leite et al., 25 finding that PDT was effective when all its components were used together, that is, the photosensitizer, PBM-T, and light source, optimizing the use of PDT mainly to reduce bacterial strains.
Both PBM-T and PDT combined with PBM-T were shown to be effective in the treatment of OM, benefiting patients with substantial pain relief and less difficulty in swallowing, which is often left untreated, resulting in discontinuation of radiotherapy and/or chemotherapy. PDT with PBM-T resulted in a decrease in OM healing time by ∼5 days when compared with PBM-T alone. However, extremely debilitated patients and those with limited mouth opening may not be candidates for PBM-T, considering the need for irradiation of a large number of points in the oral cavity and the need to rinse the oral cavity with the photosensitizing agent.
From a clinical standpoint, PDT with PBM-T helps speed recovery from OM lesions and may thus play an important role in improving the survival of patients with cancer. Further studies with larger sample sizes and designed to evaluate the influence of combined PDT with PBM-T are warranted, and should provide additional evidence on the importance of rapid remission of OM lesions, to support the recovery of patients undergoing anticancer therapy.
Conclusions
Within the parameters of this study, it can be concluded that PBM-T and PDT can be used for the treatment of OM, and that PDT has the potential to accelerate healing of OM lesions.
Footnotes
Author Disclosure Statement
No competing financial interests exist.