
Abstract
Background:
Orofacial pain has been a prevalent symptom in the worldwide population, which may cause restrictions in daily activities and, consequently, have a great impact on the well-being of affected individuals. Photobiomodulation using light sources, such as low-level laser or light emitting diodes, with different wavelengths, has been widely used in the last years, in addition to being a noninvasive, low-cost resource and reducing pain.
Objective:
This study aimed at evaluating the effect of photobiomodulation as a protocol treatment to prevent facial muscle discomfort after long-term clinical procedures.
Methods:
The volunteers were randomized and allocated as follows: laser (n = 16) and placebo (n = 16) groups, following a crossover study design. The laser parameters were as following: 786 nm wavelength, 9 J per point, and 100 mW power of 2.393 W/cm2 irradiance. The discomfort was induced by simulating a 50-min dental procedure (with bilateral mouth open), and the pain scale (assessed bilaterally), tiredness, and temperature measurement through thermography were used for analysis.
Results:
The results showed a significant lower pain and tiredness in the laser group. Also, the results showed a statistically significant valid temperature change between the groups at times: T1, T40, and T50.
Conclusions:
According to our results, photobiomodulation showed a positive effect on the face musculature in patients submitted to the treatments, reducing pain and improving the subjective perception of exertion.
Introduction
Musculoskeletal pain has been a widely prevalent symptom in the worldwide population, 1,2 which may cause restrictions in daily activities and consequently may have a large impact on the well-being of affected individuals. 3 It has been reported 4 that unknown exercises, predominantly eccentric, may result in immediate symptoms and muscle injury, such as decreased strength, reduced range of motion, stiffness, and pain. Eccentric contractions-concentric high intensity of masticatory muscles induces muscle pain, fatigue, and functional impairment of the jaw. The fatigue induced by the motor task sustained in the jaw lift muscles of healthy patients and patients with temporomandibular disorder (TMD) has been previously studied and the results suggest that patients with TMD are more easily fatigued when compared with healthy individuals; however, the activation process muscle during the fatigue test was similar between healthy patients and those with TMD. 4,5
Pain is an important symptom that signals damage to tissues or agents that are potentially harmful to the body, evoking protective sensory and motor responses. In addition, it has a significant impact on the well-being and functional capacity of people affected, consequently becoming a burden for economic productivity and the health system. 6,7
Photobiomodulation using light sources, such as low-level laser or light emitting diodes, with different wavelengths, has been widely used in the last years, moreover, it is a noninvasive and low-cost resource. Photobiomodulation treatment has shown promising results in decreasing pain, muscle fatigue, and to improve muscle performance in relation to strength training and recovery from exhaustion. 8 –11 This treatment promotes alterations in metabolism, inducing molecular, cellular, and systemic changes and promoting a photobiological response in cells.
Thermography is the technology of the radiation detection graph that records infrared (IR) radiation with points for temperature comparisons. For Kim et al., 12 in the areas of biotechnology and orthodontics, thermography contributes to the diagnosis of facial nerve injury, comparing clinical symptoms and temperature difference as a result of altered blood flow in the injured areas, in addition to the detection of IR emitted by the body. In addition, it is important to assess the temperature in the human body using asymmetries to assist in the prognosis and diagnosis of dysfunctions. The new technology may be considered a noninvasive, painless, and noncontact method, widely used in the recent biomedical field. 13
In this manner, this study aimed at evaluating the effect of photobiomodulation on facial muscle discomfort and variation on skin surface temperature of healthy individuals after undergoing a long-term simulated dental procedure.
Materials and Methods
After the approval of the Human Research Ethics Committee of the Dental School, Nove de Julho University (Protocol No. 3.078.432), a randomized-controlled, blind/placebo, clinical, and crossover trial was developed at the Integrated Health Clinic of the Nove de Julho University (UNINOVE). The protocol of this study was registered in Clinical Trials (Clinical
Inclusion criteria
Healthy young people aged between 18 and 34 years, with no previous diagnosis of TMD.
Exclusion criteria
Individuals under orthodontic and orthopedic treatments, psychological or physical therapies, and using muscle relaxant, anti-inflammatory agent, or bite plate were excluded. Moreover, patients presenting frequent headache, bruxism, facial pain, fatigue/difficulty when chewing, parafunctional habits, and psychological aspects were also excluded. After applying the Research Diagnostic Criteria for Temporomandibular Disorder (RDC-TMD) questionnaires, individuals who presented a diagnosis in the groups I (myofascial pain), II (articular disc displacement), or III (arthralgia, osteoarthritis, and osteoarthrosis of temporomandibular joint) of the RDC-TMD were also excluded from the study.
Volunteers and randomization
The volunteers were divided into two groups (laser and placebo therapies) based on a randomization method involving an opaque sealed envelope stipulating to which group a given volunteer would be allocated. The envelopes were opened at the beginning of the evaluation session.
The volunteers were randomized and allocated as follows: laser (n = 16) and placebo (n = 16) groups (Fig. 1). For the groups, eight men and eight women were allocated.
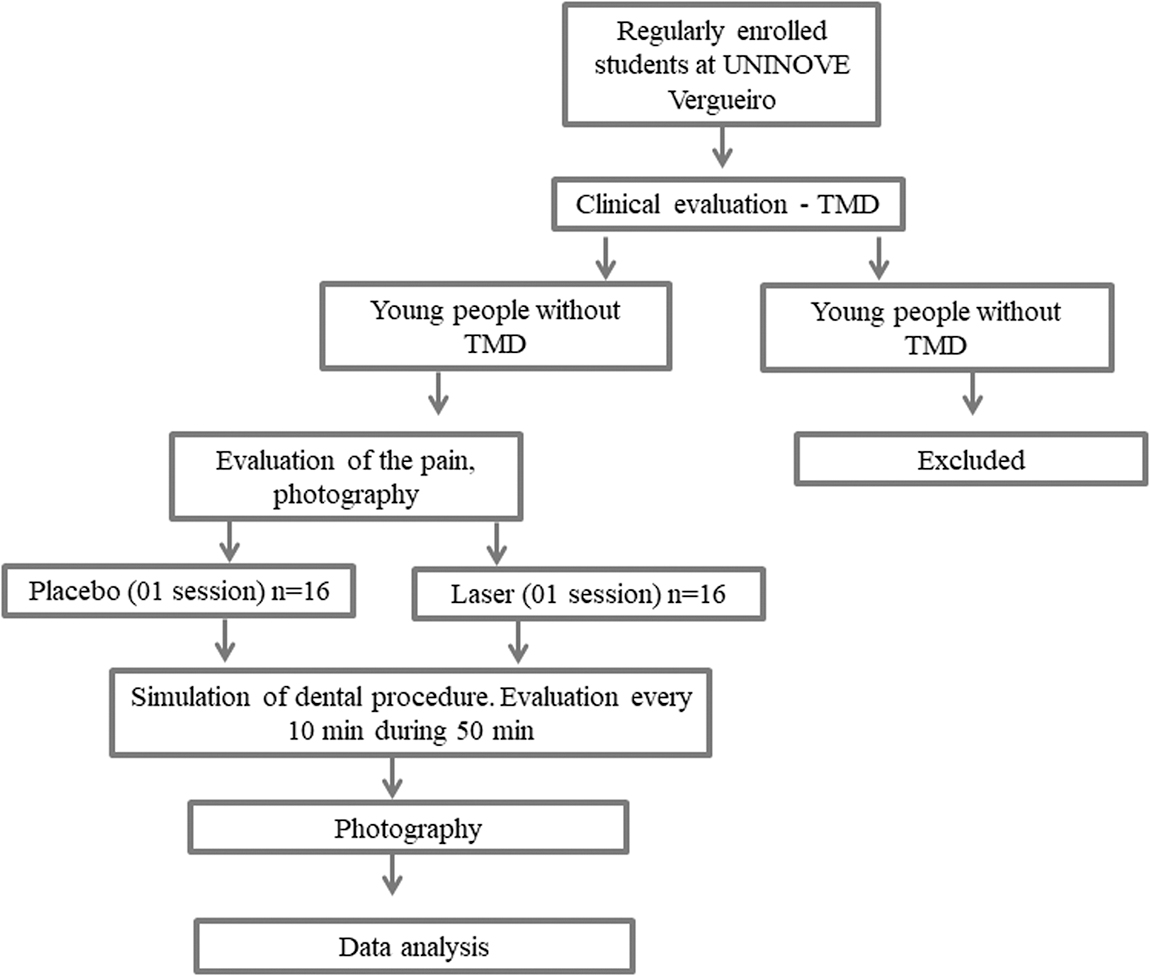
Flowchart illustrating the volunteer recruitment and treatments.
Procedures
The patients were followed to simulate a long-lasting dental procedure, with mouth open during 50 min. The monitoring and verification were done every 10 min of the scales aforementioned. Electroneuromyography was performed in the following two stages only: beginning and end times.
Evaluations
Questionnaire
The RDC-TMD questionnaire was filled out by the volunteers to evaluate TMD. A single examiner who had previously undergone by a training exercise performed a specific clinical evaluation. The evaluation involved palpation of the trapezius, sternocleidomastoid, temporal, masseter, digastric, and medial pterygoid muscles, palpation of the temporomandibular joints, analysis of mandibular movements with the aid of digital calipers, 14 and the determination of joint sounds with the aid of a stethoscope. Frequent headache, facial pain, fatigue/difficulty when chewing, bruxism, psychological aspects, and parafunctional habits were also evaluated 15 to exclude these patients as aforementioned in the Exclusion Criteria section.
Electromyography assessment protocol
Surface electromyography (EMG) is intended for the study of bioelectric phenomena. It is characterized as a noninvasive and easy method to perform. 16,17 The muscles analyzed with EMG were masseter and temporal anterior beam (right and left sides). The evaluations took place in three situations: (a) at rest, (b) maximum habitual intercuspal position using a Parafilm M® 40 blade between the molar teeth to collect the maximum voluntary contraction (MVC) of the studied muscles, and (c) maximum intercuspation (isometry) without parafilm. For all collections, three repetitions were performed with an interval of 1 min among collections. The collection time for each condition was 15 sec for rest and 5 sec for MVC.
Pain Catastrophic Scale
Pain may be considered a subjective and personal experience, and its perception is multi-dimensional in nature; different in both sensory intensity and quality. It is still influenced by affective-emotional variables. Pain Catastrophic Scale (PCS) is defined as negative orientation to certain painful stimuli and has been related to negative functional outcomes and pain. 18 PCS was described by Sullivan et al. and it is a self-assessment scale to measure catastrophic thinking about pain. 19 The instrument provides a good catastrophizing index through the highly correlated subscales of rumination, magnification, and helplessness.
Pain assessment by Visual Analog Scale
The one-dimensional scale used was the Visual Analog Scale (VAS) evaluation, which is limited to assess pain intensity only at the current moment. Analyses using only one-dimensional scales are simple and limited. The visual scale ranges from 0 to 10. 18
Tiredness assessment (BORG)
Borg Scale or Borg Table is a scale created by the Swedish physiologist Gunnar Borg for the classification of subjective exertion perception. On a numerical scale from 0 to 10 readjusted from the original from 0 to 20, the individual uses the scale to point out his/her own perception of effort. 19
Thermographic camera evaluation
For an accurate evaluation, an air-conditioned room was used. Also, the same points were used on the right and left sides of each participant. The thermal camera used was FLIR C2. The C2 thermal camera features FLIR's exclusive MSX, which adds important details of the integrated visual camera to the IR image in real time. The result is a complete undiluted thermal image with visible light capabilities that instantly recognize where the troublesome heat pattern is. Full radiometric images measure the temperature at any point in the image for further analysis from −10°C to 150°C. The software used for thermal image analysis was FLIR TOOLS, version 5.11.16337.1002 (Fig. 2).
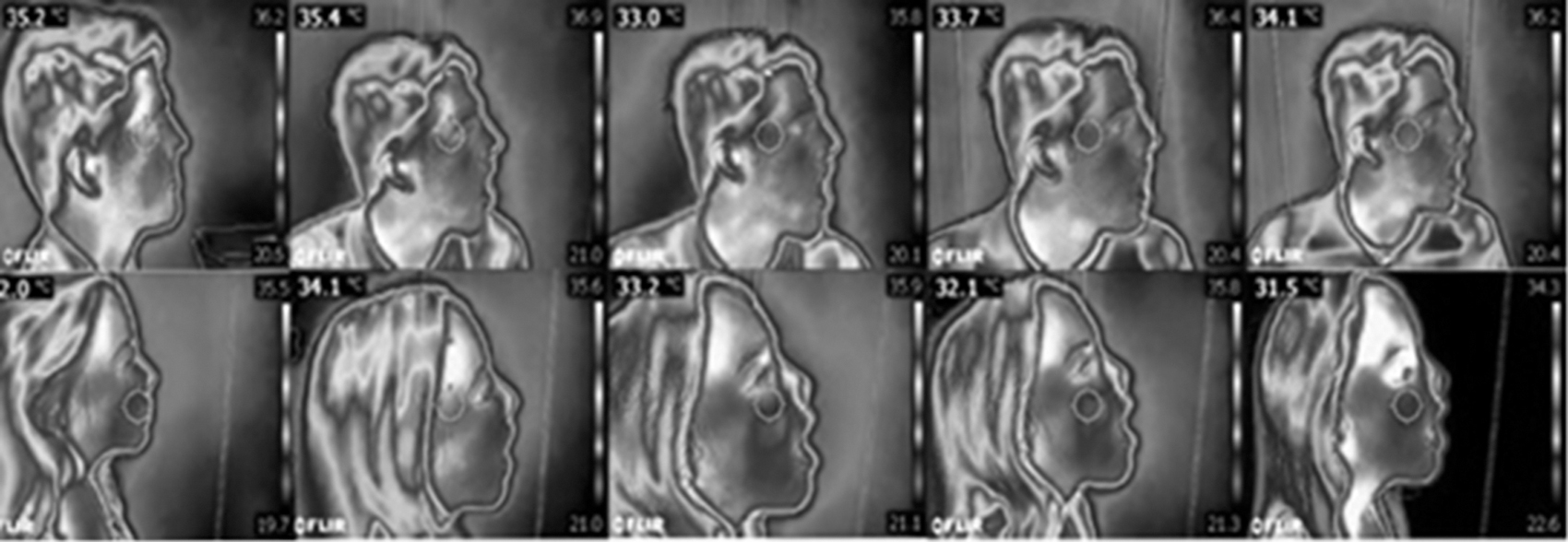
Thermographic camera evaluation.
Test preparation
(a) The camera used was an FLIR 60 Hz, with thermal resolution of 0.08°C and 0.1 mm spatial, with 320 × 240 integrated real resolution pixels in 16 bits.
(b) The test chamber (room) was kept at a temperature between 20°C and 22°C, as suggested by the International Thermography Protocol (IACT) and relative humidity between 50% and 70%.
(c) Images were taken at a distance of 50 cm by a single operator.
Photobiomodulation therapy
Photobiomodulation therapy (PBMT) was carried out with the Twin Flex Evolution® device (MM Optics). A comfortable seating was given to the volunteers in a soundproof room. The Frankfurt horizontal plane (the lowest point of the orbital margin to the highest point of the external acoustic meatus margin) remained parallel to the ground. The irradiation sites were cleaned with 70% alcohol. A transparent plastic wrap was placed over the active tip of the laser to avoid cross-contamination.
Laser application protocol: Three points of the masseter muscle (upper, middle, and lower portion) and one anterior temporal point on each side of the face (four points each side, in a total of eight points) 20 were irradiated in the laser and placebo groups, using a wavelength of 786 nm, with radiant exposure of 225 J/cm2, power of 100 mW, and irradiance of 2.493 W/cm2 for 90 sec per point, resulting in an energy of 9 J per point and a total of 72 J per volunteer. The application were timely, conventional tipped, and in contact with the skin, considering the area of 0.04 cm2. All the laser parameters are presented in Table 1.
Infrared Laser Usage Parameters
For the placebo group, the same device was used with the same irradiated points and the same application time per point, in contact with the skin, but the device was not turned on and a recording reproducing the device's audible warning was used.
The same patients participated in the research, at different times, and were submitted blindly to the laser group at one time and, at another time, were submitted to the placebo group (crossover design).
Statistical analysis
The paired t-test (parametric test) was used when data from both groups did not reject the normality hypothesis. However, Wilcoxon test (nonparametric test) was used when one of the groups rejected the normality hypothesis. Breach of the normality hypothesis was detected by the Shapiro–Wilk test in right and left t 30, so where there was a breach of the normality hypothesis, a nonparametric test was used, and when there is no breach of the normality hypothesis, a parametric test was used. The sample is homogeneous because all left the same baseline, which shows significance in the results found.
Results
No significant statistical differences were found in EMG between the placebo and laser groups at the beginning and end of the evaluation (p > 0.050) (Fig. 3).

EMG between the sham and laser groups. EMG, electromyography.
The total average value of catastrophic thinking was 1.65 points, indicating a low rate. No statistically significant correlation was detected between pain catastrophization and pain. When comparing the groups regarding VAS, significant results were found (p < 0.05). It could be shown that, at all times, the placebo group presented higher VAS results than the laser group (Fig. 4).
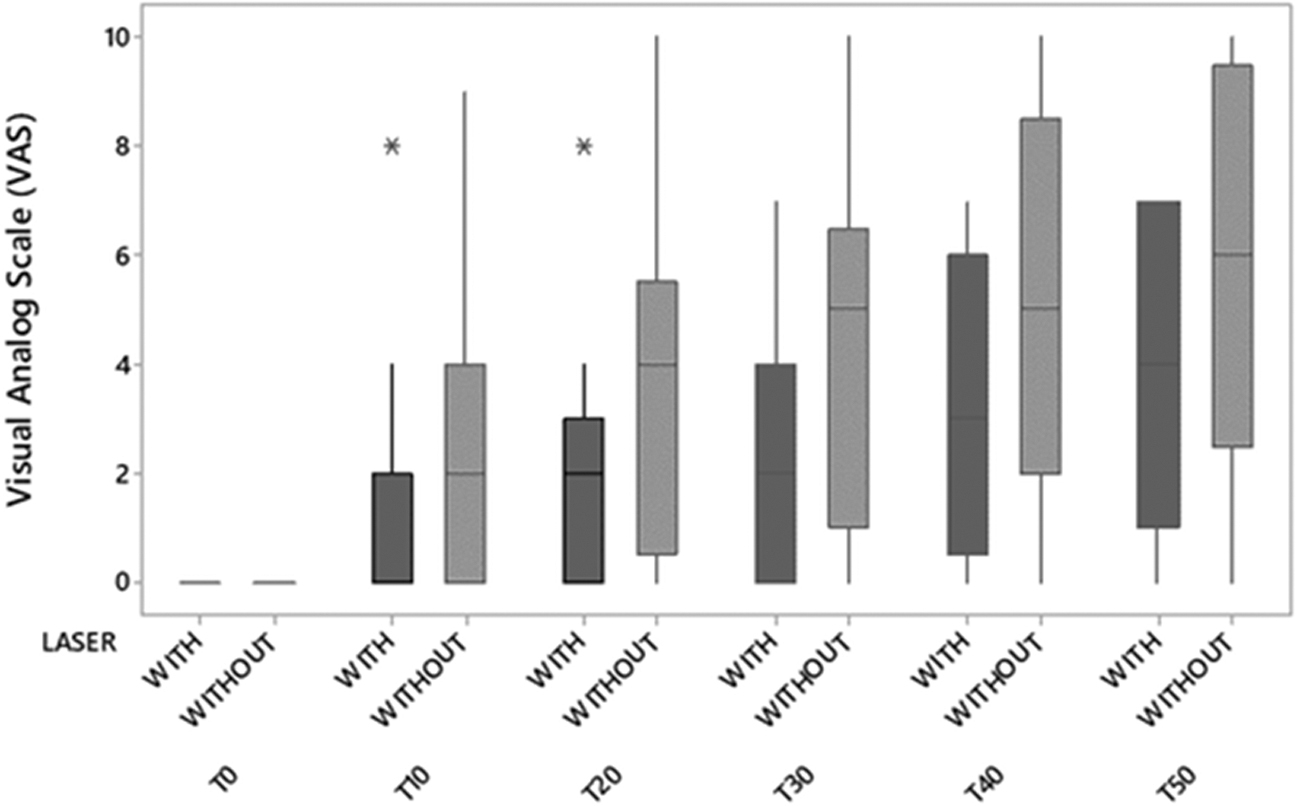
VAS between sham group and laser group. VAS, Visual Analog Scale.
Comparing BORG scale measurements between groups, the data from the BORG scale, used to point out pain and perceived exertion over the 50 min of dental procedure simulation in the two groups studied, are shown in Table 2.
BORG Descriptive Statistics According to Wilcoxon Test Groups and Results
For the laser and placebo groups, a significantly statistical correlation coefficient was found between VAS (T50) and BORG (T50). This coefficient is positive, as the VAS score increases, the BORG score also increases. Thus, the VAS and BORG show decreased pain and tiredness after using the laser throughout the study.
Regarding the assessment of temperature on the left side, a significantly statistical difference was found at the following periods: T0, T40, and T50 when comparing both groups. At these times, in the laser group, the average temperature was higher than in the placebo group. Statistically, it was observed that in the laser group throughout the dental simulation, the local temperature increased. This could be justified by the state of electronic excitation that a notable fraction of the excited energy is converted into heat, generating an increase in the local temperature in the absorbing chromophores, which is a possible mechanism of action of the laser (Fig. 5).
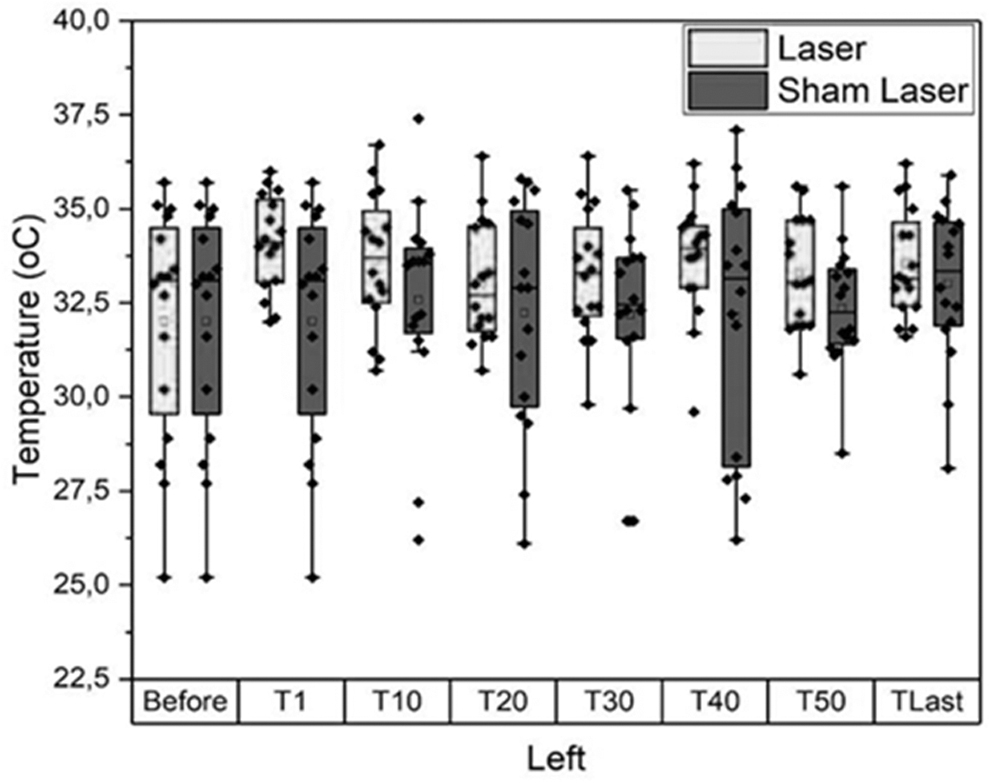
Temperature measured between control group and laser group, left side.
The results were similar for both sides. This result is important, since the same individuals participated in the laser and placebo groups, and the right and left sides were evaluated in the same individuals.
Right side: A significantly statistical difference was found at the following times among the groups T0, T40, and T50. At these times, the laser group had an average higher temperature than found in the placebo group. Statistically, it can be observed that in the laser group throughout the dental simulation, the local temperature increased. This result can be justified by the state of the electronic excitation that a remarkable fraction of the excited energy is converted into heat, generating an increase in the local temperature in the absorption of the chromophores (Fig. 6).
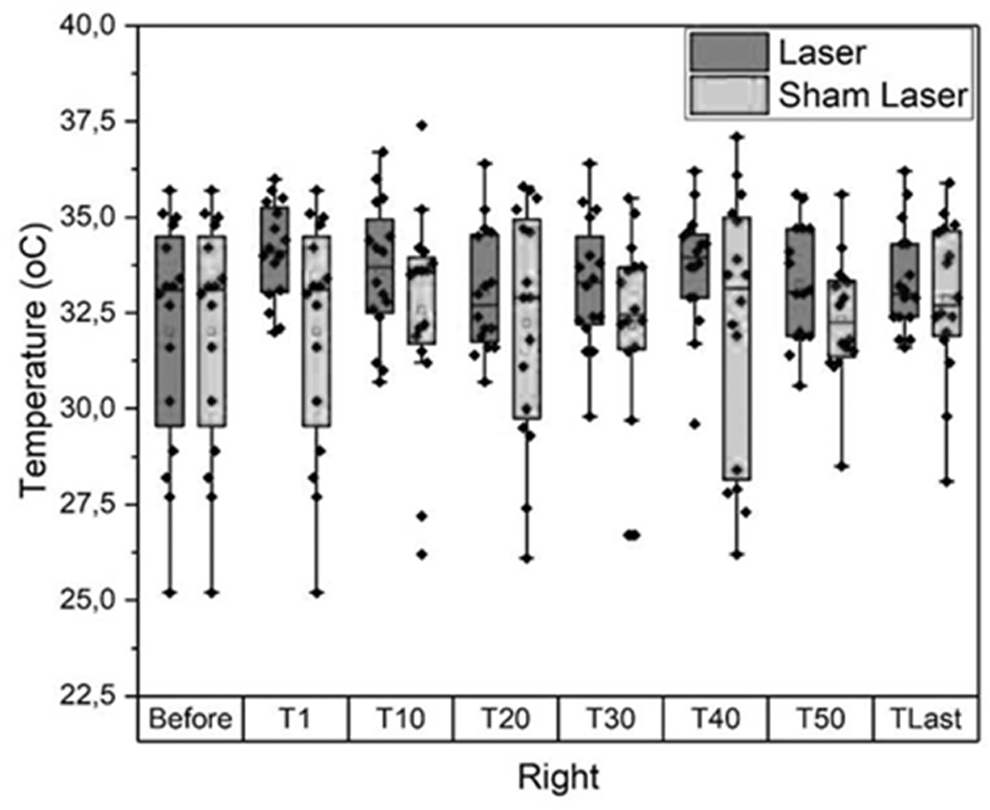
Temperature measured between control group and laser group, right side.
Discussion
Considering the complexity and subjectivity of the painful phenomenon, several aspects of this multi-dimensionality cannot be excluded, such as the biological, social, spiritual, and psychological aspects. The present study included PCS, BORG, VAS, mouth opening measures, and use of EMG for patient assessments. According to our results, the laser group showed a statistically significant reduction in pain and improving the subjective perception of effort.
A previous systematic review 21 concluded that for patients with TMD, PBMT effectively relieved pain and improved functional outcomes. Although this study did not investigate the PBMT for orofacial discomforts only in long-term clinical procedures, it showed satisfactory outcomes for patients with TMD. Other previous studies 22 –24 also corroborated with our findings as PBMT contributed as a clinically effective therapy for managing patients with temporomandibular joint pain. There are some studies in the literature with regard to the orofacial discomfort of the patients after dental procedures, such as edema and trismus after extraction of third molars. 25 –27 However, there are no studies regarding orofacial discomfort of the patients during a long-term dental treatment. In this way, our study showed promising outcomes using PBMT before starting the treatment, which may help to decrease this discomfort during dental procedures.
PBMT has the mechanism of local analgesic action, acting directly in the reduction of inflammation, which favors the elimination of allogeneic substances, stimulates a reflex action leading to the production of substances such as endorphins, in pain block, and thus improving local microcirculation and blood supply in areas with muscle tension. 21,28 –30 Therefore, laser therapy acts as a resting membrane potential stabilizing factor, acting directly on the nerve endings and maintaining analgesia lengthened, making it difficult to transmit local painful stimuli. 31 –33
In the present study, at all times, the placebo group presented higher VAS results than the group with laser. This result means that the placebo group presented statistically more pain than the laser group. Our results suggest that, in both groups, the initial moment was the one with the least pain and the pain scale increased as time increased.
According to our results, the first measurement that evaluates whether the long-term procedures can cause muscle fatigue in patients or any injury was observed. Also, our study evaluated whether these same procedures even cause pain, discomfort, and tiredness; if catastrophic thinking prompted at the beginning of the assessment comes to influence the pain outcome; and if the mouth remains open even with long clinical procedures. After evaluating each result of the scales, these same patients were then exposed to the procedure again, but at this time, only using laser before the procedure. Thus, it is possible to stipulate the efficacy of the PBMT and to propose a possible preventive use of it before the dental consultations.
A previous study has shown that phototherapy (laser) is able to promote increased peripheral circulation, and consequently, local temperature of 0.5°C. 34 The wavelengths most commonly used in PBMT are between 600 and 1000 nm, a spectrum that corresponds to the “optical window of the skin.” PBMT has anti-inflammatory, analgesic, and cell proliferation inducing effect. 10 According to a previous study, the effects of PBMT can be long-lasting on the cutaneous tissue with regard to temperature. 35 Laser effects are dose dependent 36 and they have an effect on microcirculation, leading to vasodilation. When vasodilation occurs, the amount of plasma that migrates to the interstitium is larger, making the blood more viscous, which slows circulation. 37
The results presented in this study demonstrated a statistically significant valid temperature change among the groups at the times: T1, T40, and T50. The laser group presented an increase in temperature over the 50 min of simulation. According to the authors, the control of pain and edema may be related to increased local blood perfusion. According to Kosiak and Kottke, 38 rising temperatures increase cellular metabolism. The metabolic rate increases by 10% with each 1°C increase in tissue temperature.
In our study, at T1, a temperature increase was observed shortly after laser application, which demonstrates an expected clinical picture as shown in a previous study, 39 caused by some lasers. Also, the final T presented a difference on the left and right side that can be justified by the fact that the person uses musculature more on one side than on the other side.
Conclusions
According to our results, PBMT showed a positive effect on the face musculature in patients submitted to long-term treatments, reducing pain and improving the subjective perception of exertion. Also, the conditions tested in this study did not cause fatigue despite discomfort and pain. Under the experimental conditions used, it could be observed that PBMT did not promote statistical changes on local surface temperature at 10, 20, and 30 min, however, there was a statistical change at 40 and 50 min. Thermography with current technological resources is a promising and important means for diagnosing muscle pathologies and orofacial pain, where there is an exacerbation of sympathetic activity and possibly inflammatory process. As future studies, tests with a larger control group and tests with different dysfunction conditions are suggested to ensure greater reliability in the use of thermography technology. PBMT is a safe effective tool, widely studied in the literature in healthy and pathologically ill patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding received for this work.