
Abstract
Objective:
We evaluated the effects of photobiomodulation (PBM), mandibular advancement (MA), and the combination of both treatments (PBM+MA) on condylar growth, by the analysis of cartilage and bone formation, fibrillar collagen deposition, proteoglycan content, cell proliferation, and clastic cell index (CCI).
Methods:
Forty male Wistar rats were randomly assigned to CONTROL, PBM, positive control-MA, and PBM+MA groups. The appliance was worn 10 h/day. Laser was irradiated bilaterally on mandibular condyles in 8 alternate days (1 irradiation point per condyle) using the following parameters: 780 nm, 10 J/cm2, 40 mW, 1 W/cm2, 10 sec/point, 0.4 J/point, and cumulative dose per point: 3.2 J. PBM+MA received both treatments simultaneously. After 15 days, the animals were euthanized and the condyles dissected and embedded in paraffin. Histological sections from the intermediate portion of the condyle were used for morphometric analysis. The relative frequency (%) of fibrillar collagens was determined in sections stained with picrosirius red-hematoxylin under polarized light or Gömöri's method for reticular fibers. Proteoglycan content was evaluated by computerized photocolorimetric analysis. CCI was determined by tartrate-resistant acid phosphatase (TRAP), and proliferating cell nuclear antigen (PCNA) was detected by immunohistochemistry.
Results:
PBM and MA influenced condylar cartilage thickeness and matrix deposition, but none of the treatments affected significantly the area of the condyle. CCI were not influenced by the treatments, but clastic cells distribution was influenced by MA and PBM+MA treatments. There was no significant difference in proliferating cells among the groups.
Conclusions:
This study demonstrated that PBM and MA stimulates matrix deposition and cartilage thickening in the mandibular condyle, but was not able to demonstrate a synergistic effect between the treatments. Additional studies should be conducted to evaluate the possible synergistic effect between PBM and MA.
Introduction
Growth discrepancies between the maxilla and the mandible characterize most of the malocclusions and can cause overload in the temporomandibular joint (TMJ) and disturbances in the physiology of the stomatognathic system. 1 In growing patients, functional devices for mandibular advancement (MA) are used in the management of class II malocclusion and have shown to effectively reduce growth discrepancies between the maxilla and mandible. 2 These devices transfer tensions to the mandibular condyle, modulating cartilage growth and bone formation. 3 The effects are increased cell proliferation, 4 growth factor expression, and matrix deposition, 5 –7 besides apoptosis regulation. 8
The mandibular condyle is the main growth center of the mandible and is lined by a secondary cartilage. Its superior layers comprise the fibrous layer, which is composed of a rich collagen I matrix and of an undifferentiated layer, whose cells can differentiate into cartilage or bone, depending on the nature of the stimulus affecting the tissue. 9 Following the undifferentiated layer, there are the chondroblast layer, the chondrocyte layer, the hypertrophic layer, and the degenerative layer. 6 In this study, we refer to the last four layers as maturation zone.
The possibility of modulating condylar growth is the key to achieve efficient approaches for the treatment of malocclusion. The combination of features capable of potentiating the known effects of functional devices or shortening the period of treatment is desirable, and studies involving photobiological stimuli have yielded promising results. 10,11
Photobiomodulation (PBM) has been used in dentistry for the past 30 decades due to its analgesic, anti-inflammatory, and biostimulatory effects. 12 –14 Many studies on the treatment of oral disorders such as herpes labialis, mucositis, stomatitis, and temporomandibular disorders have indicated these positive properties of PBM. 15 –18 The effects of PBM on the tissues are based on its interaction with the mitochondrial membranes, stimulating energy production. 19 In the joint cartilage, PBM enhances the stiffness of the repairing tissue, 20 and increases extracellular matrix volume 21 and the production of glycosaminoglycans and collagen II. 22
This study tested the hypothesis that PBM could improve MA effects on cartilage and bone tissues of the mandibular condyle.
Materials and Methods
Animals and experimental protocol
All experiments were conducted in accordance with the guidelines of the Committee on Animal Experimentation of the Federal University of Goiás (CEUA/UFG 154/2009). Forty 30-day-old (juvenile phase) male Wistar rats were provided by the UFG's central animal facility and maintained in the vivarium of the Laboratory of Morphology at 22°C in a 12 h/12 h light/dark cycle. Animals received water and food ad libitum (Labina-Purina®) during the adaptation period, but during the experimental period, animals received food only in the dark period to prevent the removal of the mandibular appliance. The animals were randomly assigned to four groups (n = 10/group): intact control, PBM, positive control-MA, and PBM and MA combined (PBM+MA), the lattern of which was patented by the Federal University of Goiás (BR102016018828-8). MA was performed by a propulsive appliance designed as described by Hajjar et al. 6 The appliance was used from 8:00 a.m. to 6:00 p.m., totaling 10 h daily in both positive control-MA and PBM+MA groups (Fig. 1A). In brief, the appliance consists of a copper plate fixed in the upper incisors of the animals. It creates an inclined plane, in which the mandible is displaced anteriorly every time the animal closes its mouth, following the principles of functional orthopedics. The animals wore a soft leather collar to prevent the removal of the appliances (Fig. 1B, C).
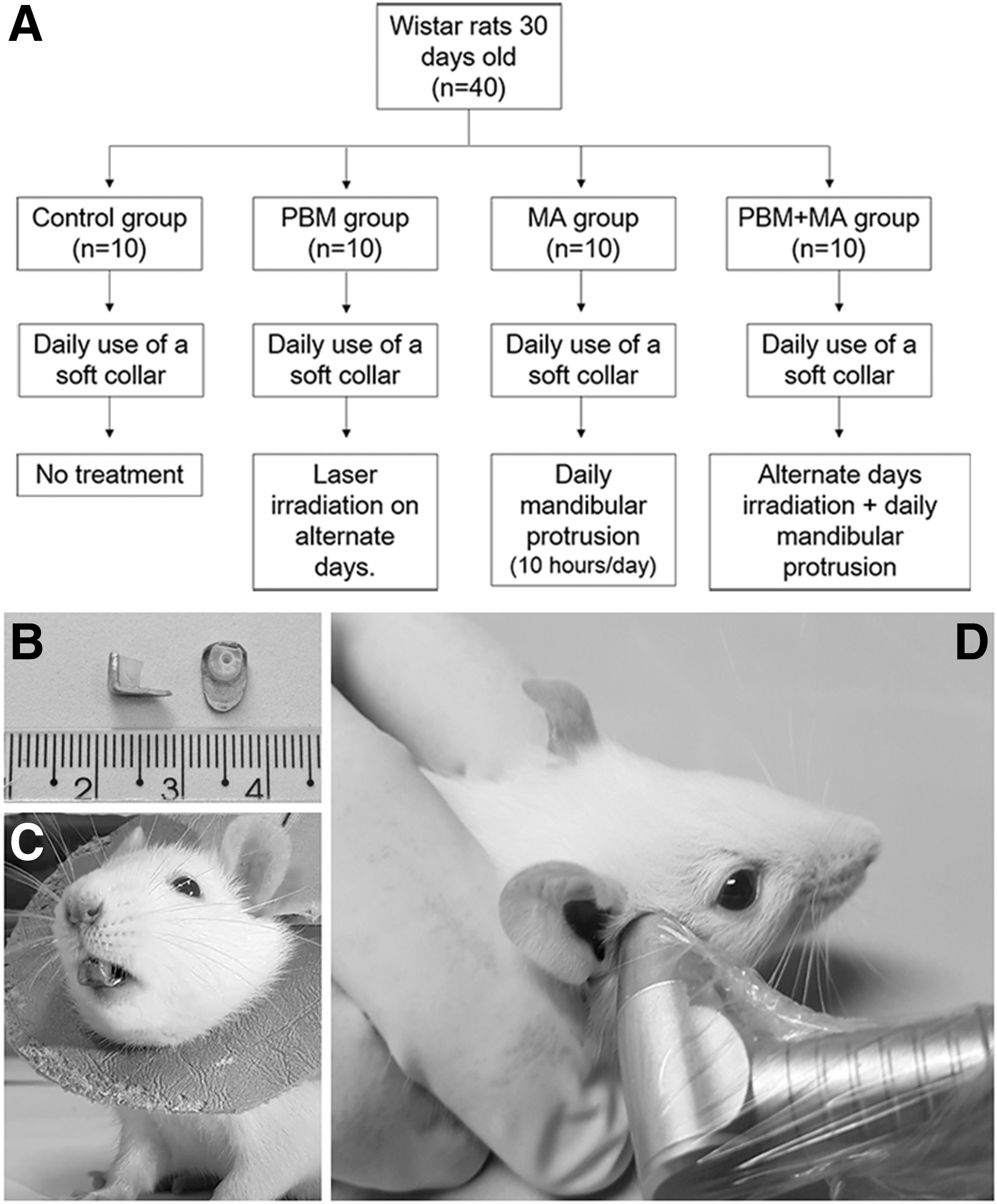
Experimental design.
Photobiomodulation
A continuous-wave laser diode (InGaAlP; Twin Laser; MM Optics®, São Carlos, Brazil) was used. A power meter (Laser Check; MM Optics, São Carlos, Brazil) was used to determine the laser output power before each irradiation. The parameters used are based on previous studies 28 and were as the following: wavelength: 780 nm; power output: 40 mW; spot size: 0.04 cm2; power density: 1 W/cm2; energy density: 10 J/cm2; one point of irradiation for each TMJ; energy/point: 0.4 J; and duration of irradiation: 10 sec/point. As laser applications were performed for 8 alternate days, then the total accumulated energy per point was 3.2 J (Table 1). Irradiation was applied to one point covering the TMJ region, bilaterally, and the laser beam was applied in contact with the skin at an angle of 90° (Fig. 1D). Irradiation was performed every other day, at 3:00 p.m. During the study, the animals were weighed every other day.
Laser Parameters
Histological processing
After 15 days of treatment, the animals were euthanized (ketamine 180 mg/kg of body weight combined with xylazine 20 mg/kg of body weight). The condyles were fixed in methacarn solution for 3 h, demineralized in 5% EDTA solution, and processed for Paraplast® embedding (Sigma Chem. Co., St Louis, MO). Serial sagittal sections (5 μm) from the intermediate portion of the condyles were used for analysis.
Morphometric analysis
The sections were stained with hematoxylin-eosin (HE) and then analyzed and photographed using a Primo Star iLed microscope (Carl Zeiss MicroImaging, Goettinger, Germany) attached to an AxioCam ERc 5s microcamera (Carl Zeiss MicroImaging, Jena, Germany). Measurements (n = 4 animals/group) were performed using Image Pro-Plus 6.0 (Media Cybernetics, Inc., Silver Spring, MD). The area per section of the cartilage, bone, and the whole section of the condyle was determined from the intermediate portion of the condyles at 100 × magnification. To determine the thickness of the layers five sections per animal were photographed at 400 × magnification. In each of them, 5 linear measurements were obtained, totaling 100 measurements for each layer per group.
Distribution and relative frequency of fibrillar collagens
Sections were stained with picrosirius red-hematoxylin and then analyzed and digitized using a Zeiss Axioscope A1 light microscope (Zeiss) with polarizing filter (n = 4 animals/group). Collagen III (reticular fibers) was detected by Gömöri's silver impregnation technique. Fifteen microscopic fields were obtained from the undifferentiated layer and also from the maturation zone (1000 × magnification) per animal, totaling 60 fields/group. The relative frequency of fibrillar collagens was obtained using Weibel's 23 multipurpose test grid with 130 points and 10 test lines. The relative value was determined by counting the coincident points in the test grid and dividing them by the total number of points using the Image-Pro Plus software v6.1 for Windows (Media Cybernetics, Inc.).
Determination of proteoglicans content
The content of proteoglycan was determined by computerized photocolorimetric analysis and the variable of interest was optical density. For that, 400-fold increased images obtained in light field microscopy were used to determine the optical density in the ImageJ software (National Institute of Health) using the pluggin Fiji. A circular macro was used to capture the optical density at 3 distinct points of each image, totaling 108 points of quantification per group. The intensity of staining was quantified on a scale between 0 and 255, with 0 being the highest density and 255 being the lowest.
Clastic cell index
The clastic cell index (CCI) per area was determined in the posterior region of the condyle using tartrate-resistant acid phosphatase (TRAP) 387 kit (Sigma-Aldrich, St Louis, MO) according to the manufacturer's instructions. Four sections of the intermediate portion of the condyle were used per animal. Two images from the subchondral zone were obtained for each region of the condyle, totaling eight images per region. Images were captured at 400 × magnification comprising an area of 5590 mm2. The number of clastic cells was counted in the subchondral zone (n = 6 animals/group and 36 fields/animal) using Image Pro-Plus 6.0 (Media Cybernetics, Inc.).
Immunohistochemistry
Tissue sections were subjected to immunohistochemistry for detection of the proliferating cell nuclear antigen (PCNA; n = 6 animals/group). The sections were deparaffinized, rehydrated through a decreasing ethanol series, and the Leica BIOSYSTEMS NovoLink Polymer Detection System Kit (RE7150-K) was used according to the manufacturer's instructions. DAB was used as chromogen.
PCNA quantification
Seventy-two microscopic fields (n = 6 animals/group; 40 × magnification) were used for PCNA quantification in each experimental group. In each field, the total number of positive cells was obtained as relative frequency (%) in relationship to the total number of cells. All the analyses were performed using the previously described image analysis system.
Statistical analysis
The proper evaluation of the existence of a synergistic effect between PBM and MA demands the evaluation of the statistical interaction of them. Otherwise, as different measurements in the same individual are not statistically independent, we include the individual as a random effect in all analysis. Thus, we apply a General Linear Mixed Model (GLMM) to the results using the package LME4 in the software R. 24 This choice favored both the use of all information collected, respect the statistical independence, and increase statistical power of the test. GLMM is known to have a higher statistical power even under small sample sizes since it can consider the repeated measurements in each individual in the analysis. 25 Values are presented as mean ± standard error of mean. Statistical data not present in the main text are available in the Supplementary Tables S1–S4.
Results
Morphometric analysis
None of the treatments increased significantly the area of the condyle, neither the cartilage nor bone areas (Fig. 2A–C). In the condylar cartilage, none of the treatments changed the fibrous layer thickness (Fig. 3A). The undifferentiated layer and the maturation zone were increased by PBM and by MA. However, there was no synergistic effect between the treatments in these layers (Fig. 3B, C).
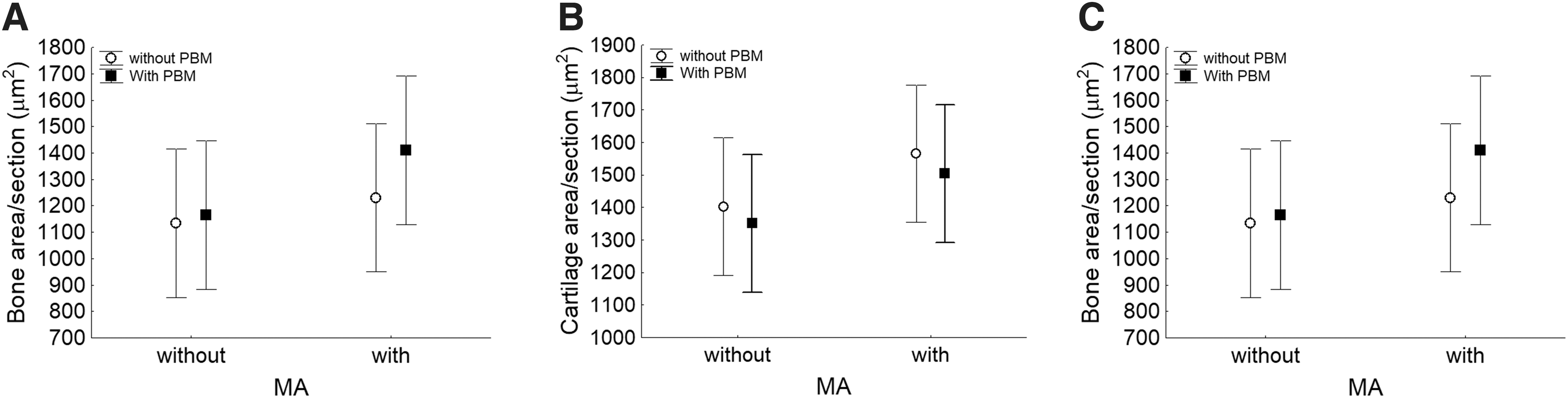
Area per section in the mandibular condyle. Area per section considering the whole condyle

Thickness of the condylar cartilage layers. Fibrous layer
Distribution and relative frequency of fibrillar collagens
In the control and PBM groups, fibrillar collagens were oriented predominantly on the long axis of the undifferentiated layer (Fig. 4 a, b). In the MA and PBM+MA groups, fibrillar collagens were clearly oriented in the posterosuperior direction; however, fibers were thicker in the PBM+MA group (Fig. 4c, ). In the maturation zone, fibrillar collagens were located around the chondrocyte lacunae and were progressively thicker in the treated groups (Fig. 4e–h). PBM decreased the percent of fibrillary collagens in the undifferentiated layer (Fig. 4i) and increased it in the maturation zone (Fig. 4j). MA increased fibrillar collagens in the undifferentiated layer (Fig. 4i) and in the maturation zone (Fig. 4j). Collagen III was present in the undifferentiated layer and its relative frequency increased in all the groups, particularly in the PBM group (Fig. 5A). There was no synergistic effect between the treatments on fibrillar collagen deposition.

Fibrillar collagens in the posterior region of the condylar cartilage. Picrosirius red staining shows fibrillar collagens in the fibrous layer and undifferentiated layers
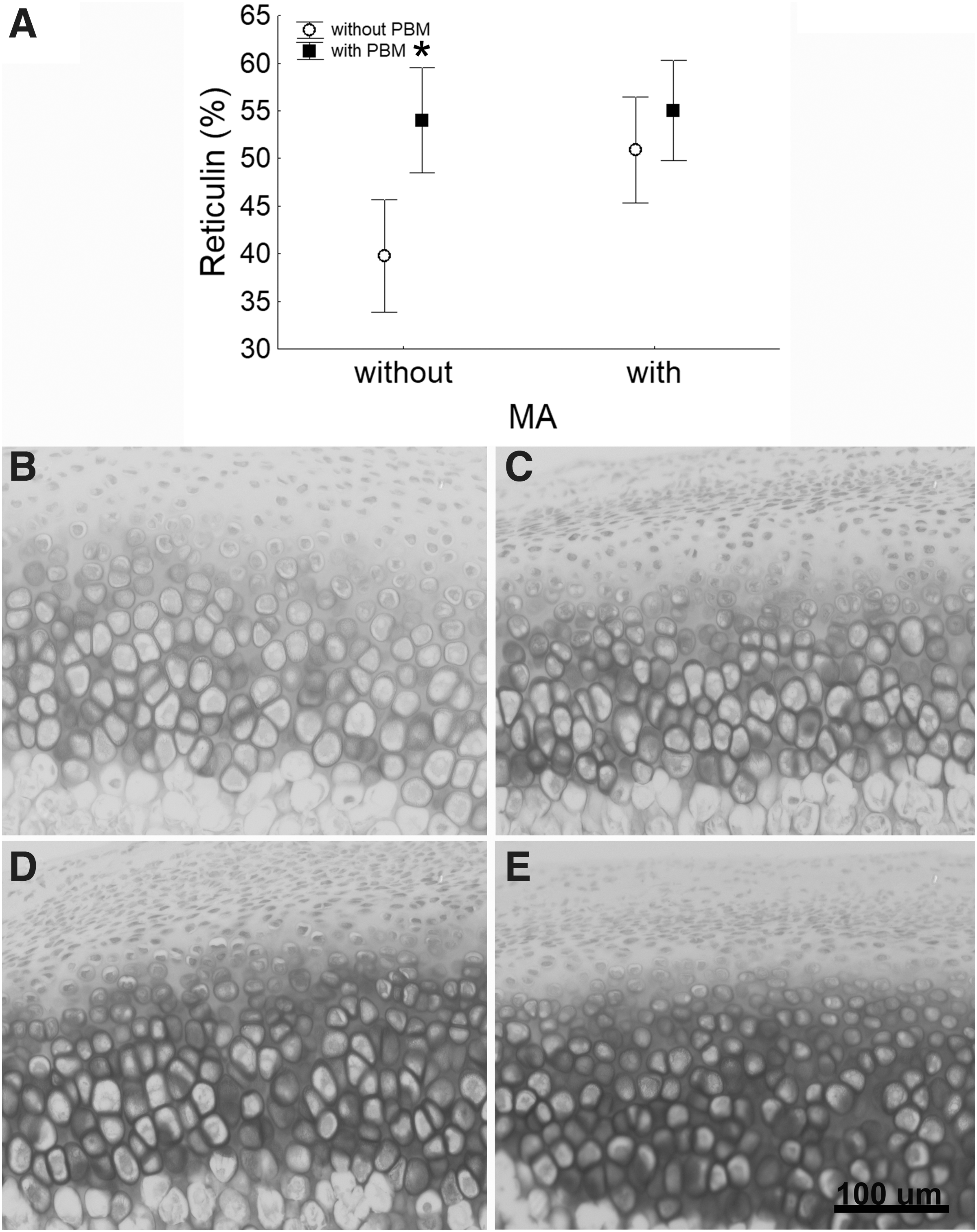
Reticulin (collagen III) and proteoglycan deposition in the condylar cartilage. Relative frequency of collagen III
Distribution and optical density of proteoglicans
Proteoglicans depositon was detected in the maturation zone. According to the scale of the Fiji pluggin of the ImageJ program, the higher the number of proteoglycans, the lower the value attributed to optical density. So, the content of proteoglycan in the CONTROL group (167.2 ± 1.4) was lower than the treated groups (PBM = 153.2 ± 1.4; positive control-MA = 144.8 ± 1.6 and PBM+MA = 141.8 ± 1.0; p ≤ 0.05). However, there was no synergistic effect between the treatments (Fig. 5B–E).
Cell proliferation
PCNA-stained cells were distributed in the chondroblast and hypertrophic layers of the condylar cartilage in all groups. The relative frequency (%) of PCNA-positive cells did not differ significantly among the groups despite the increase in PBM and positive control-MA groups (Table 2).
Proliferation and Clastic Cells Index in the Condylar Cartilage
GLMM, p < 0.05.
CCI, clastic cell index; GLMM, General Linear Mixed Model; MA, mandibular advancement; PBM, photobiomodulation; PCNA, proliferating cell nuclear antigen.
Clastic cell index
The histochemical analysis of TRAP revealed a similar pattern for TRAP-positive clastic cells in all groups. Numerous multinucleated TRAP-positive clastic cells were attached to the trabeculae in the subchondral region of the condyle, which is characteristic of active clastic cells. Cell count revealed no statistical difference among the groups (Table 2).
Discussion
This study tested the hypothesis that PBM could improve the effects of MA on condylar growth. Therefore, the effects of MA, PBM, and PBM+MA on the morphology of bone and cartilage of the mandibular condyle were assessed after 15 days of treatment. The relative frequency (%) of proliferating cells and fibrillar collagens in the cartilage was also evaluated. The CCI was determined for the subchondral zone in the anterior, central, and posterior regions of the condyle. MA was performed 10 h daily and the total laser energy applied was 3.2 J.
The treatments affected neither the area of the condyle nor the area of the cartilage or the bone, however, the effect of PBM varied in the different layers of the condylar cartilage. PBM did not affect the fibrous layer, reduced the undifferentiated layer, and increased the maturation zone, suggesting that the effects of PBM depend on the characteristics or the sensitivity of the tissue to photobiological stimuli. PBM reduced the undifferentiated layer thickness. This effect is contrary to bone growth once the more the undifferentiated cells, the more the bone formation in the mandibular condyle. 4 However, even though PBM reduced the undifferentiated layer, it increased the maturation zone thickness and matrix deposition in this layer. These results suggest an inductive effect on cell differentiation. Such stimulatory effect has been previously shown by in vitro studies on cartilage, 21 osteocytes, 26 and cardiomyocytes. 27 In other words, PBM does not seem to be able to promote condylar cartilage growth, but it prepares the tissue for bone formation, at least in the evaluated period. Fekrazad et al. 28 described similar effects on joint cartilage defects in rabbits, showing that PBM does not increase cartilage but promotes bone formation. Long-term studies could demonstrate whether PBM consolidates bone formation in the mandibular condyle.
Sinergistic effects of PBM associated to MA on bone formation have been demonstrated by morphometric 29,30 and cephalometric studies. 31,32 Our study did not show significant increase in the bone area for any of the treatments, however, PBM and MA increased cartilage thickness in the undifferentiated layer and in the maturation zone. There is a close relationship between the amount of extracellular matrix in the hypertrophic layer and the potential amount of bone formation. 20,21 All the treatments increased the maturation zone thickness, which involves the hypertrophic layer. PCNA-stained cells and fibrillar collagens also increased in the hypertrophic layer of the PBM and positive control-MA groups; however, as the increase in PCNA-stained cells was not statistically significant, we considered the increase in the maturation zone to be closely related to fibrillar collagen production. These findings are in line with the literature, showing an increase of collagen X in the hypertrophic layer after 14 days of mandibular protrusion. 22 The proteoglycan content also increased in all the treated groups, certainly contributing to the maturation zone increase.
According to Shen et al., 21 it is well established that postnatal growth of the mandibular condyle is mainly supported by endochondral ossification of the condylar cartilage. The condyle is the main growth center of the mandible; thus, modulating its bone formation is important to adjust the growth discrepancies between the maxilla and the mandible. Combining MA with PBM may offer a new possibility of treatment for class II malocclusion.
Few studies have evaluated the thickness of condylar cartilage layers. Abtahi et al. 29 using 1.8 J/point, 5.4 J/d, and 113.40 J of energy accumulated after 3 weeks of daily application compared MA and PBM+MA groups and found that condylar cartilage thickness remained unchanged between the groups and reduced the fibrous layer in the PBM+MA group. Previous studies conducted at our laboratory 30 applying 0.4 J/point, one point per condyle/day, and 3.2 J of energy accumulated after eight intercalated applications are partially at odds with these findings, showing that PBM+MA increased total cartilage thickness when compared to the MA group. 30 Now, in the present study, we suggest that the total increase in cartilage thickness could be promoted by collagen and proteoglican deposition in the maturation zone.
In the undifferentiated layer of the positive control-MA and PBM+MA groups, collagen fibers became backward-oriented, corroborating the data of Oudet et al., 31 who show that mandibular propulsion promotes condylar growth in the same direction. The combined treatment also increased the percentage of fibrillar collagens in this layer, suggesting that the effects on matrix deposition extended to the superior regions of the cartilage and could improve condylar growth. The expression of collagen III (reticular fiber) increases during connective tissue repair. 32 In the condylar cartilage, collagen III is resynthesized, together with type II collagen, during cartilage repair. 33 In this study, all the treatments increased collagen III, suggesting that as PBM as MA are able to stimulate condylar cartilage remodeling.
The widely accepeted PBM mechanism of action is the absorption of the LED/laser by the Citochrome C Oxidase enzyme of the respiratory chain in the internal mitochondrial membrane. As result, the ATP production and the cellular activity increase. 19 In the bone, PBM increases osteoblasts and osteoclasts activity, 10 osteoblasts viability, 11 and extracellular matriz gene expression 26 indicating that PBM favors bone formation. In the condylar cartilage, PBM has shown opposite effects as increased cartilage area 34 and no changes in the cartilage thickeness. 29
There are distinct protocols using different laser doses in studies involving mandibular condyle and it is well known that cells' behavior depends on irradiation conditions. 35,36 We applied 0.4 J/point and a total dose of 3.2 J in the treatment and observed a reduction in the cartilage thickness. Cephalometric studies show that 5.0 J/point 37 results in higher condylar growth compared to 0.4 J/point of our study. On the contrary, the cartilage area increases after irradiation of 6.0 J/cm2 (Total Energy applied of 7.9 J). 38 Possibly higher energy/point could have an important influence in the effect of PBM on cartilage. So, studies testing different laser parameters are important to discover the best parameter for condylar cartilage growth. Also, understanding the molecular basis that regulates condylar cartilage response to PBM could contribute to learning about the controversial behavior of the cartilage.
Clastic cells such as osteoclasts and chondroclasts resorb bone and mineralized cartilage during endochondral ossification. 39 We showed that the number of clastic cells was similar among the groups, suggesting that the treatments did not affect the recruitment of clastic cells and none of the treatments accelerated cartilage absorption.
In conclusion, isolated PBM or MA increased condylar cartilage thickness possibly by increasing collagen and proteoglycan deposition in the maturation zone. According to the parameters used in this study, we were not able to show synergistic effect between the treatments. Additional studies testing different PBM parameters should be conducted to evaluate the possible synergistic effect between PBM and MA in the mandibular condyle.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This article was supported by a grant from the Goiás Research Foundation, Procs. (FAPEG No. 05/2012).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.