
Abstract
Objective:
This randomized controlled trial aims to verify the efficacy of a combined fractional CO2 laser and rhodamine-intense pulsed-light (r-IPL) protocol in the photoaging therapy.
Background:
Skin aging is related to multiple environmental and genetic factors that give rise to different manifestations. In recent years many techniques have been proposed for the rejuvenation of the skin of the face such as ablative and nonablative procedures. Combination of laser or light sources with different wavelengths represents a safe and effective treatment method. r-IPL is a new pulsed-light technique capable to generate wavelengths varying from 550 to 650 nm proposed in nonablative photorejuvenation with a good efficacy and safety profile.
Methods:
Twenty-two patients (skin phototypes II–III, aged 46–67 years) were randomly allocated into two groups: group A was treated only with a therapeutic standard dose of the fractional CO2 laser, whereas group B was treated with a combined therapy of r-IPL and fractional CO2 laser. All patients were treated up to three times at a 2-month interval. Efficacy of the procedures was assessed thanks to the Fitzpatrick Wrinkle Severity Scale (scores 1–9) before treatment and at a 4-month follow-up from the last treatment.
Results:
Patients treated with the combination of r-IPL and fractional CO2 laser showed better results in terms of wrinkle reduction according to the Fitzpatrick Wrinkle Severity score (2.82 ± 0.87 vs. 3.09 ± 1.14), with a statistically significant reduction in healing times (7.82 ± 0.75 vs. 13.82 ± 1.94 days, p ≤ 0.001) and duration of post-treatment erythema (3.55 ± 0.93 vs. 8.18 ± 1.47 days, p ≤ 0.001). Patient satisfaction was higher after combined fractional CO2 laser and r-IPL treatment.
Conclusions:
Our data suggest that combined use of fractional CO2 laser and r-IPL may lead to excellent results in terms of skin rejuvenation with a simple post-treatment management and an optimal tolerability.
Introduction
Aging is a physiological progressive transformation that conducts to the gradual deterioration of the organs and consequent clinical and histological alterations. Incident ultraviolet (UV) radiation, inducing the formation of reactive oxygen species (ROS), which generate cellular oxidative stress, forms the basis of the photoaging process. 1 In fact, ROS can damage both the lipid components of the cell and the structures of the dermis, in particular collagen. It has also been shown how overtime fibroblasts and other skin cells express different genes that influence their biosynthetic capacity. 2
Skin aging signs include wrinkles, skin laxity, alterations in pigmentation, and teleangiectasias, which can be treated with different ablative or nonablative techniques. Typical ablative procedures include vaporizing tissue and removing epidermal layer, causing marked patient discomfort and longer healing times. 3 Gentler nonablative lasers stimulate collagen production in the dermis without epidermal damage, allowing shorter healing times. 4 Fractional carbon dioxide (CO2) laser produces dermal microthermal zones with consequent new collagen formation and skin tightening, being very effective in the process of skin rejuvenation. 5
In addition, intense pulsed light (IPL) has been widely shown as an effective and safe procedure to treat photodamaged skin. The effectiveness of IPL is founded on the theory that high-intensity light energy determines a rise in collagen fibers temperature and their consequent shrinkage. 6
Furthermore, recent studies showed that skin fibroblasts that receive IPL increase the formation of elastin and new type I and III collagen and the synthesis of extracellular matrix proteins, as demonstrated by post-treatment histological evaluations. 7 Rhodamine IPL (r-IPL) is a new IPL energy with a polychromatic emission with wavelengths ranging between 550–680 and 850–1200 nm, which has been recently proven to be a valid therapeutic approach in noninvasive photorejuvenation. 8
This randomized controlled trial aims to determine the effectiveness and synergistic safety of a combined fractional CO2 laser and r-IPL treatment.
Materials and Methods
The study included a total of 22 women (mean age 55.77 ± 6.05), with Fitzpatrick skin types II–III; the recruited patients were examined for signs of skin aging, such as wrinkles, dyspigmentation, telangiectasias, and skin laxity, and subsequently treated on the cheeks and followed up at the Dermatology Laser Unit of Florence and at the Dermatological Unit of Mater Domini Hospital of Catanzaro, Italy (Table 1).
Evaluation of the Effect of Fractional CO2 Laser Alone and Fractional CO2 Laser in Combination with r-IPL in the Treatment of Photoaging
Values in bold indicate statistically significant differences.
r-IPL, rhodamine-intense pulsed light.
Local research ethics committee approval was obtained (Calabria Centro Committee 2019/373).
Patients were randomly allocated into 2 groups: group A (control) included 11 patients treated with the fractional CO2 laser alone (43.2 mJ/DOT—D-Pulse—500 μm DOT spacing; SmartXide, Deka Me.La, Italy) with a therapeutic standard dose according to recent reports. 5,6
Group B, on the contrary, included 11 patients treated with a combination of the fractional CO2 laser (22.5 mJ/DOT—D-Pulse—750 μm DOT spacing) used at a lower energy to reduce healing times and side effects, and the r-IPL (RightLight SynchroVasQ; Deka Me.La, Italy) with the following parameters: fluence of 15 J/cm2—8 + 8 ms Delay 20 ms. All subjects were evaluated before treatment (baseline) and had a 4-month follow-up after the last treatment. Devices' characteristics are better described in Table 2.
Device Characteristics
The effectiveness of these treatments was assessed comparing the Fitzpatrick Wrinkle Severity Scale 9 (FWSS) (scores 1–9) before and after treatment, and asking each patient to rate his or her satisfaction (Dissatisfied, Slightly Satisfied, Satisfied, and Very Satisfied) (Table 1).
All patients were treated up to three times (less if they have reached very high satisfaction before the third treatment) with 2-month interval between each treatment.
After each treatment a nonsteroidal anti-inflammatory cream was applied once per day for 14 days. 10
High-resolution photographs were taken before and 4 months after the last treatment.
Statistical analysis using an unpaired Student's T test assuming equal variances was performed.
Post-treatment complications and side effects were also recorded.
Results
Patients in group B (treated with the combination of low-fluence fractional CO2 laser and r-IPL) showed better results when compared with group A (treated with fractional CO2 treatment in monotherapy) in terms of wrinkle reduction according to the FWSS (2.82 ± 0.87 vs. 3.09 ± 1.14), with a statistically significant reduction in post-treatment erythema (3.55 ± 0.93 vs. 8.18 ± 1.47 days, p ≤ 0.001), in healing times (7.82 ± 0.75 vs. 13.82 ± 1.94 days, p ≤ 0.001) and in the number of treatments (2.36 ± 0.50 vs. 2.91 ± 0.30, p: 0.006). FWSS score reduction was significantly better in group B (3.18 ± 1.08 vs. 2.36 ± 0.67 p: 0.045). Patient satisfaction rate was higher in group B: 64% of patients in this group were “very satisfied” with the treatment they received compared with 45% of patients in group A (Table 1).
In addition, the vascular component of aging skin was successfully treated in group B patients (Fig. 1). No serious adverse events were reported throughout the study period. Photographs taken at baseline and 4 months after the last treatment demonstrated relevant improvement of photodamaged facial skin (Fig. 1).
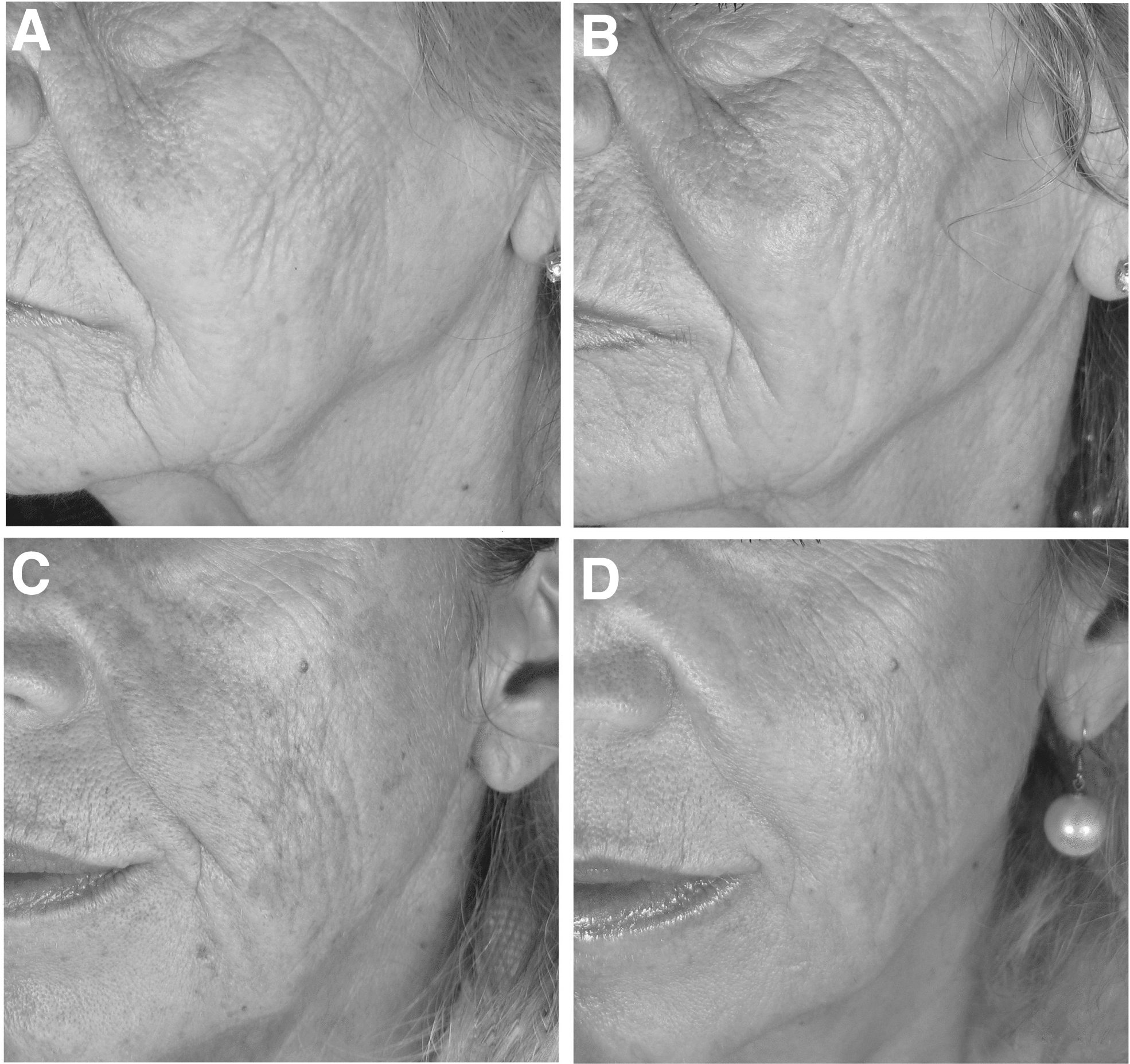
Patient No. 6 left cheek before treatment
Discussion
In this randomized controlled trial study, we compared the effectiveness and safety of fractional CO2 laser therapy in combination with r-IPL and fractional CO2 laser therapy alone in the treatment of photodamaged skin in 22 Caucasian women. We observed that compared with fractional CO2 laser treatment alone, low-fluence fractional CO2 laser combined with r-IPL significantly reduces signs of facial skin aging.
Recently, laser systems have become a powerful and effective tool in dermatology, plastic surgery, and esthetic medicine.
The current goal in laser treatment is to identify the minimal dose required to achieve optimal clinical outcome with the shortest healing time and the fewest side effects, to improve patient's comfort before and after treatment. 11
The combination of laser or light sources with different wavelengths may lead to targeting the disease in various ways, with safer and more effective treatments. 12
Subablative or minimally ablative lasers have been projected to achieve similar treatment outcomes reported with fully ablative devices, but with fewer post-treatment adverse reactions, including infections, post-inflammatory hyperpigmentation, persistent erythema, and atrophic scars. 13
Moreover, fractional CO2 lasers usually induce shorter healing times and downtime, reducing side effects. This therapeutic strategy has the ability to induce the dermis in producing new collagen, regenerating its texture and enhancing skin tone and softness. 14
Superpulsed CO2 may act as a powerful wound modulator by increasing basic fibroblast growth factor (bFGF) production and reducing transforming growth factor-b1 (TGFb1) secretion. 15
While promoting cell replication, in the mean time CO2 laser is probably able to adjust collagen organization against excessive fibrosis, hence reducing the risk of abnormal wound healing.
Resurfacing using fractional CO2 is effective in the treatment of various degrees of photodamage; also its high versatility makes this technique very useful in the treatment of acne scars or any cicatricial tissue (burns, surgery, or post-traumatic scars). 11
IPL is a complementary source of microablative cutaneous rejuvenation, with a range of actions within the visible and near-infrared spectra. IPL has significant biological effects on tissue, such as fibroblastic reorganization and collagen redistribution, by activating specific proteins (versican and decorin) with clear improvement in texture, skin tone, and texture of the epidermis, and a reduction in the discolored and vascular components. 16
Greater selectivity in the pulsed-light emission beam might also help provide even more targeted action on superficial and deep vascular structures. This could help improve control of the vascular component of scar lesions or vascular reactions induced by ablative treatment in patients with a tendency to scar formation.
r-IPL is a pulsed-light generator device operating with wavelengths from 550 to 650 nm, with performances similar to dye laser (595 nm). The r-IPL handpiece uses rhodamine as a fluorescent matter able to absorb electromagnetic radiations in the UV spectrum up to 550 nm, and re-emit these radiations in a range between 550 and 650 nm, with a rhodamine peak at ∼570 nm.
As demonstrated, r-IPL technology emits energy with a “vascular”-specific wavelength, similarly to the 595 nm Dye laser, targeting the hemoglobin chromophore with high selectivity and efficacy. 17,18
Observational and biochemical studies showed that the 595 nm Dye laser treatments induce a global improvement of scars, with a reduction of the TGFβ growth factor and an increase of the metalloproteinase (MMP) expression. 19,20 Based on these considerations, we developed an operational protocol combining fractional CO2 laser and r-IPL for the treatment of photoaging signs.
In this treatment protocol, different wavelengths (near infrared for r-IPL and far infrared for the CO2 laser) have been used to achieve controlled neocollagenogenesis and tissue remodeling, acting synergically and furthermore strengthening the microablative effect of the CO2 fractional laser with the nonablative effect of the IPL. Activation of cytokines to stimulate the correct epidermal turnover in the healing process has already been evidenced after the use of ablative and nonablative energy sources on aging skin. 14,15 Indeed, this novel combined strategy may help reduce side effects and healing times.
Conclusions
In this randomized controlled trial we compared the use of a fractional CO2 laser in monotherapy with a combined fractional CO2- r-IPL treatment: our results suggest that the combination of the two light sources may lead to better clinical results, with a faster postoperative management, a reduction in post-treatment erythema and number of treatment sessions, and an higher patient satisfaction.
Further studies with a larger sample of patients would be required to better assess the real effectiveness of this combined technique.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was needed to complete this study.