
Abstract
Objective:
The purpose of this study was to review the literatures regarding the treatment outcomes of applying laser to the infected sites in immediate implant placement. The review tended to primarily target a question: does applying high-power laser have any positive effect on infected sites in immediate implant placement?
Background:
Although immediate placement of dental implants has been referred to as a predictable and successful procedure, it is prone to the presence of infection that interferes with the healing process, and triggers the failure of implants.
Materials and methods:
A thorough electronic database search was conducted on PubMed/Medline, Embase, Web of Science, Google Scholar, and the Cochrane library in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. Two writers worked separately on screening the eligible studies, assessing whether there was a risk of bias, and extracting the required data.
Results:
Five out of the 60 studies nominated by the database search matched the inclusion criteria. The studies were carried out on a total of 192 patients with 296 implants in all. Ultimately, the study focused on 245 implants whose infected bed had been already decontaminated and prepared with the help of the high-intensity laser, used either alone or in combination with other approaches before implantation. With only nine failures, the implants inserted in infected and irradiated areas had a 96.3% overall survival rate.
Conclusions:
Taking the limitations of the review into account, the authors arrived at the conclusion that high-power laser irradiation can be beneficial for immediate implant placement in infected sites.
Introduction
Thanks to their high success/survival rates, dental implants are routinely deployed as a treatment modality to replace lost teeth. 1 According to Buser et al., 2 timing is an essence for the implant placement and is classed in three modes: (1) immediate placement (right away after tooth extraction), (2) early placement (4–8 weeks after extraction), and (3) late placement (6 months after extraction).
The concept of immediate implant placement was initially put forth by Schulte and Heimke. 3 Later on, in 1989, Lazzara 4 reported how immediate placement was applied to an extraction socket in humans. Immediate placement is a single-stage cost-effective surgical procedure with two benefits: (1) the treatment does not take as long as it does with multiple surgeries and (2) the patients are also more satisfied. 5,6 Countless authors have relied on the immediate implant placement as a procedure with high rates of predictability, success, and survival in the long run. 7 –9
Most compromised teeth, indicated for extraction, entail risks of developing both a local infection or inflammation and microbial interference with the healing process. As a result, the early/late modes of implant placement were conventionally preferred to the immediate mode to encourage the healing of soft and hard tissues and boost the resolution of infections. 10
Since infection has an adverse impact on implant osseointegration, leading to peri-implant diseases or implant failures, 11,12 some authors have taken the view that immediate implant placement ought to be preserved when there exist infections such as periodontal and periapical lesions. However, other investigations have reported that the implants placed immediately in the presence of periapical pathology with proper decontamination may result in almost the same complications and failure rates as those placed in a healed area. 5,13
It goes without saying that to perform any desirable immediate implant placement, clinicians must both decontaminate the soft/hard tissue aspects of infected sockets and remove the microbial debris. 14 However, it has been suggested that even after the most meticulous actions, the sockets may still host bacteria that vegetate in the extraction sockets, leading to retrograde peri-implantitis. 15,16 Accordingly, a number of treatment procedures have been proposed (i.e., systemic antibiotics, chlorhexidine mouth rinses, and the use of lasers) to ensure the best possible prognosis. 17,18
The first two procedures, however, suffer from major drawbacks: systemic antibiotics fail to achieve high gingival crevicular fluid concentration, 19 increase the risk of adverse drug reactions, 20 and require frequent selection of multiple antibiotic resistants. Similarly, chlorhexidine (CHX) leaves an unpleasant taste and stains the tongue, decreasing patients' compliance. 21
Recent years have witnessed a considerably upward trend in the use of lasers in dental implantology. Laser therapy has a comparative merit, the bactericidal effect on postoperative wound healing; lasers have the capacity to create a disinfected field during the surgical procedure, reducing the risk of infection. 22 Therefore, different lasers (e.g., erbium family) can play the role of disinfectants for extraction of sockets in immediate implant placement. 23
Nonetheless, as literature reports, the claims about the more efficient healing of high-power laser-treated sites have provoked controversies. Kusek suggested Er,Cr:YGG laser irradiation to decontaminate the infected sockets before implant insertion, and showed that the laser treatment reduced the anaerobic bacteria in number. 17 To the contrary, Birang et al. reported no complications in healing processes after immediate placement of implants into fresh extraction sockets with chronic periapical lesion either in presence or absence of erbium: yttrium-aluminum-garnet (Er:YAG) laser irradiation. 24
Accordingly, there remains a moot question as to whether the healing process of laser-treated sites is superior to that of the sites with no laser treatment. Thus, this systematic review was an attempt to critically inspect the literature concerning the efficacy of laser irradiation in infected sockets before immediate implant placement.
Methods and Materials
Protocol and registration
In this systematic review, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses criteria were adopted from the existing literature to enhance reproducibility and transparency. 25 Before the data extraction, the methodology was registered at the NIH International Prospective Register of Systematic Reviews, PROSPERO (CRD42021275409).
Focus question
The goal of this review was to provide a response to the following focus question. Does the use of high-power lasers have any beneficial effect on the infected sites in immediate implant placement?
The participant, intervention, comparison, and outcome question was constructed as follows: Participants: healthy adults (>18 years) with periapical infections Intervention: use of high-power lasers before implant placement Comparison: conventional implant placement Outcome: Implant survival.
Search strategy
A fully electronic database search was undertaken in PubMed/Medline, Embase, Web of Science, Google Scholar, and the Cochrane library to cover the research carried out until September 2022. Table 1 gives the search strategy for each database. This was followed by a manual review of the references in the collected publications to identify any additional research probably missed by the automatic search.
Electronic Search Strategy
Eligibility criteria
After removing the duplicate publications, two reviewers (P.R., N.S.) used the following eligibility criteria to separately review the titles and abstracts of the remaining studies.
Inclusion criteria: The review examined the randomized clinical trials, prospective studies, retrospective studies, and case series focusing on the use of high-power laser irradiation before implant placement; they had to be published in English and involve at least 10 patients.
Exclusion criteria: Animal studies, in vitro studies, reviews, the studies not employing a high-power laser and not published in English, and those with <10 patients.
Cohen's kappa coefficient was used to calculate the level of inter-reviewer agreement. In case of any disagreement, a senior investigator (R.F.) decided whether to include the article in the analysis or not. The selected articles underwent a quality evaluation and a full text review.
Quality assessment
The Joanna Briggs Institute (JBI) Critical Appraisal Checklists for randomized controlled trials, quasi-experimental research, and case-series 26,27 were deployed to assess the methodological quality of the investigations. Two authors worked independently to complete the appropriate JBI checklist for each investigation (P.R., N.S.). Each question on the JBI Critical Appraisal Checklist had to be answered with one of four choices: yes (Y), no (N), unclear (U), or not applicable (NA). The bias risk percentage was calculated using the quantity of “Y” selected in the checklist.
According to the rules of the JBI, the questions answered “NA” were ruled out from the calculations. The risk of bias was given three levels of high, moderate, and low (between 21% and 49%, between 50% and 70%, and >70% of “YES,” respectively). This review included the articles only with a low 28 or moderate risk of bias. 17,23,24,29
Data extraction
Once the two authors (P.R. and N.S.) had closely reviewed each publication, they used a structured extraction form to get the following information from the selected articles: the leading author, demographic information (the number of patients, number of implants, average age, smoking habits, presence of systemic illnesses, and implant area), reasons for extraction, method of extraction, decontamination process, implant properties (the area, insertion torque, loading duration, and graft usage), postoperative management, postoperative complications, laser characteristics (the type, mode, wavelength, power, irradiation period, and probe distance), outcome(s) (the success rate, survival rate, implant stability, bleeding index, marginal bone level, and pain present), and the duration of follow-up.
Results
The flow diagram in Fig. 1 demonstrates the process of how the studies were selected for this review. The database search helped to find a total of 60 studies. After the removal of 17 duplicates, the remaining 43 were chosen for the title and abstract screening with 13 qualifying for the full text examination. The remaining articles were submitted to a full text review, which resulted in the removal of eight research articles due to failure to meet the inclusion criteria.
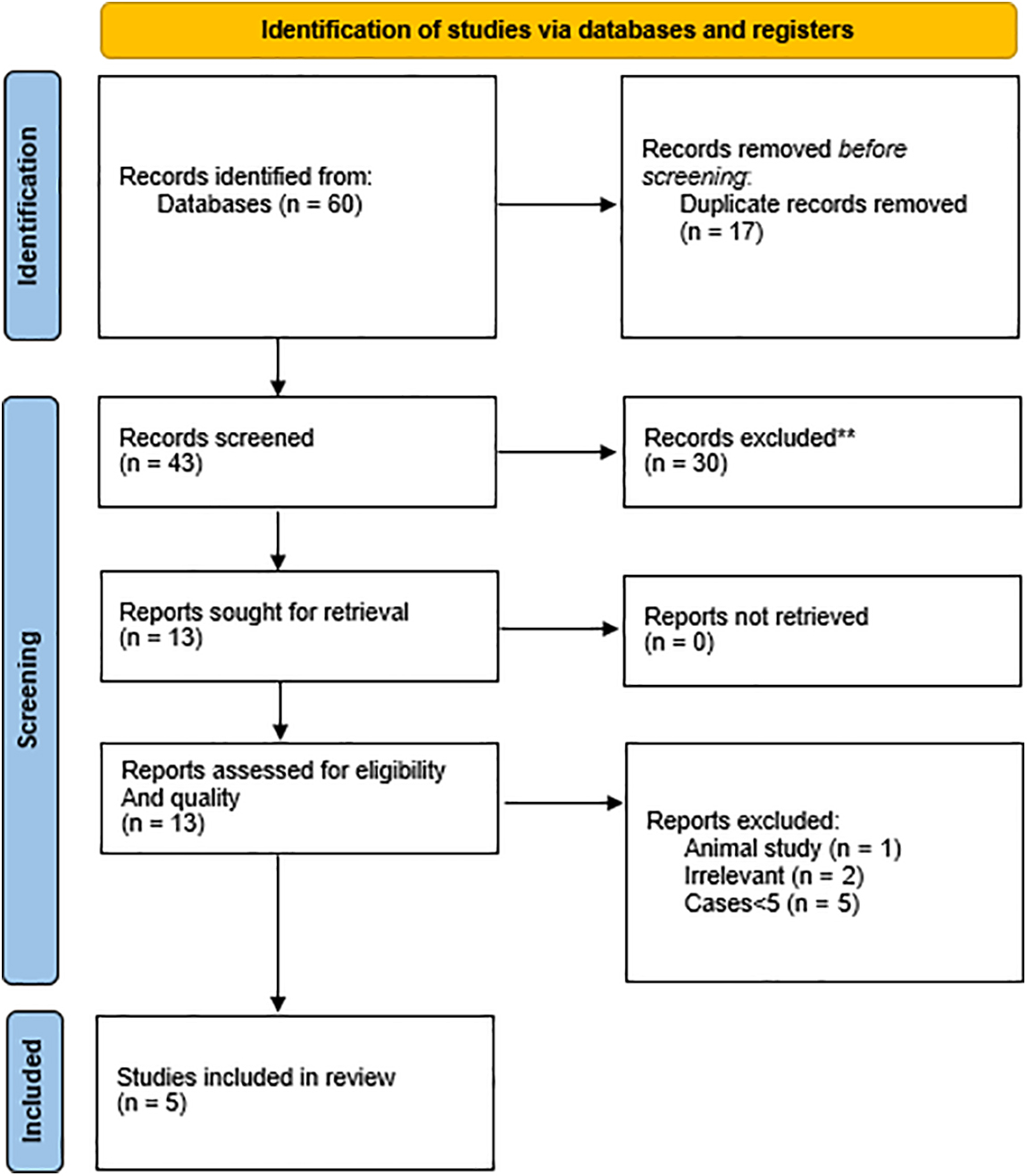
Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 flow diagram for systematic reviews.
The methodological quality of the remaining five studies was assessed using the relevant JBI checklist. Since four of the five studies had a moderate risk of bias and one had a low risk of bias, they were chosen for the qualitative analysis. Cohen's kappa value was = 0.71 for the reviewer agreement. According to the Landis and Koch's interpretation, this kappa coefficient indicates significant agreement. 30
Characteristics of the selected studies
Table 2 displays the demographic and methodological details of 3 case series, 1 randomized clinical trial, and 1 quasi-experimental research with a total of 192 patients (18–85 years of age) whose gender was not mostly reported. 31 –33 The review was carried out on 263 implants (out of 296 total implants) inserted in the infected sites, where the high-intensity lasers had been used either alone or in combination with other approaches to manage decontamination and preparation of the implant bed.
Methodological Information, Demographic Data of the Included Studies
CHX, chlorhexidine; Er,Cr:YSGG, erbium, chromium: yttrium-scandium-gallium-garnet; H2O2, hydrogen peroxide; IM, intramuscular; IV, intravenous; RCT, randomized clinical trial.
A pulsed erbium family laser [Er:YAG, 32 erbium, chromium: yttrium-scandium-gallium-garnet (Er,Cr:YSGG) 31,33 –35 ] with a power range of 0.5 watts 33,34 for decontamination to 2.5 watts 31 for implant bed preparation and a frequency range of 10 Hz 32 to 20 Hz 31,33,34 was employed in all of these studies. These lasers have been employed in a circular motion for 40–90 sec per socket. 31 –35
Table 3 displays all characteristics of the lasers utilized in all of the selected articles. The corresponding authors were contacted about some of the undefined parameters, but no responses were received. Prophylactic antibiotics were utilized in all of the included investigations; 31 –35 however, Crippa et al. only employed prophylactic antibiotics in 13 individuals with managed diabetes. 35 In all of the included trials, the infected sockets were debrided and decontaminated by utilizing a high-power laser in conjunction with some other methods such as socket curettage, 31 –33 0.2% chlorhexidine digluconate, and saline or hydrogen peroxide rinse. 31 –33
Lasers Characteristics
Er:YAG, erbium: yttrium-aluminum-garnet.
The root fracture, abscess, periodontal disease, endodontic lesion, and severely carious lesion were the most common reasons for extraction in the included studies. Most trials used a mucoperiosteal flap for extraction. Several brands of implants with varying properties, with or without grafts, were implanted with a torque of 35 N/cm33,35 or 25 N/cm. 32 Implant loading times varied among individuals, ranging from immediate loading to a 6-month delay after implant placement. Antibiotic medication was employed for postoperative care of patients in three of the examined trials. 31,32,35 Further, all of these studies but one 34 recommended using a chlorhexidine gluconate mouth rinse two times a day for at least 14 days after implant placement.
Assessment of outcomes
Various factors were evaluated throughout these five studies to target the effectiveness of laser irradiation in infected sockets on dental implants. Most of the included studies 32,33,35 employed the success criteria put forth by Albrektsson et al. 36 to assess the treatment outcomes. Based on the criteria, an implant is considered successful if no mobility is found during the clinical examinations after the 1st year; bone loss should be <0.2 mm per year; there should be no chronic pain, discomfort, or infection; and the attached gingiva must measure >2 mm in width.
However, the survival rate of the implants was chosen as the primary outcome of this review for two grounds: first, the studies did not enjoy a sufficient duration of follow-up. Second, the survival rate is the most generally reported success criteria in clinical reports. 37 Therefore, after obtaining permission from the authors, the survival rates (if not reported) were computed using failure rates.
In the included studies, a total of 210 patients received 296 immediate implants. Eight patients (16 implants) were subsequently lost to follow-up. Two implants were replaced due to the factory defects (although no problem with osseointegration had been observed in this group). Of the remaining 278 implants, 245 implants (with 9 failures) were placed in infected areas with the use of high-intensity lasers. The overall survival rate was 96.3%.
Other parameters (i.e., probing depth, plaque index, bleeding index, width of keratinized mucosa, or implant stability) were individually assessed by the authors. Birang et al. 32 found no significant differences between the test and control groups in their plaque index, bleeding index, width of keratinized mucosa, and probing depth from baseline to 6 months. Montoya-Salazar et al. 33 reported statistically similar plaque and bleeding indexes in the test and control groups at baseline and after 24 and 36 months of follow-up; however, the groups significantly differed in their plaque indexes and bleeding indexes after 12 months.
They also revealed that the significant differences in width of keratinized mucosa at the baseline and after 12 months did not exist 24 and 36 months later, and that neither group yielded significant changes in probing depth and marginal gingival level from the baseline to 36 months of follow-up. Detailed outcomes of each study are listed in Table 4.
Outcomes
CG, control group; PTV, periotest value; TG, test group; VNS, verbal numeric scale.
Three studies reported to have radiographic assessments. Birang et al. 32 and Crippa et al. 35 found no evidence of peri-implant radiolucency in their last checkups. In the study by Montoya-Salazar et al., 33 the test group had less marginal bone loss at 24 months of follow-up, whereas it was statistically similar at 3 years evaluation in both groups. Implant stability was only evaluated in the study by Birang et al. 32 using a periotest and was reported by periotest value at baseline and after 6 months and found no significant difference between both groups at any time. Crippa et al. 35 used verbal numeric scale to report postoperative pain (score <6 for 90% of patients) 1 week after the surgery.
Discussion
It is commonly accepted that the extraction of any infected tooth, debridement, and application of different modalities before implant placement is critically important to mitigate the inflammatory response, delay the bone resorption process, encourage osseointegration, and increase the implant success rate. 38 Among various modalities to control inflammation (e.g., antibiotics, chlorhexidine mouth rinses, and plasma-rich growth factors), lasers have been increasingly used as the disinfectant of extraction sockets in immediate implant placement. 39
Therefore, the goal of this systematic review was to scrutinize the published literature to examine how far this popular modality had been an efficient way of decontaminating the infected sockets in immediate implant placement and increasing the implant survival rate.
Different laser systems such as erbium family are available on the market for these kinds of procedures. The wavelength of erbium enjoys a high affinity with hydroxyapatite and water and desirably meets the requirements of both soft and hard tissue surgeries. 40 This can in return ablate or inactivate toxic substances such as bacterial endotoxins (lipopolysaccharide) that not only have a positive correlation with the wound healing of treated sites, but also outperform the conventional mechanical treatment plans in many aspects. 41
Er,Cr:YSGG and Er:YAG are the two most commonly used erbium lasers in dentistry. 42 Many studies have confirmed the high capacities of erbium family lasers to decontaminate and reduce anaerobic and pathogenic bacteria, minimize the risks of postoperative infections, and improve the healing process. 43 –45 In general, the former (Er,Cr:YSGG) is used to incise, excise, and ablate intraoral soft tissues and to remove hard tissues. 46,47 Four of the studies 17,23,28,29 used Er,Cr:YSGG (the wavelength of 2780 nm) mainly because it leaves the minimal thermal side effects and makes the minimal damage (if any) to the surrounding tissues. 48
First used in dental procedures by KaVo Key Laser (Kaltenbach and Voigt GmbH & Co., Biberach/Riss, Germany) in 1992, 42 Er:YAG laser (wavelength of 2940 nm) enjoys the highest absorption of water and is well absorbed by hydroxyapatite. It can ablate both soft and hard tissues with minimal thermal effects. 49,50 Takasaki et al. indicates that Er:YAG laser is capable of removing granulation tissue and deep decontamination of the intrabony defects. 51 Kreisler et al. 52 confirmed that Er:YAG laser-assisted decontamination of the infected areas is able to bring about results devoid of any considerable damage to the adjacent tissues.
Among the studies listed in our review, only did Birang et al. 24 apply Er:YAG laser to the infected sockets and found it to have an insignificant effect on achieving a high survival rate in immediate implant placement in extraction sockets with periapical lesions. However, their findings would not suffice to conclude that the Er:YAG laser irradiation was an ineffective method because there was a short-term follow-up (6 months) and probably an inadequate number of participants in this study.
There has been much research indicating the antimicrobial effect of photodynamic therapy in the treatment of infected sockets. 53,54 Although it is not in the scope of this study, it should be considered that photodynamic therapy could have the same potential effect as high-power lasers.
The studies in our review 17,23,24,28,29 calculated the survival rate in infected sockets (96.3%) in the presence of laser irradiation. There are two noteworthy points: first, to avoid any biased interpretations and overestimations, the terms “implant survival” and “implant success” must not be taken synonymously because the success rate (defined by Albrektsson criteria 55 ) is normally lower than the survival rate. “Implant survival” is referred to as the presence of an implant in the mouth independent of biological and/or technical complications. “Implant success” is commonly defined by Albrektsson criteria 55 that identify clinical evidence of successful osseointegration and survival of implants.
Kusek 17 and Kakar et al. 29 reported the survival rate, whereas Crippa et al. 23 and Montoya-Salazar et al. 28 reported the success rates. Birang study 24 interchangeably used “implant survival” based on Albrektsson criteria that should be considered as the success rate.
Second, conventionally evaluated based on Albrektsson, the implant success has been recently measured by new parameters namely health status, natural-looking peri-implant soft tissues, prosthodontic parameters, aesthetics, and patient satisfaction. 56,57 This can significantly decrease the overall success rate. Nonetheless, none of the included studies evaluated the recent criteria for success rate; therefore, it is recommended to take them into account for further investigations.
The popularity of the survival studies is likely to be related to their less challenging methodology, that is, to count the in-the-mouth remaining implants as the only statistical calculation. Whereas the analysis of success involves more complex parameters and criteria, and is directly associated with the health and quality of the implants. Therefore, for an accurate and thorough evaluation of the effectiveness of lasers in implant dentistry, studies are expected to report both survival and success rate.
Previous studies confirmed the bactericidal efficacy of laser devices in oral infections. 58,59 Although there are countless settings to perform, it is always important to obtain an ideal disinfection property, the average power, and precise timing of treatment. In fact, the higher is the average power, the more bacteria can be killed, but at the same time, any rise in average power would encourage longer treatment periods, causing a collateral damage to the tissue. A low-power setting would enable the clinicians to achieve a good effect with the tissue remaining intact; thus, it would be a must to find a balance between these factors.
In all of included studies, 17,23,24,28,29 the power of erbium lasers was in the range of 0.5–2.5 W and the irradiation time was in the range of 30–90 sec in the pulsed mood. As mentioned by Sindel et al., 60 the Er,Cr:YSGG laser (λ = 2780 nm) with 2.75 W power generates low levels of heat compared with diode lasers and may allow a safer surgery in the soft and bone tissues without any destructive effects by the rise in the temperature.
The Er,Cr:YSGG laser is a hydrokinetic system operating by photon liberation in an air–water spray, which triggers strong explosions in water droplets. 61 Within a confined space, the laser significantly reduced the concentration of bacteria. 62 Research has it that laser technology has a significant impact on areas of infected sites. 63 Effectively cleaving the molecules, hydroacoustic effects were found to be a highly efficient barrier to bacterial growth and denatures endotoxins. 62
Beside the photoacoustic effect, the erbium laser (like other wavelengths) has a bactericidal effect. 64,65 The erbium wavelength is absorbed by the water in the bacterial cells, undergoing the same liquid-to-steam vaporization that is seen during ablation of hard tissues. 66 That using lasers can destruct bacteria is an extra benefit to soft or hard tissue dental procedures.
The air–water integrated atomizer spray assists the removal of the tissues free of any considerable thermal damage. 67 Therefore, regulations of air–water spray are important. In both Kusek 17 and Montoya-Salazar et al. 28 studies, the water–air proportion was 7/14, whereas in Crippa et al. 23 and Kakar et al. 29 studies, it was 60/40 and 30%–40%/50–60%, respectively (almost the same). Birang et al. preferred not to mention the figures. 24 Clinicians must be cautious both to use adequate water spray with the laser and to constantly maintain the up and down pumping motions, as temperature can increase in the bone, potentially altering the osseointegration. 68 One key factor in this regard is how far the operator is familiar with this technique.
To our knowledge, this has been the first systematic review to assess the effectiveness of high-power lasers in infected sockets. Four out of five studies demonstrated that high-intensity lasers could be a reliable modality for socket disinfectant in immediate implant placement. However, the current systematic review has a number of limitations.
First, the studies were heterogeneous in terms of the variations in the study designs, different tooth sites for implant placement, extraction methods, implant systems, grafting the implant site, follow-up periods, characteristics of the lesions, and origin of the infections. Second, they suffered a nonuniform reporting of clinical parameters such as probing depth, bleeding and plaque indices, widths of keratinized mucosa, and implant stability. Third, they lacked randomized sampling, making it very complicated to compare the protocols with quite different selection criteria as there are numerous cases with extraction site risk factors such as presence of thin or absent buccal bone, making them less preferable for one protocol.
Fourth, the studies varied in the predictability of implant success in immediate placement; this was owing to a number of factors such as primary stability at the time of implant placement, implant positioning, socket anatomy, soft tissue morphology, tooth position, implant system used, and administration of antiseptic protocols that could change the results of immediate implant into an infected extraction socket. One major drawback that merits scrutiny is that the results of this review might be attenuated by the fact that antibiotics were prescribed in all included studies. That is to say, the results could not be associated merely with the use of lasers, and antibiotics might have interfered with the accuracy of the figures.
To address the concern, it is highly recommended to conduct a randomized clinical trial (RCT) study, comparing two groups of patients who receive laser irradiation: one in the absence and the other in the presence of antibiotics. Fifth, they mostly had short-midterm follow-up periods. Finally, the studies classified infection in vague and varied ways. Thus, clinical evaluations call for a clear classification system related to a more specific pathology.
In the future, well-designed studies (controlled clinical trial with strict inclusion criteria and a very large patient sample) with long-term follow-up are required to obtain more reliable results. In addition, it is necessary to provide far-fetched descriptions and examinations of extraction socket sites and to assess the success rate based on all aforementioned criteria.
In conclusion, although the systematic review was subject to a few limitations, high-power laser irradiation for immediate implant placement in infected sites can be beneficial. Further studies with more accurate designs would definitely shed light on the topic. It is highly recommended to control intervening factors so that the examination can go as meticulous as possible.
Footnotes
Authors' Contributions
H.K.G. contributed to investigation (equal), data curation (equal), and writing (equal)—original draft. N.S. was involved in investigation (equal), data curation (equal), and writing (equal)—review and editing (lead). P.R. was involved in investigation (supporting) and writing (equal)—review and editing (supporting). Y.K. carried out supervision and writing (equal)—review and editing (lead). R.F. was in charge of conceptualization, validation, supervision, and project administration.
Author Disclosure Statement
The authors have declared that there is no conflict of interest.
Funding Information
No funding was received for this article.