
Abstract
Objective:
The aim of this study was to assess shear bond strength (SBS) and failure analysis of adhesion of composite resin (CR) to caries-affected dentin (CAD) pretreated with the Er,Cr:YSGG (ECY) laser, photodynamic therapy (PDT), and etch and rinse (ER) used for cavity disinfection.
Materials and methods:
Methods used in this study included scanning electron microscopy (SEM), SBS analysis, failure analysis, and digital microscopy. The methods were adopted to assess bond integrity, CAD interface, smear layer, and hybridization. Thirty human third molars assessed clinically and having scores of 4 and 5 based on International Caries Detection and Assessment System (ICDAS) criteria were inspected. Infected dentin was removed. Dentin that was hard and stained pink was categorized as CAD. Ten samples were used in each group for pretreatment of CAD. Ten samples of healthy dentin [sound dentin (SD)] were collected separately and taken as controls. Samples were divided into the following groups: group 1: SD+ER; group 2: CAD+ER; group 3: CAD+ECY; and group 4: CAD+PDT after the pretreatment bonding agent was applied and the restorative procedure was performed using CR.
Results:
CAD conditioned with PDT before bonding to CR demonstrated the lowest SBS values (11.22 ± 0.77 MPa), whereas the highest SBS values were observed in the SD surface treated with ER (18.25 ± 1.22 MPa). In CAD and SD pretreated with ER, majority of failure modes were cohesive failure and admixed failure, whereas in CAD pretreated with PDT and the ECY laser, the adhesive failure mode was pertinent.
Conclusions:
The use of the ECY laser and PDT on CAD for cavity disinfection does not have potential for application in clinical settings as it decreases bond integrity of CR. Moreover, the ER pretreatment method for CAD and SD remains the gold standard.
Introduction
The success of a restorative procedure is dependent on bacterial removal from the carious dentin structure. 1 Only mechanical cleaning of the carious tooth raises concerns as the procedure is insufficient not only for eliminating bacteria but also because it results in removing excessive tooth structure, which may lead to tooth sensitivity, pupal violation, secondary caries due to microleakage, and finally treatment failure. 2
Caries removal should be based on the minimal invasive technique, which aims to eliminate soft, mushy, infected, and disorganized dentin, while preserving caries-affected dentin (CAD) harboring less bacterial load and with the ability to remineralize. 3 However, CAD needs to be disinfected before restoration. 4
Intrinsically, dentin is moist and a heterogeneous tissue, and adhesion to dentin is a sensitive technique that is challenging compared with enamel. 5 Irrespective of evolution in the adhesive system, the hybrid layer formed at the interface between the CAD and filling material over time experiences degradation, reflecting the endurance of the restoration. 3,6 Degradation of the smear layer is dependent on multiple factors, that is, the conditioning method, fluid intake, and bacteria in situ, which may result in degradation of organic components. 7,8
Therefore, in CAD, disinfection of the cavity becomes significant. Among cavity disinfectants, chlorhexidine is the most convenient, simple to use, and readily available disinfectant. 9,10 However, despite several advantages, its effect on adhesion is still unclear. 10 –12
The use of lasers in dentistry is not unusual. Among different laser prototypes, the Er,Cr:YSGG (ECY) laser has gained extraordinary acceptance with dentists as it is well absorbed by hard tissues. 13,14 Working at a wavelength of 2.78 μm, it ablates the dentin structure, eradicating the smear layer, and its antibacterial nature kills bacteria. 15,16 Its suicidal action is based on activation of water molecules in bacteria, resulting in destruction. 16
However, still, no consensus has been arrived at on whether bond values are improved when CAD is pretreated and disinfected with the ECY laser. Alkhudhairy et al. and Vohra et al., in their recent work, advocate its use on CAD surfaces. 13,17,18 However, Attrill et al. and Kameyama et al. oppose its application before the use of an adhesive. 19,20 Photodynamic therapy (PDT) for dentin in the presence of a photosensitizer (PS) is another alternative approach.
The procedure results in lysis of bacteria by producing reactive oxygen species and elimination of the smear layer when irradiated under light of a specific wavelength. 21,22 However, the effect of PDT as an alternative to conventional dentin pretreatment—etch and rinse (ER)—on CAD is still dubious with conflicting outcomes. 2,23 It is notable to mention that the use of PDT in canal disinfection has already shown promising outcomes. 23,24
According to our information from indexed literature, heterogeneity in the available evidence advocates the necessity to perform an in vitro study to evaluate the bonding interface of CAD pretreated with the ECY laser and PDT and conventional ER and also to assess the shear bond strength (SBS) and failure analysis of adhesion of composite resin (CR) to CAD pretreated with the ECY laser, PDT, and ER when used for cavity disinfection.
The hypotheses investigated were (1) CAD pretreated with ER will display better bonding to the CAD surface conditioned with the ECY laser and PDT and (2) the sound dentin (SD) surface conditioned with ER will exhibit better bond integrity than CAD pretreated with ER.
Materials and Methods
Thirty human third molars assessed clinically and having scores of 4 and 5 based on International Caries Detection and Assessment System (ICDAS) criteria were inspected, as shown in Table 1. The standards used to find affected and infected dentin were a digital micrographic examination, use of a dental explorer for surface hardness, visual examination, and staining of dentin.
International Caries Detection and Assessment System Criteria for Caries-Affected Dentin, Description of Clinical Criteria
Shear Bond Strength of Dentin After Different Pretreatment Methods
Different alphabetic superscripts denote statistically significant differences (Tukey multiple comparison tests).
Showing significant difference among study groups (analysis of variance).
CAD, caries-affected dentin; ECY, Er,CR:YSGG; ER, etch and rinse; PDT, photodynamic therapy; SD, sound dentin.
Modes of Failure Categorized into Adhesive, Cohesive, and Admixed Among Investigated Groups
Infected dentin that was mushy, dark stained, and soft was removed, whereas dentin that was hard and stained pink was categorized as CAD. 5,25 The tooth was excluded if the lesion was deep or shallow and having an ICDAS score of 6 (clinically assessed). The study was carried out according to the checklist for reporting in vitro study (CRIS) guidelines. 2,9
A periodontal scaler was used to remove organic and inorganic remnants (Henry Schein Dental, United Kingdom). Chloramine-T hydrate (95% concentration) was used to disinfect specimens. All samples were stored at 5°C until further use. Samples were positioned perpendicularly up to the cementoenamel junction within the section of polyvinyl pipes with an internal diameter of 3 mm.
Polishing was performed using silicon carbide paper, 320 grit, under running water before pretreatment. A power analysis using G*Power 3.1 (Heinrich Heine University, Düsseldorf, Germany) indicated that a minimum sample size of 9 for each group ensured a power of 80% to detect significant differences at a 0.05 significance level. Thus, 10 samples were used in each group for pretreatment of CAD and were allocated through a simple random sampling technique. Ten samples of healthy dentin (SD) were also collected separately and taken as controls. 2,26
Group 1, SD+ER: the SD structure was pretreated with conventional ER. Thirty-seven percent phosphoric acid (Harward, etch) was applied on SD for 20 sec, followed by washing of specimens and air drying for 15 sec without desiccation.
Group 2, CAD+ER: samples of CAD were considered and pretreated with the conventional ER technique, as demonstrated previously.
Group 3, CAD+ECY: PDT for CAD was performed using the ECY laser at a power of 4.5 W, frequency of 30 Hz pulse, duration of 140 μsec, spot size of 600 μm in diameter, energy density of 107.1 J/cm2, air pressure setting of 90%, and water pressure setting of 75% for 60 sec in a noncontact position of 3 mm, perpendicular to the CAD surface, using [mizoram (MZ)] tips of 6 and 8 mm. 15,17 Following ECY laser treatment of CAD, the specimens were washed using for 30 sec without being desiccated.
Group 4, CAD+PDT: PS methylene blue (MB) (Qualigens Fine Chemicals, Mumbai, India) at a concentration of 100 mg/L in the solution form was brushed on CAD. The PS was activated using a diode laser (Piccasso, Italy) for low-level laser therapy with power of 1.5 W, wavelength of 810 nm, and power density of 33 mW/cm2 in a continuous circular motion with a fiber optic tip of 0.5 microns and laser spot diameter of about 10 μm (1/e 2 ) placed perpendicular to the CAD surface for a duration of 30 sec. 2,9,10 This was followed by washing the dentin surface for 5 sec and air drying without being desiccated.
After pretreatment of CAD with ER, PDT, and ECY and SD with ER, a bonding agent (Tetric N-Bond Universal; Ivoclar-Vivadent) was applied in two strokes using a plastic microbrush applicator and gently scrubbed for 15 sec on all specimens and cured (Woodpecker, Pearson dental company, Sylmar, CA; 1400 mAH, wavelength 470 nm) for 20 sec.
A polyether mold having standardized dimensions of 3 mm diameter was placed on CAD and SD, and restorative material (MultiCore; Ivoclar Vivadent) was dispensed using a cement plunger placed using the incremental technique and light cured (Woodpecker, 1400 mAH, wavelength 470 nm, India). Following restoration, all samples were placed in a thermocycler (Automated Thermal Cycler; Applied Biosystems, CA) for 3000 cycles equivalent to 2 min 30 sec each at 5℃ to 60℃.
Digital microscopy, SBS, and failure analyses
A digital microscope (Hirox-KH7700) was used to assess the interface between CR bonded to CAD conditioned with the ECY laser and PDT. With the help the measuring software, measurement, manipulation, and capture of images were performed (Hirox, Measuring Software, CA). A calibrated measurement of 50 × magnification was used.
Specimens from all groups were positioned in a universal testing machine (UTM) (Instron 8500 Plus, Canton). The cylinder was subjected to controlled force, the chisel being vertical to the cylinder containing the composite. The force on the composite cylinder was applied at a crosshead speed of 1 mm/min. The force applied for debonding was measured in megapascals (MPa) and recorded through the digital display.
Failure analysis was performed with 60 × magnification of debonded surfaces using a stereomicroscope. The failure analysis was categorized into three modes: adhesive, cohesive, and admixed failure modes.
Scanning electron microscopy of the CR/CAD interface
A fractographic analysis was performed by taking two pairs of specimens from each group using a scanning electron microscope (SEM) (JEOL JSM-6360 LV, Tokyo, Japan). Samples were initially wiped using an ethanol swab and dried. Gold sputtering of specimens was performed for 180 sec at 40 mA to obtain a thickness of 6 nm. The specimens were examined at a different magnification at 20 KV by a single operator.
Statistical analysis
SPSS, version 22 (SPSS, Inc., Chicago, IL), was used for entering data. The difference between groups was calculated through analysis of variance using means and standard deviations. A Tukey post hoc multiple comparison test was used to identify differences between groups. p-Values <0.05 were considered statistically significant.
Results
SEM and digital microscopy
The illustrative digital microscopy image shows the appearance of CAD treated with the ECY laser and bonded to CR (Fig. 1A). Figure 1B demonstrates PDT for CAD using PS MB. The composite adhered to CAD using a dentin bonding agent, which is visible in Fig. 1A and B. Similarly, Fig. 1C validates a graphical SEM image of CAD and healthy dentin (SD).
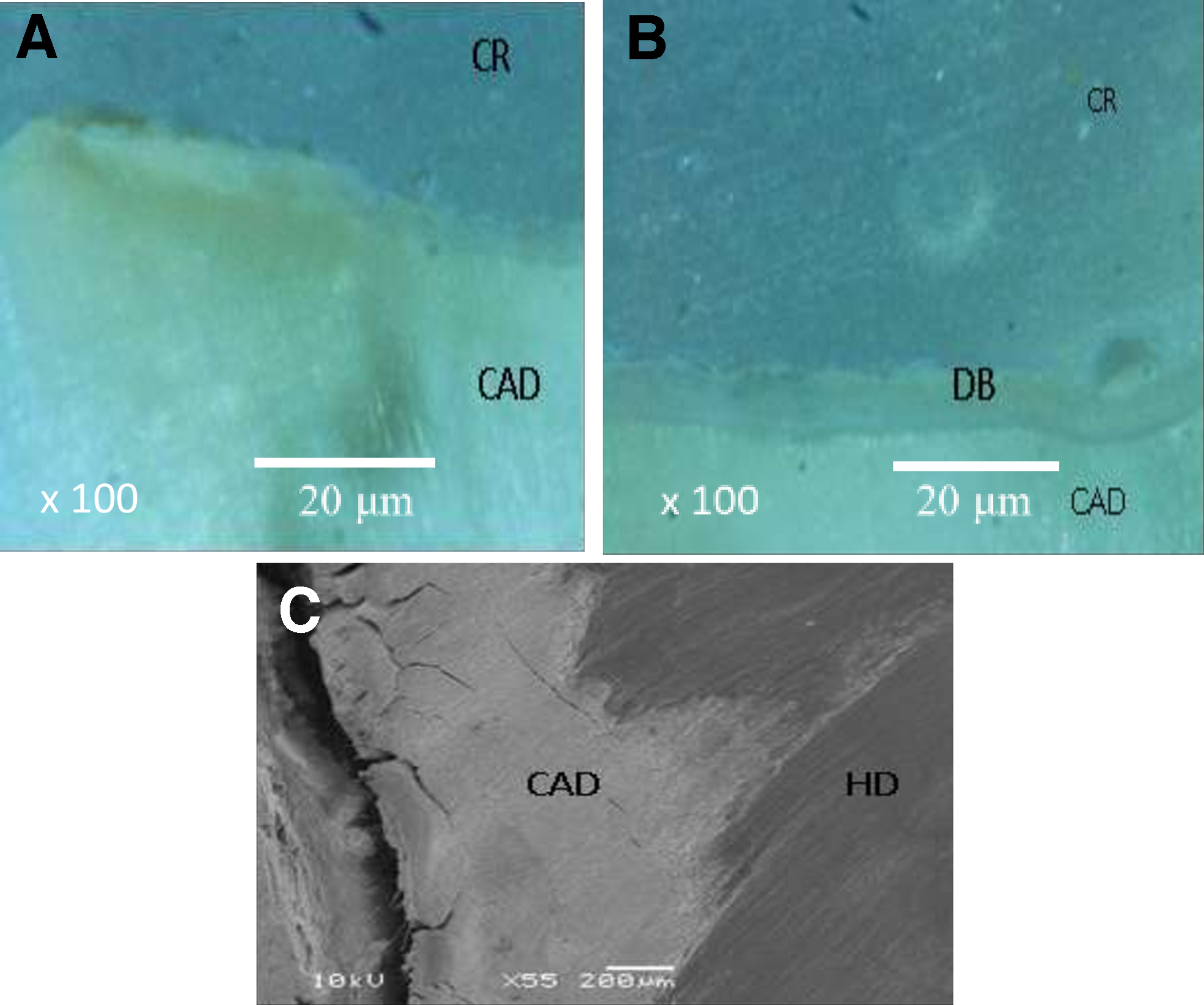
Appearance of carious dentin (CAD) treated with the ECY laser
The ECY laser on dentin demonstrates a rough eroded dentinal surface with flecks. The ablated surface is also noted with the use of ECY laser (Fig. 2). SEM (Fig. 3A) displays an image of CR bonded to CAD treated with PDT. Gaps are visible at the bonding interface due to sclerotic dentin.
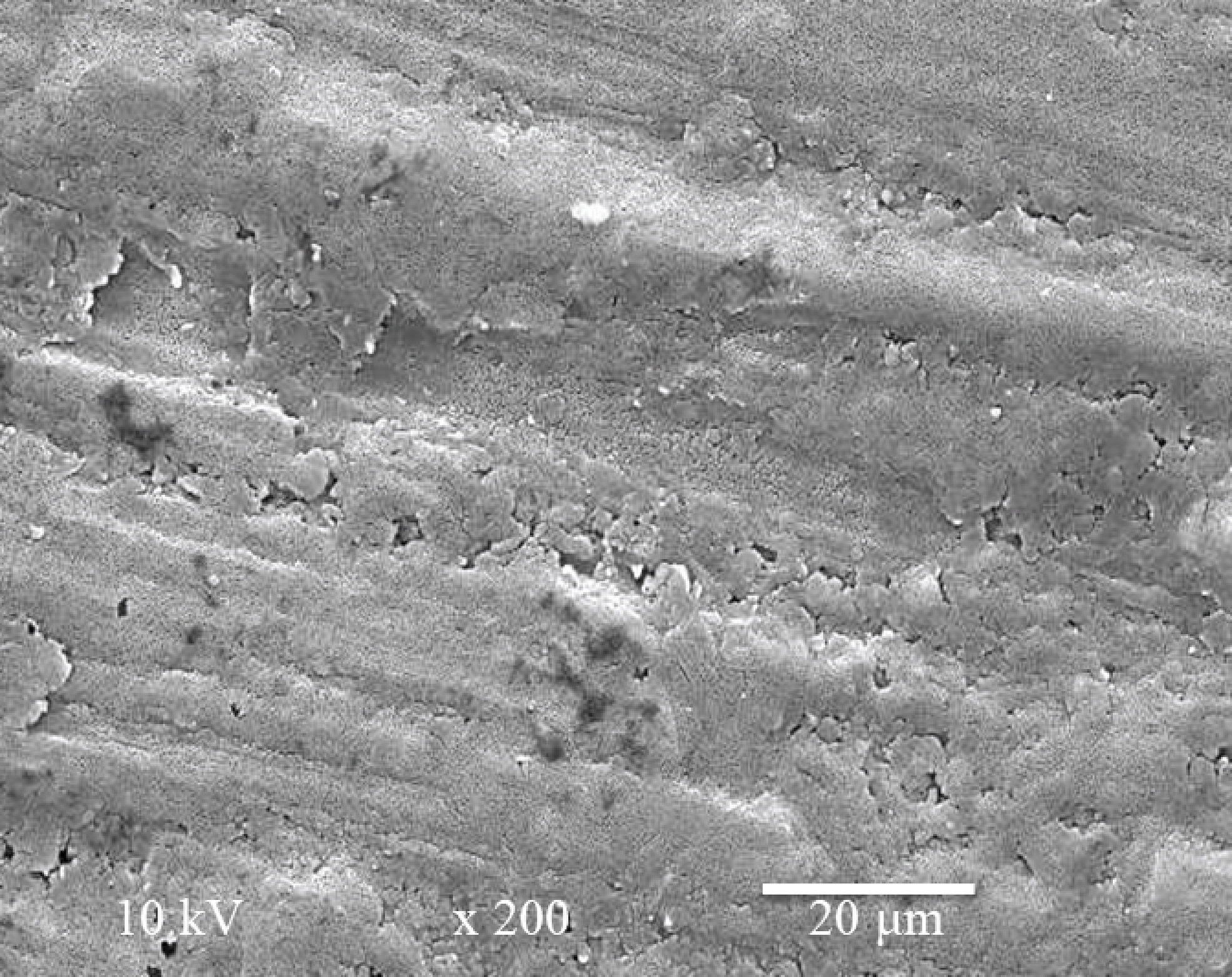
Presenting eroded dentin surface after the ECY laser treatment.

Figure 3C demonstrates fused dentinal tubules' lack of penetration of adhesive and CR and dentin sclerosis. Gaps are visible at the bonding interface. Figure 3B shows SD bonding to CR, showing no visible gaps, a good quality hybrid layer, and resin tag formation with visible penetration of adhesive.
SBS and analysis of failure modes
CAD was pretreated using three different types of methods. The normal distribution of data was assessed using Levene's test. CAD conditioned with PDT before bonding to CR demonstrated the lowest SBS values (11.22 ± 0.77 MPa), whereas the highest SBS values were observed on the SD surface treated with ER (18.25 ± 1.22 MPa).
The bond values of CAD pretreated with the ECY laser and PDT using PS MB were comparable (p > 0.05). Similarly, ER of CAD and SD before CR demonstrated no significant difference (p > 0.05).
No conclusive pattern of failure among samples was observed. In CAD and SD pretreated with ER, majority of failure modes were cohesive failure and admixed failure, whereas in CAD pretreated with PDT and the ECY laser, the adhesive failure mode was pertinent.
Discussion
The present study was postulated on two hypotheses: first, CAD pretreated with ER will display better bond values than CAD conditioned with the ECY laser and PDT; and second, the SD surface conditioned with ER will exhibit better bond integrity than CAD pretreated with ER. Both suppositions were accepted. A UTM was used for assessment of bond strength. UTM was preferred as its main advantage was its ability to assess the suitability and resilience of the material. 21
Adhesion of the adhesive was assessed by SBS. The method of SBS testing is cheap, simple, less time-consuming, and offers relative analysis of different groups simultaneously. SBS testing was favored with resin-based restorative material as the results are more reliable with less dubious outcomes. 23,27
The organic and mineral variations in CAD result in complex adhesion in comparison with SD. Our findings are consistent with other studies, indicating that when CAD and SD are treated with the same ER and adhesive system, SD will exhibit high bond integrity. 25,28 –31 There are multiple factors credited to this type of result. The carious process consists of two layers, the outer infected layer and the inner affected dentin, which is hard and sclerotic.
In CAD, the continuous process of demineralization and remineralization results in the formation of β-tricalcium phosphate (βTP) within dentinal tubules, which creates barriers to penetration of the adhesive. 32,33 This βTP is not readily soluble when treated with acid etching. 5,34 However, prolonged acid etching may permit incomplete dissolution of βTP, which further demineralizes CAD, resulting in funnel-shaped tags lacking cohesiveness of the adhesive, resulting in decreased bond values on the CAD surface. 31,35
Alterations in chemical and topographical characteristics of CAD may also be contributing factors to low bond strength. 36 Percentage of water content in CAD is far higher (14–53%) compared with SD (5%), compromising adhesion and hence decreasing bond values. 32,33 The SD surface treated with ER, as predicted, showed the highest bond scores. This is evident in Fig. 3B where CR bonded to SD, with a standard, thick hybrid layer and resin tags. Penetration of the adhesive in resin tags contributes to strong adhesion and perfect conservation of collagen architecture. 5
In the current study, CAD was pretreated with the ECY laser and the PS on CAD was activated by PDT. Both modern-day methods displayed bond values significantly lower than CAD treated with ER. PDT for the CAD structure in the presence of PS MB activated by a diode laser (low-level laser therapy) decreased bond values. Several conceivable clarifications are correlated with this conclusion. MB is cationic, it endures PDT, binds with calcium (Ca++) and phosphate ions, and results in precipitation in carious dentin, resulting in a compromised interface between CR and the CAD surface. 21
In addition, since the water content of CAD is high, it absorbs water due to its hydrophilic nature, worsening bond values. 37 Figure 3A with an SEM image of CR bonded to CAD treated with PDT shows gaps at the bonding interface due to sclerotic dentin and precipitation of the PS. Since CAD is incompletely demineralized, the hybrid layer formed is thinner and enriched with organic components, weakening adhesion of CR. 33 Similarly, CAD treated with the ECY laser before application of the adhesive decreases bond values.
Our findings of the existing study are in harmony with the work previously stated by Ceballos et al. and Cardoso et al.; the ECY laser treatment on CAD results in cross-linking of dentinal tubules, eliminating intrafibrillar spaces, and loss of cross bonding between collagen fiber networks, which are already demineralized. 38,39 It is noteworthy that although the diffusion penetration depth of the laser is better for disinfecting dentinal tubules, 40 laser irradiation results in microcracks on already chemically and morphologically compromised CAD surfaces.
Figure 2 displays the eroded dentin surface after ECY laser treatment. Similarly, Fig. 3C illustrates an image of CR bonded to ECY-treated CAD, showing gaps at the bonding interface due to lack of resin penetration and dentin sclerosis. The outcomes related to ECY laser treatment are diverse due to variable methodology, power, frequency, duration, beam spot size, and optical characteristics. 4,41 –43
The failure analysis confirmed that the CAD surface treated with the ECY laser and PS activated by PDT showed adhesive failure. The degree of water absorption correlates with adhesive failure patterns among CAD surfaces treated with PDT, 21,44 whereas thermomechanical ablation compromising the physical characteristics of affected dentin resulted in adhesive failure in CAD lased with ECY. 45
Due to the limitations of the present study, further in vivo and in vitro studies are mandatory to extrapolate the results of the current study. PDT of CAD using natural and synthetic PSs along with the use of the ECY laser at different power and frequency settings needs assessment and further probing. The microleakage score, dental sensitivity, fracture resistance, and other mechanical properties along with the tooth–composite restoration complex need further assessment.
Conclusions
The use of the ECY laser and PDT on CAD for cavity disinfection does not have potential for application in clinical settings as it decreases bond integrity of CR. Moreover, the ER pretreatment method for CAD and SD remains the gold standard.
Footnotes
Authors' Contributions
All authors have read and approved the final draft.
Acknowledgments
The authors extend their appreciation to the Deanship of Scientific Research at King Saud University for funding the work (through research group number: RGP-1438-028).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors extend their appreciation to the Deanship of Scientific Research at King Saud University for funding the work (through research group number: RGP-1438-028).