
Abstract
Objective:
This study was designed to evaluate the effects of an Erbium, Chromium:Yttrium-Scandium-Gallium-Garnet (Er,Cr:YSGG) laser on removing the filling residues and smear layer (SL) after retreatment using rotary files.
Background:
Er,Cr:YSGG laser has been proposed as an additional protocol to improve root canal cleaning and removal of the filling remnants.
Methods:
Eighty-four mandibular premolars were divided into six groups (n = 14). Groups 1, 2, and 3 were obturated using a cold lateral compaction technique, and groups 4, 5, and 6 were obturated using a thermoplasticized injectable technique. The retreatment procedures were performed in all of the groups using a rotary system before applying Er,Cr:YSGG laser at 1.5 W for groups 2 and 5, and at 3.0 W for groups 3 and 6. Then, the teeth were split longitudinally into two halves and observed under a stereomicroscope and a scanning electron microscope. The SL and residual filling materials were evaluated at the coronal, middle, and apical thirds of the root canal. The data were statistically analyzed using three-way analysis of variance and Tukey tests.
Results:
The 3.0 W Er,Cr:YSGG laser was significantly more effective in removing SL than the other retreatment procedures in the coronal and middle thirds, but there was no significant difference in the apical third (p > 0.05). However, carbonization was observed in some of the specimens in the 3.0 W laser groups.
Conclusions:
None of the retreatment procedures completely removed the filling remnants from the root canal. However, the additional use of lasers improved the canal cleaning after retreatment.
Introduction
The main purpose of root canal treatment is to prevent infections by shaping, cleaning, and filling the root canal system. 1 Several obturation techniques, including cold lateral compaction (CLC), single core, and thermoplasticized injectable (C) techniques, have been introduced in an attempt to improve the hermetic filling of the root canal with apical seal. 2
Despite the fact that an endodontic treatment has a high success rate, there are some cases in which an infection reappears and the endodontic treatment fails. In these cases, the root canal system should be retreated and disinfected by completely removing the previous canal obturation materials. The retreatment success depends on many factors, such as removal of as much filling material as possible from the root canal system, elimination of failure factors in primary treatment, biomechanical preparation, and hermetic filling of the canal. 3
Traditionally, root canal retreatment has been performed using hand files and solvents. As an alternative to the conventional methods, rotary nickel-titanium (NiTi) retreatment files have been developed to remove the obturation materials and smear layer (SL) more effectively. However, many studies showed that there are significant amounts of obturation materials and SL left on the canal walls after using rotary retreatment files. 4 –7 Therefore, several techniques have been introduced as additional attempts to enhance root canal cleaning, such as the use of ultrasonic systems, heat-carrying devices, and lasers.
Several laser devices have been evaluated for improving the removal of SL, debris, and obturation materials residues, including diode, Erbium:Yttrium-Aluminum-Garnet (Er:YAG), and Neodymium-doped:Yttrium-Aluminum-Garnet (Nd:YAG) lasers. 8 –11 In addition, an Erbium, Chromium:Yttrium-Scandium-Gallium-Garnet (Er,Cr:YSGG) laser is another of these devices, and it has a 2780 nm wavelength that is delivered by using radial firing tips (RFTs) at different output powers. This laser's high affinity to hydroxyapatite and water produces a cleaner root canal surface when compared with the other laser devices. 12 –15 In addition, thermal damage to the surrounding tissues is minimal when using Er,Cr:YSGG laser in the root canal. 15 –18 However, to the best of our knowledge, there have been no attempts to demonstrate the efficacy of the Er,Cr:YSGG laser on removing filling remnants in retreatment cases.
The aim of this study was to utilize stereomicroscope and scanning electron microscope (SEM) to determine the effectiveness of Er,Cr:YSGG laser at two different output powers on removing the filling residues and SL after retreatment using ProTaper Universal rotary files in teeth filled with two different obturation techniques.
Materials and Methods
Teeth selection
After receiving ethics committee approval (protocol YDU/2018/54-517), 84 straight single-rooted extracted mandibular premolars were selected. Those teeth presenting apical curvatures (more than 5° according to Schneider classification), 19 carries, resorptions, or fillings were excluded. The selected specimens were disinfected with a 0.1% thymol solution and stored in physiological saline solution. Then, the crowns were sectioned using a diamond saw under water cooling (Isomet 1000; Buehler, Lake Bluff, IL) to standardize the root lengths (∼15 mm) for all the teeth. The glide path was determined using a #10 K-file (Dentsply Maillefer, Ballaigues, Switzerland). When the tip of the file was shown at the apex of the tooth, the rubber stop was placed at the reference point, and the working length (WL) was established at 0.5 mm shorter than this measurement. All of the initial and retreatment steps were completed by the same practitioner.
Root canal preparation
The root canal preparations were performed with a crown-down technique using ProTaper Universal NiTi rotary system (Dentsply Maillefer) following the manufacturer's instructions. The files were driven by an electric motor (X-Smart; Dentsply Maillefer) at a 16:1 gear reduction with hand-piece set at 250 rpm. The teeth were prepared using SX, S1, S2, F1, F2, and F3 rotary files, respectively, in which the final apical file was F3, by applying in-and-out motions. Irrigation was performed between the files using 5.25% NaOCl at a total of 20 mL per canal. Thereafter, 5 mL of 17% EDTA was applied for 5 min, followed by 15 mL of physiological saline as a final rinse. The root canals were dried using appropriate paper points (Dentsply Maillefer).
Root canal obturation
The samples were randomly divided into six groups (n = 14). In groups 1, 2, and 3, the root canal obturations were performed using a CLC technique with gutta-percha (Dentsply Maillefer) and AH Plus sealer (Dentsply DeTrey, Konstanz, Germany). The CLC technique was achieved using a #F3 master cone and #20 fine gutta-percha cones after coating them with the sealer. In groups 4, 5, and 6, the root canals were obturated using a (C) technique with Calamus Dual System (Dentsply-Tulsa Dental, Tulsa, OK) and AH Plus sealer. A #F3 gutta-percha cone was placed in the canal at the WL and it was cut off using the electrically heated tip, leaving 3–4 mm of the cone for apical sealing. The backfilling of thermosoftened gutta-percha was used to fill the rest of the canal following the manufacturer's instructions. All of the teeth were radiographed to ensure the root canal filling consistency and the absence of spaces in the filling mass. Thereafter, the teeth were incubated at 37°C and 100% humidity for 10 days to ensure the setting of the sealer.
Root canal retreatment
The retreatment procedures for all of the teeth were performed using ProTaper Universal retreatment (PTUR) instruments (Dentsply Maillefer) driven by an X-Smart electric motor at 3 N/cm torque and 300 rpm without using solvents. Three retreatment files were used following the manufacturer's instructions: D1 file (size 30, 0.09 taper) in the coronal third, D2 file (size 25, 0.08 taper) in the middle third, and D3 file (size 20, 0.07 taper) in the apical third of the canal, with a brushing action toward the canal walls. After reaching the WL, F1, F2, and F3 rotary files were used to enhance the cleaning and removal of the residual filling materials from the canal walls. The retreatment procedure was considered finished when the WL was reached, and no more gutta-percha or sealer could be seen on the surface of the last instrument used. A 5.25% NaOCl irrigation was used after each step at a total of 20 mL and physiological saline as a final irrigant. Then, the additional laser irradiation applications were performed as follows (Table 1):
Erbium, Chromium:Yttrium-Scandium-Gallium-Garnet Laser Parameters
RFT, radial firing tip.
Group 1 (CLC+PTUR)
The samples were retreated using only PTUR.
Group 2 (CLC+PTUR +1.5 W)
Er,Cr:YSGG laser (Waterlase MD; Biolase, Irvine, CA), which emitted a wavelength of 2780 nm, was used to irradiate the root canals. After setting the laser device to the hard tissues mode, the following parameters were used: pulse duration of 140 μsec, repetition rate of 20 Hz, output power of 1.5 W, and energy pulse of 75 mJ. The air and water were set at a level of 20% as recommended by the manufacturer to prevent overheating of dentine tissues. After laser activation, an RFT2 fiber tip (275 μm diameter and 21 mm length; Endolase; Biolase Technology, San Clemente, CA) was positioned in the canal at a point 0.5 mm shorter than WL, and it was pulled out from the apex back to the orifice in consecutive cycles for 15 sec at a constant speed of ∼1 mm/sec. This procedure was repeated 4 times for a total of 1 min of laser activation in each canal. The root canals were irrigated using 5 mL of 5.25% NaOCl for 2 min after the laser application, followed by 15 mL of physiological saline for the final irrigation.
Group 3 (CLC+PTUR+3.0 W)
The root canals were irradiated using Er,Cr:YSGG laser at output power of 3.0 W and energy pulse of 150 mJ, and the other parameters were the same as those in group 2.
Group 4 (C+PTUR)
The root canals retreated using only PTUR.
Group 5 (C+PTUR+1.5 W)
The teeth were irradiated using Er,Cr:YSGG laser with the same parameters that were used in group 2 (output power of 1.5 W).
Group 6 (C+PTUR+3.0 W)
The canals were irradiated using Er,Cr:YSGG laser with the same parameters that were used in group 3 (output power of 3.0 W).
Finally, all of the root canals in all the groups were dried properly with paper points for 30 sec.
Stereomicroscope and SEM evaluations
After retreatment and laser applications, the teeth were grooved longitudinally on both buccal and lingual surfaces without touching the internal walls of the canals, and they were split into two halves with a chisel. The halves were then dehydrated using ethyl alcohol (25%, 50%, 75%, and 100% for 10 min each) and dried in a desiccator for 24 h. The specimens were evaluated under stereomicroscope (S8 APO; Leica, Wetzlar, Germany) at 18 × magnification to evaluate carbonization areas on the canal walls. Before taking SEM images, the specimens were mounted on metallic stubs and coated with a gold-palladium layer. Then, the specimens were examined using SEM (EVO 40; Zeiss, Oberkochen, Germany) at 2000 × magnification at the centers of coronal, middle, and apical thirds of the root canal. According to Hulsmann et al.,
20
a 5-score system was used to evaluate the SL as follows: Score 1: An absence of SL with all of the dentin tubules being open. Score 2: A slight SL amount with some dentin tubules being open. Score 3: The canal wall covered by a homogenous SL with only a few dentin tubules being open. Score 4: The canal wall covered completely by a homogenous SL with no open dentin tubules. Score 5: A nonhomogeneous and thick SL covered the entire root canal wall with no open dentin tubules.
All images were independently evaluated and scored by two observers three times at 10-day intervals under the same conditions without knowledge of the experimental groups, the other observer's evaluations, or the previous results.
Statistical analysis
Kappa test was used to measure the interexaminer and intraexaminer repeatability during the separate time periods with values of >0.8 for each category. Then, IBM SPSS Statistics for Windows (version 22.0; IBM Corp., Armonk, NY) was used for the statistical data analyses. The mean ± standard deviation (SD) values were calculated and subjected to an analysis of variance (ANOVA) with three variables (filling technique, retreatment procedure, and root third) followed by post hoc Tukey test for the multiple comparisons when significance was detected. For all analyses, p-values of <0.05 were accepted as statistically significant.
Results
According to three-way ANOVA, the SL score values were not affected by the obturation technique or their interactions (p > 0.05) (Table 2). The mean and SD score values of SL for the test groups are summarized with Tukey post hoc comparison results in Table 3. Except for the apical third of the root, 3.0 W output laser significantly removed the SL and filling remnants more effectively than 1.5 W output laser and PTUR for both filling techniques (p < 0.05). In the apical third, all retreatment procedures showed equal effects in removing SL (p > 0.05). When the different root thirds were compared, regardless of the retreatment procedure, the coronal and middle thirds were cleaner than the apical third for both filling techniques. Figure 1 shows the representative SEM views of the coronal, middle, and apical thirds of the root canal walls in all experimental groups.
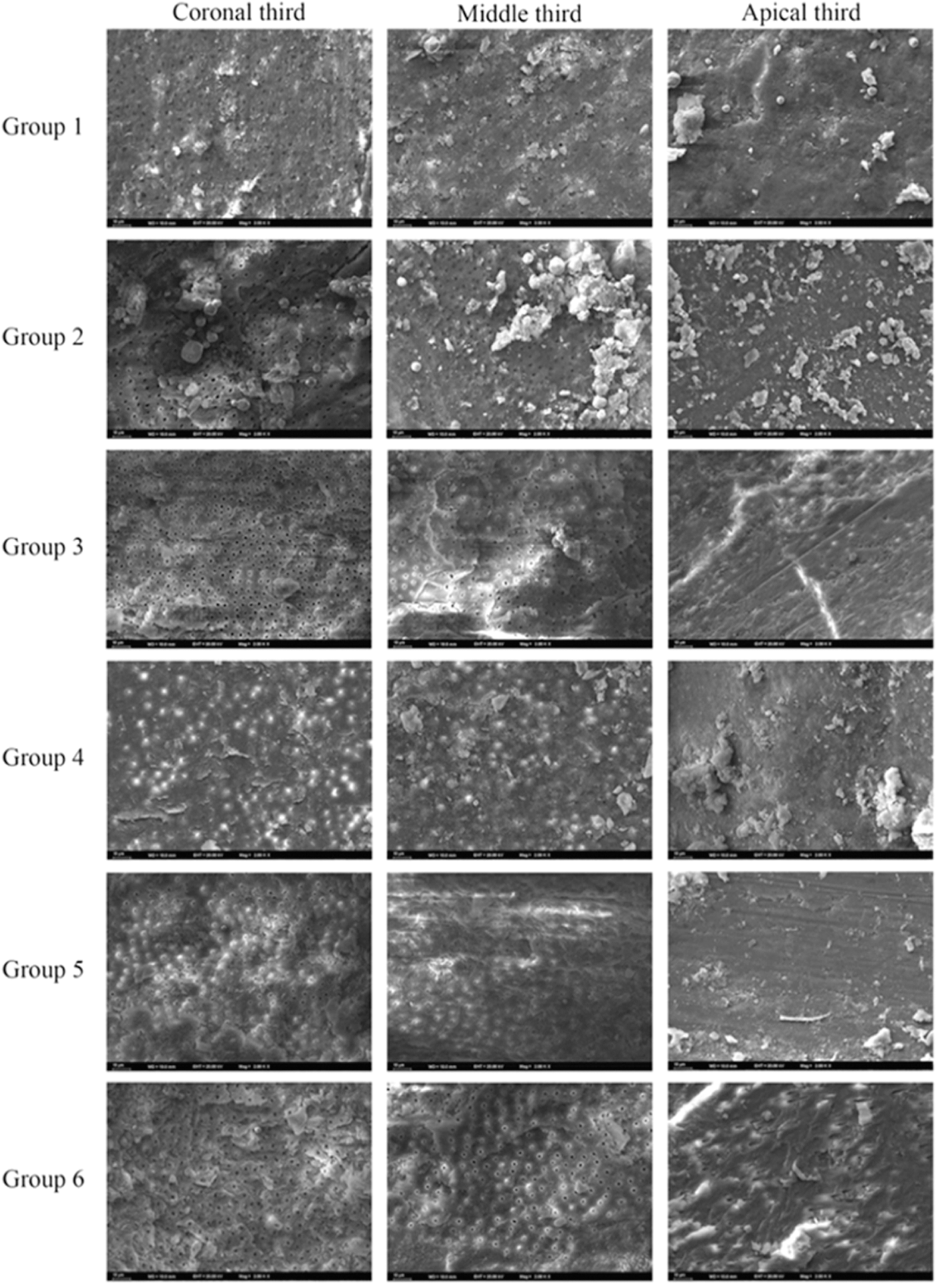
Representative SEM images of coronal, middle, and apical thirds of the root canal walls in all experimental groups. SEM, scanning electron microscope.
Three-Way Analysis of Variance of Combination of Filling Technique, Retreatment Procedure, and Root Thirds
R 2 = 0.399 (adjusted R 2 = 0.355).
Descriptive Statistics and Tukey Post Hoc Comparison Results of Smear Layer Score Values
The different superscript lowercase letters in same column represent significant differences between retreatment procedures (p < 0.05). The different superscript capital letters in same row represent significant differences between root thirds (p < 0.05).
C, thermoplasticized injectable; CLC, cold lateral compaction; PTUR, ProTaper Universal retreatment.
Stereomicroscope evaluations showed carbonization areas in some of the specimens from 3.0 W laser groups, while the teeth from 1.5 W laser groups were free from carbonization (Fig. 2). In addition, SEM images showed more cracks in the groups that were irradiated using 3.0 W laser than in the groups irradiated using 1.5 W laser and PTUR (Fig. 3).
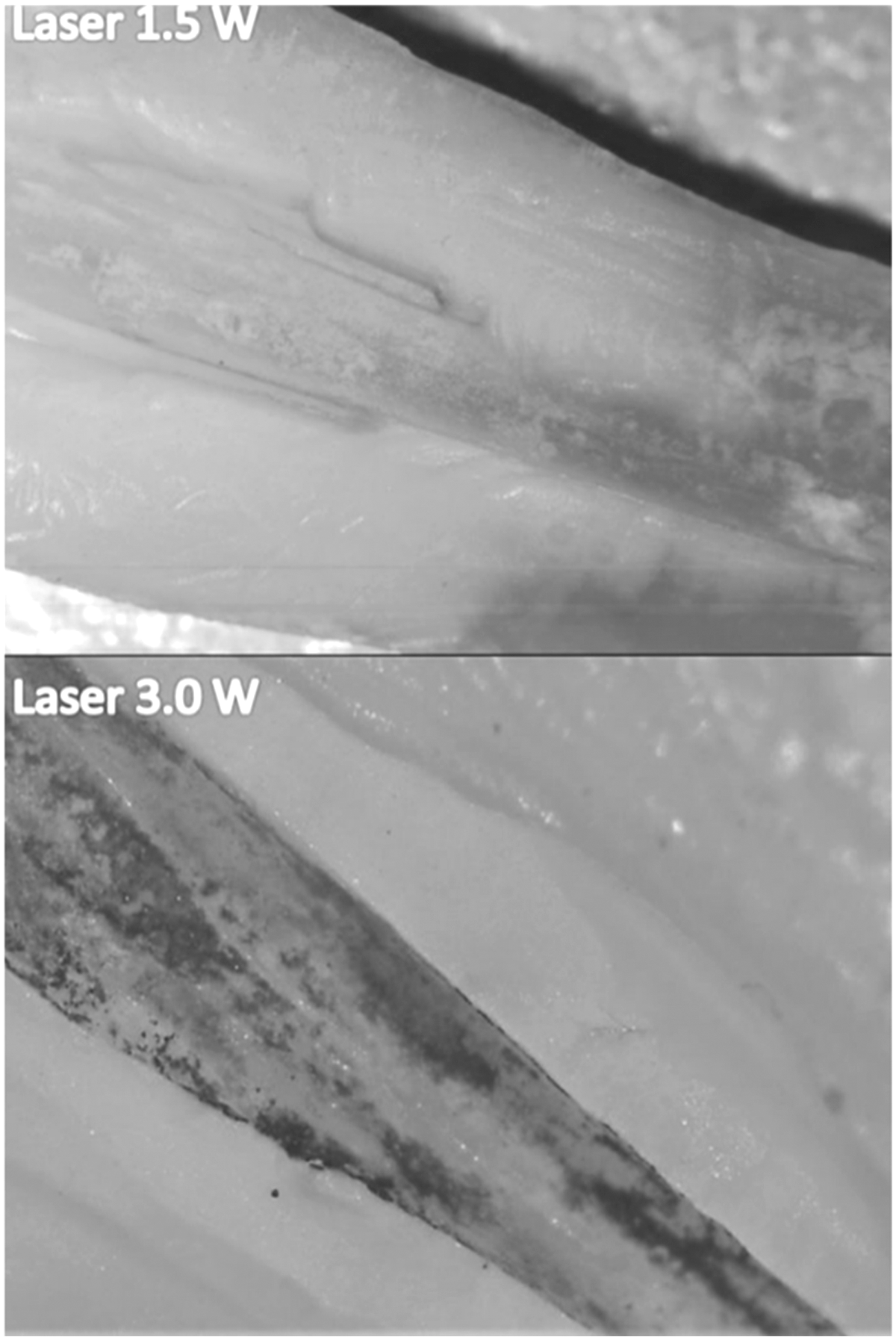
Stereomicroscope images at 18 × magnification of carbonizations in the root canal in group at 3.0 W, while no carbonizations in group at 1.5 W.
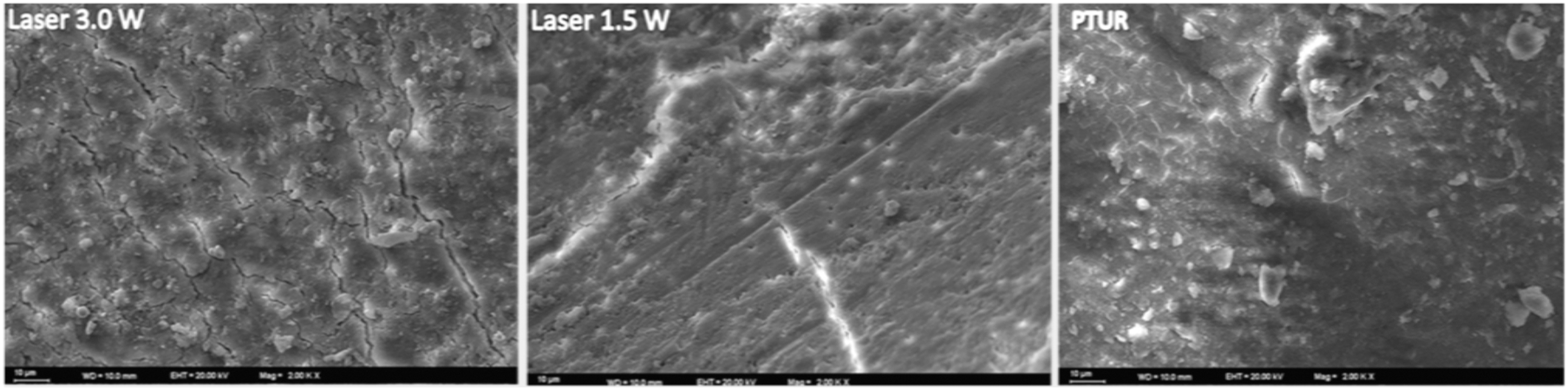
SEM observation at 2000 × magnification of cracks in samples from 3.0 and 1.5 W laser and PTUR groups, respectively. PTUR, ProTaper Universal retreatment.
Discussion
It is known that the complete removal of previous root canal filling materials during a retreatment procedure is necessary to eliminate bacteria and sufficiently remove SL from the root canal walls. 3,21 The results of this study support those from previous studies in which none of the retreatment procedures completely removed the SL and filling remnants from the root canal system. 21 –23 With regard to the literature, 24 no solvents were used in this study to prevent their effects on our results; softening the filling materials with solvents could push these materials further toward the irregularities along the canal wall.
PTUR system was used in this study to remove the filling materials from the root canals filled using two different techniques. However, the statistical analysis showed no significant differences in remnant filling materials when comparing C and CLC techniques after the retreatment procedures, which is in agreement with previous studies. 25,26 According to this study's results, a significant amount of filling materials was left in the canal after using PTUR. Several studies have reported that PTUR instruments were less effective than hand instruments in removing the previous fillings and SL. 5,27 Because of this, additional procedures should be applied to increase the retreatment success rate. Er,Cr:YSGG laser was used in this study because of its ability to remove the SL and debris with minimal side effects. 17,28 RFT2 (275 μm diameter and 21 mm length) and RFT3 (415 μm diameter and 17 mm length) fiber tips of this laser device were developed for endodontic treatment. The RFT2, which is longer and thinner than the RFT3, was selected for canal irradiation in this study due to its ability to reach the apical third of the root canal.
Previous studies have evaluated other laser devices, such as diode, Er:YAG, and Nd:YAG lasers, for retreatment procedure, and they have shown their efficiency in removing filling remnants and SL. 22,29,30 However, to our knowledge, there have been no attempts to evaluate Er,Cr:YSGG laser for the removal of remnant obturation materials in retreatment cases in the literature. Er,Cr:YSGG laser is a water-absorption infrared laser that has the potential to clean dental hard tissues by causing a small burst in these tissues. In addition, several studies have reported that Er,Cr:YSGG laser irradiation produces a minimal temperature increase that is not high enough to damage the periodontal tissues. 15,18,31,32 This is why temperature increase during the laser irradiation was not measured in this study.
The effects of different output powers (1–6 W) of erbium lasers have been studied previously. Cracks, carbonizations, and thermal damages on the canal walls were the results that have been reported when using a high output power (>4 W). 12,13,15 Therefore, we decided that irradiation between 1.5 and 3.0 W was suitable for the retreatment cases due to the presence of gutta-percha and sealer on the canal walls, which required a higher output power to remove them. According to the results of this study, the higher laser power (3.0 W) was more effective on removing SL and residual filling materials than the other retreatment groups in the coronal and middle thirds of the root canal. This is consistent with some previous studies, 12,13,15 but not in agreement with other studies. 14,33 These differences between the studies could be because our study was conducted using retreatment teeth that had remnants of gutta-percha and sealer on the canal walls, in addition to SL.
Regardless of the retreatment procedure, the results of this study showed more effective SL removal in the coronal and middle thirds than the apical third, which is in agreement with the results of previous studies. 4,34 –36 This could be because the fiber tip of laser was moved in circular motion in the coronal and middle thirds, while it was moved parallel to the canal wall in the apical area, without touching the residual materials and SL. In addition, the increased number of lateral and accessory canals in the apical region may be another reason for this finding. However, the results of this study and previous studies have shown that Er,Cr:YSGG laser alone is not an ideal tool for removing SL from the apical third of the root canal. 14,34 –36 Further investigations in future studies are required to improve root canal wall cleaning in the apical third after retreatment, such as a combination of Er,Cr:YSGG laser irradiation and irrigation solutions or using ultrasonic systems with a laser. 37,38
According to the results of this study, carbonizations and cracks were observed in some of the specimens from the 3.0 W laser groups; however, no teeth in the 1.5 W laser groups were carbonized, but a few of them were cracked. These findings are consistent with those of some previous studies, 14,33 but they were not in agreement with the results of other studies. 12,13,15
The results of this study may not be associated with clinical situations because the evaluations were performed in the laboratory on extracted teeth. In addition, irrigation solutions, which play a role in root canal cleaning and disinfection, in combination with laser irradiation were not investigated. These factors could be considered limitations of this study.
Conclusions and Summary
Within the limitations of this study, Er,Cr:YSGG laser at 3.0 W output removed SL and remnant filling materials more effectively than the other retreatment procedures. However, Er,Cr:YSGG laser should be used carefully because the 3.0 W output power caused carbonization areas and cracks in some of the samples. Unfortunately, none of the retreatment methods was able to entirely clean and remove the SL and filling remnants from the root canal system.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding provided for this article.