
Abstract
Objective:
Evaluate the bond strength of repairs made on composite resin following the treatment of the surface of the flaw with different bonding agents and/or CO2 laser.
Background:
The influence of CO2 laser and its interaction with other bonding agents on the surface of the flaw is not yet known. In this study, CO2 laser was chosen to treat the surface of the flaw due to its capacity to promote irregularities on the surface that enhance mechanical micro-retention.
Methods:
A block was created with Vitra APS nanohybrid composite resin (color: A3; FGM, Joinville, Brazil) measuring 5 mm in width, length, and depth (volume: 125 mm3). The surface of the flaw was treated before the repair with an adhesive, silane bonding agent, and/or CO2 laser. Six specimens were created in composite resin for each group (total: n = 36): G1: resin+resin; G2: adhesive+resin; G3: laser+adhesive; G4: laser+silane+adhesive; G5: silane+adhesive; G6: laser+silane. After the repair, the surfaces of the fracture of all specimens, which were submitted to the microtraction test, were analyzed under an optical microscope. Bond strength values obtained according to the type of surface treatment were tabulated and submitted to the Kruskal–Wallis test. Dunn's test was used to compare means.
Results:
G3 and G4 had significantly higher bond strength values compared to all other groups tested. Adhesive fractures predominated in all groups. However, G3 and G4 had a higher percentage of cohesive fractures compared to the other groups.
Conclusions:
The application of CO2 laser as a surface treatment led to greater bond strength of composite resin repairs in comparison with the groups that only received treatment with a burr and silanization. The groups submitted to CO2 laser also had a significantly lower number of adhesive failures when submitted to the microtraction test.
Introduction
The use of composite resins on teeth is indicated due to the advances achieved in adhesive dentistry since the advent of acid etching of the enamel in the 1950s 1 and the introduction of composite resins in the dental setting in the 1960s. 2 When combined with bonding systems, photoactivated composite resins enable minimally invasive restorations. The possibility of bonding the polymeric restoration material to dental tissue avoids the need to create extensive cavities or additional retentions that cause the wear of sound tissues to secure the restoration material. Moreover, bonding to dental tissues reinforces the remaining dental structure, enabling the distribution of axial tension throughout the entire tooth in the occurrence of masticatory forces. 3 Adhesive restorations function as if the remaining tooth and resin were a single substrate, dissipating the force generated by mastication and preserving both the tooth structure and integrity of the restoration.
Despite the advantages, composite resins tend to degrade over time, which diminishes the longevity of the restoration. The main problems detected are wear, discoloration, microinfiltration, and fracture of the restoration. When marginal pigmentation is detected, it is likely that marginal microinfiltration has occurred due to the degradation of the adhesive interface. In this situation, the restoration must be replaced. However, in the occurrence of mechanical wear or a resin fracture without compromising the adhesive layer, a question arises regarding the most adequate conduct on the part of the dentist: should the restoration be replaced or is it possible to perform a repair? 4
Some researchers have demonstrated that it is possible to repair a composite resin failure. 5,6 Failures occur due to the influence of diverse factors, such as location, dimension or the distribution of masticatory forces. However, repair is only possible if the marginal integrity is maintained. 7
A repair entails the replacement of the compromised region of the composite resin restoration with the insertion of further composite resin. The new portion is placed in close contact with the photopolymerized resin that already composes the restoration, with the maintenance of the entire extension of the restoration not compromised by the flaw. The advantage of a repair is the preservation of the healthy tooth structure, since this procedure enables avoiding the complete replacement of the restoration. Whenever a dentist decides to completely replace the restoration, there will inevitably be wear on the sound enamel and dentin during the removal of the composite resin adhered to these dental tissues. Therefore, the repair of composite resin restorations is in line with the principles of minimal intervention that currently guide dental practices.
Studies demonstrate that it is possible to obtain satisfactory bond strength when the repair is performed following standard bonding principles. 5 –7 For such, the bonding of a new resin layer to the existing restoration is performed after cleaning the surface exposed by the flaw with the use of phosphoric acid, followed by the application of one or two layers of the resinous component of a particular bonding system. However, the influence of CO2 laser and its interaction with other bonding agents on the surface of the flaw is not yet known. In this study, CO2 laser was chosen to treat the surface of the flaw due to its capacity to promote irregularities on the surface that enhance mechanical micro-retention.
Thus, the aim of this study was to evaluate the bond strength of repairs made on composite resin following the treatment of the surface of the flaw with different bonding agents and/or CO2 laser.
Materials and Methods
Preparation of standard block
A block was created with Vitra APS nanohybrid composite resin (color: A3; FGM, Joinville, Brazil) measuring 5 mm in width, length, and depth (volume: 125 mm3). The measurements were confirmed with digital calipers (Vonder, Curitiba, Brazil). A matrix made in condensation silicone (Zetalabor; Zhermack, Badia Polesine, Rovigo, Italy) was used to guide the making of the specimen using a mold of the block. Increments of up to 2 mm of composite resin (Vitra APS; FGM) were inserted into the matrix with the aid of a 26–30 burnisher (Cosmedent, Chicago). Each increment was individually photoactivated for 30 sec using an light-emitting diode (LED) device (Valo Cordless; Ultradent, South Jordan) with a maximum radiance of 1200 mW/cm2.
Treatment of flaw surface
The surface of the flaw was treated before the repair with an adhesive, silane bonding agent and/or CO2 laser. The different combinations of surface treatment agents are displayed in Table 1.
Experimental Groups
Six specimens were created in composite resin for each group (total: n = 36) and stored in a transparent flask (Eppendorf, São Paulo, Brazil) containing distilled water for 7 days at 37°C. After the storage period, the surface of the flaw of all specimens was scuffed using a diamond tip (#4138; KG Sorensen, Cotia, Brazil) coupled to a counter-angle handpiece (T2 Revo; Sirona, Austria) with pendular movements for 20 sec by the same operator. The counter-angle handpiece was coupled to an adapted suspension scale with a pressure of 300 g to standardize the scuffing.
Phosphoric acid (Ultra-Etch 35%; Ultradent) was applied using the aid of an applicator brush (Vigodent, Rio de Janeiro, Brazil) for 60 sec over the entire scuffed area. The acid gel was then removed with abundant water and dried with compressed air at a mild pressure. Next, 70% alcohol was applied on the entire prepared area with an applicator brush for 15 sec and dried with compressed air for the decontamination of the surface. The procedures for the treatment of the flaw surface were then performed according to the experimental group.
The silane agent (Mono Bond-S; Ivoclar Vivadent, Lichtenstein) was actively applied with an applicator brush for 60 sec, followed by evaporation of the solvent with compressed air at a mild pressure. The adhesive (Ambar APS; FGM) was applied under agitation with an applicator brush for 60 sec. The solvent was removed with compressed air and photoactivation was performed with a LED device for 30 sec at high power (1200 mW/cm2).
Ultrapulsed CO2 laser at a wavelength of 10,600 nm was applied with a quadrangular manual scanner and constant air cooling to cover the entire surface of the flaw on the specimen. The focal distance from the coaxial laser diode was 75 mm. The ultrapulsed CO2 laser (λ = 10,600 nm; Ultralase 30, South Atlanta) was used in pulsed mode, peak power of 14 W, aperture diameter of 0.20 cm, power density- 1.7J/cm2, and target beam size of 0.04 cm2. The mean pulses per sample were 157.14 pulses at energy density per sample 267.14J/cm2.
Table 2 displays the dosimetric parameters used for the application of the laser.
Dosimetric Parameters Used for Laser Application
cm, centimeters; J, joules; nm, nanometers; sec, seconds; W, watts.
Repair
The repairs were made with Vitra APS nanohybrid composite resin (color: A1; FGM) in increments of a maximum of 2 mm photoactivated individually until reaching a final volume of ∼125 mm3 (equal to the volume obtained when the specimens were made with the aid of the condensation silicone guide). After the repairs, the specimens were stored in the transparent flask with distilled water for 7 days at 37°C and then submitted to testing.
Microtraction test
Each specimen was attached to an acrylic plate with a godiva stick (DFL, Rio de Janeiro, Brazil) so that standardized cuts could be performed on all specimens with a precision cutter (ISOMET 1000; Buehler, Lake Bluff). The distance between cuts was standardized as 1.2 mm. Cuts were made in both directions, forming slivers measuring 1.0 cm in length and ∼1.0 mm2 in area.
The slivers were stored in a transparent flask with distilled water for 24 h at 37°C. Seven slivers from each specimen were selected for the microtraction test in a universal testing machine (Instron 5565; Instron Corporation, Canton, MA) at a velocity of 1 mm/min until fracture. Maximum tension values were determined based on the ratio between the load recorded at the time of fracture (given in Newtons [N]) and the area of the specimen (mm2). The cross-sectional area of each specimen was measured after the test with the aid of digital calipers. The data were tabulated and converted to MPa. There were pretest flaws in all groups tested.
Analysis of fracture pattern
The surfaces of the facture of all specimens submitted to the microtraction test were analyzed under an optical microscope (Focus–Z10; Talmax, Curitiba, Brazil) at a magnification of 10 × and classified as follows: adhesive failure: when the rupture occurred in the adhesive layer, wholly separating the two resins. cohesive resin failure: when the rupture occurred only in the composite resin (either that used in the surface treatment and that used as the repair).
Statistical analysis
For the statistical tests, the standard block was considered a specimen. Thus, each set of “slivers” obtained from the standard block enabled the determination of the mean resistance to microtraction of the corresponding specimen. Bond strength values obtained according to the type of surface treatment were tabulated and submitted to the Kruskal–Wallis test. Dunn's test was used to compare means. The SigmaPlot 11.0 program was used for the statistical tests.
Results
Bond strength
The graph in Fig. 1 shows the mean and standard deviation values for bond strength between the flaw surface of the A3 composite resin and repair in A1 composite resin in the different surface treatment groups.
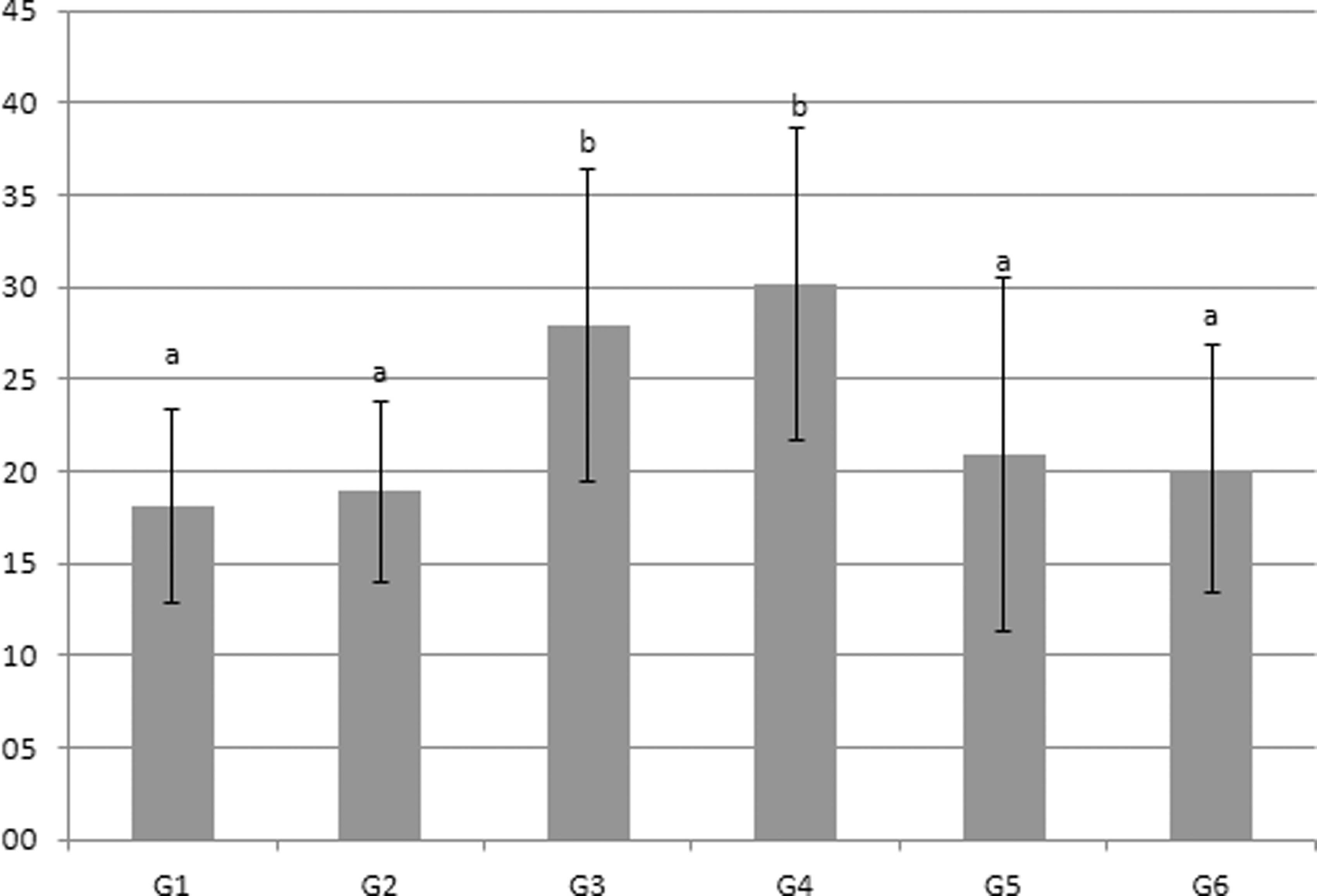
Bond strength (in Mpa) in microtraction test of composite resin repair according to surface treatment. a and b mean statistical differences and similarities. The same letters mean similar values and different letters (a × b) indicate statistically different values.
The analysis of the results revealed that G3 (laser+adhesive) and G4 (laser+silane+adhesive) had significantly higher bond strength values compared to all other groups tested (p < 0.001). In contrast, no significant differences were found among G1 (resin+resin), G2 (resin+adhesive), G5 (silane+adhesive), and G6 (laser+silane).
The specimens that failed before the microtraction test were not considered in the calculation of mean bond strength in the different groups. However, the failures corresponded with the bond strength results. Among a total of 18 failures before the test, 5 occurred in G1, 3 occurred in G5, and 5 occurred in G6. Two failures occurred in G2 and G3, each, and only 1 pretest failure occurred in G4.
Fracture pattern
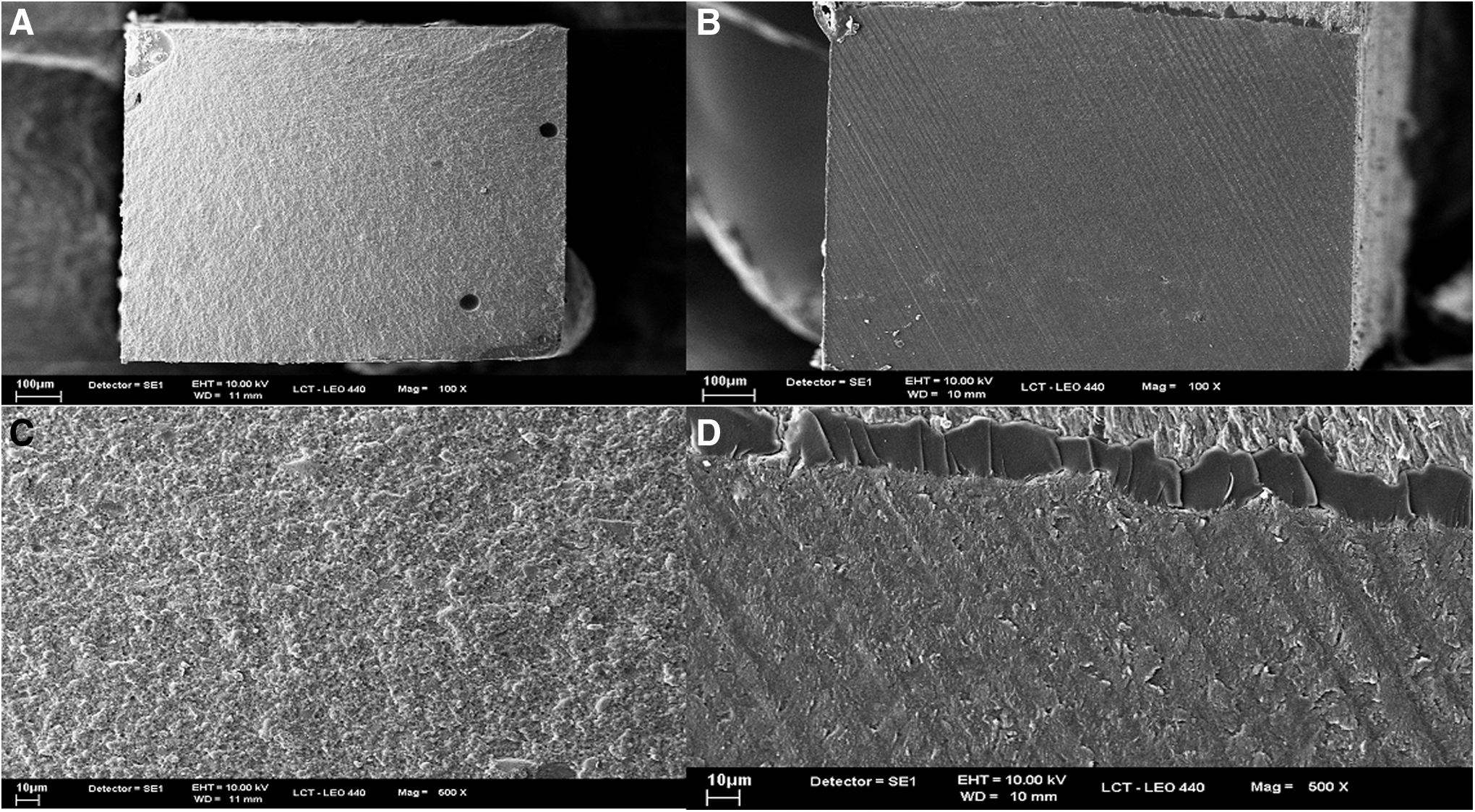
The graph in Fig. 2 displays the type of fractures having occurred after the submission of the specimens in each experimental group to the microtraction test. Figure 3 shows the fracture pattern analyzed by scanning electron microscopy.
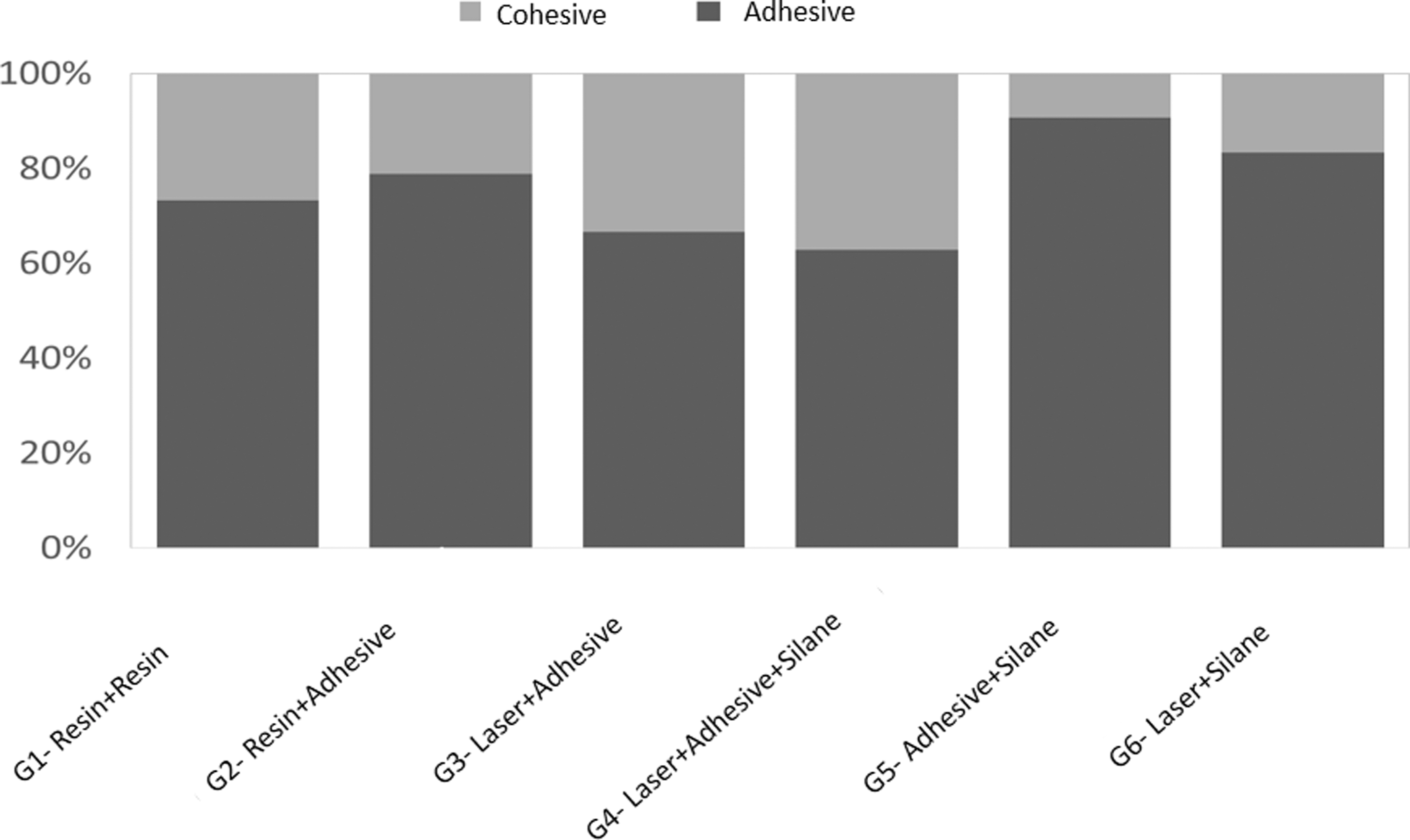
Fracture pattern after rupture of specimens according to surface treatment.
Adhesive fractures predominated in all groups. However, G3 and G4 had a higher percentage of cohesive fractures compared with the other groups.
Discussion
The repair procedure for composite resin restorations is an important part of clinical practice for dentists, as it enables “touching up” a restoration with a flaw without necessarily having to completely replace it, thereby preserving sound dental tissues. 8 –10 However, it is of extreme importance to demonstrate the bond efficiency of the repair, since, if the repair fails, all efforts to preserve the sound enamel and dentin will have been to no avail.
The repair procedure involves the use of phosphoric acid on the surface of the flaw in the restoration to remove possible impurities. Next, the flaw surface is washed and dried, followed by the application of one or two layers of the resinous component of the selected adhesive system (primer and bond). After photopolymerization of the adhesive, the missing part of the restoration is reconstructed. This standard technique was used in G2 in this study, which exhibited a similar bond strength to that found in G1, in which only a new resin layer was placed over the flaw surface of the existing restoration.
If the surface of the flaw was not in contact with the oxygen from the air before the fracture, one may suppose that there is an absence of nonreacted free monomers on this surface capable of establishing chemical bonds with the recently inserted monomers of the repair resin (G1 and G2). Therefore, the bond strength of the repair resin could be low, thereby hindering the repair. Despite this, the repairs made with only the addition of composite resin (G1) and those made with the adhesive system (G2) has statistically similar bond strength values, demonstrating that the repair resin somehow establishes chemical bonds with the surface of the flaw with or without the use of an adhesive system. However, G1 and G2 had lower bond strength values than the groups in which the flaw surface was treated with CO2 laser before the application of the adhesive.
The highest bond strength values during the microtensile tests were found in G3 and G4. In these groups, the use of laser before the application of the adhesive system was the preponderant factor for this increase in the bond strength of the repairs. When interacting with the surface of resin, the CO2 laser beam is absorbed by the resin composites components generating a sudden rise in temperature that vaporizes the resin and creates porosity, 11 and likely enables the greater permeation of the resinous components of the adhesive system. Polymers combine a low heat capacity with a low heat conductance, which means that any absorbed heat will result in a rapidly rising temperature. 12 Some studies indicate that laser is capable of increasing the number of micro-retentions, increasing the surface energy, and favoring the wetting of the resinous component of the adhesive system, just like aluminum oxide blasting proposed in other studies. 13,14
It should be pointed out that during the application of laser to the surface of the flaw in the existing restoration, it was necessary to hydrate the composite resin with jets of water to decrease the temperature at the target and to avoid the alteration of its physical properties.
CO2 laser had been shown to be successful at enhancing the bond interface between brackets and ceramics. This is attributed to the complete absorption of the wavelength of the CO2 laser on the surface of the glaze, 15 which can be reproduced on the surface of a composite resin to promote micro-mechanical retentions. 16 Türkmen et al. 17 report that the application of Nd:YAG laser on the surface of composite resin results in the formation of cracks, micro-pits, and porosities. Chan et al. 18 report that the use of CO2 laser promotes the selective ablation of the composite resin. Ahmadizenouz et al. 19 reported that the use of Er: YAG laser promoted bond strength similar to the use of blasting and the use of drills in nanoparticulate composites. However, Etemadi et al. 20 reported that proper use of potency is critical because of excessive material deterioration but potencies below 5 W produced a retentive surface that can interact with composite resin.
The irradiation of the laser applied after the use of diamond tip as it occurs when blasting with an abrasive substance produces micro and macro-mechanical retentions that favor the imbrication of the resin of repair.
Like what occurs when blasting with an abrasive substance, laser irradiation applied after the use of a diamond tip in the region of a restoration in which a fracture or chipping has occurred produces micro and macro-mechanical retentions that favor the imbrication of the repair resin. This hypothesis seems to hold true, as the resinous component of the Ambar adhesive system (FGM) was used after irradiation in G3 and G4. In G4, the flaw surface also received a layer of the silane bonding agent after the adhesive, but the bond strength values were statistically similar to those in G3. Therefore, silane appears not to have played an important role in the bond between the repair resin and flaw surface of the restoration. This phenomenon has also been reported in previous studies. 20
A possible explanation for the negative interference of the silane agent on bond strength resides in its chemical nature. As silane is made up of a bi-functional molecule, it establishes chemical bonds with organic molecules through one of its functional groups and also establishes chemical bonds with inorganic groups. In the repair of composite resin components, however, there are no inorganic molecules available to establish a chemical bond with silane, which makes its presence diminish the interaction between the resin of the flaw surface and the repair resin.
The bond strength data in G3 and G4 are confirmed by the analysis of the fracture pattern in the specimens submitted to traction force. Although the predominant pattern in all groups was adhesive failure, a greater frequency of cohesive failures (either of the repair resin or the resin of the flaw surface) occurred in the groups in which CO2 laser and adhesive were used, confirming the greater strength of the adhesive interface in G3 and G4.
The bond strength values in G5 and G6 were similar to those found in G1 and G2. In G5, the use of silane once again was unable to exert a positive influence on the bond strength of the restoration/repair interface. In G6, although CO2 was used as in G3 and G4, the adhesive was not used, having been replaced with the silane agent. Therefore, although the laser increased the roughness of the flaw surface, the silane agent once again appears not to have been able to establish all chemical bonds necessary to increase the bond strength of the adhesive interface. When ceramic materials are involved in the adhesive interface, the silane agent is able to establish chemical bonds with the inorganic molecules that compose ceramic glass and thus increase bond strength. 20 –23 Although the literature has reported good clinical results for more than 10 years with the use of composite resin repair methods, 24,25 there is no consensus on which is better in the long term or which is more reliable among the new generation of materials, such as the use of functional monomers in adhesive systems and resins that enable the control of polymerization tensions.
Based on the present findings, the use of CO2 laser combined with a universal bonding agent increases the bond strength in repairs of composite resins with charged nanoparticles.
Conclusions
In this study, the application of CO2 laser as surface treatment led to greater bond strength of composite resin repairs in comparison with the groups that only received treatment with a burr and silanization. The groups submitted to CO2 laser also had a significantly lower number of adhesive failures when submitted to the microtraction test.
Footnotes
Author Disclosure Statement
No competing financial interests exist.