
Abstract
Objective:
This study was conducted to investigate whether the addition of photobiomodulation therapy (PBMT) to pelvic floor exercises (PFEs) is more effective in treating postpartum coccydynia compared with either modality alone.
Background:
Postpartum coccydynia is a widespread condition that significantly affects the quality of life. Inflammation as a response to childbirth trauma and weakening of the muscles and ligaments attached to the coccyx are presumed causes of postpartum coccydynia. Finding effective modalities to manage this condition will help the quality of life for most women.
Methods:
Sixty women aged 25–35 years with postpartum coccydynia ≥6 weeks were randomly allocated to Group A (PBMT + hot pack + PFEs), Group B (PBMT + hot pack), and Group C (placebo PBMT + hot pack + PFEs). All groups received 12 sessions over 4 weeks of hot packs plus their allocated active treatment (PBMT and/or PFEs). Outcomes were pain intensity (visual analog scale), lumbar flexion range of motion (ROM) (modified Schober test), and self-reported disability (Oswestry Disability Index). The assessors were blinded to group allocation.
Results:
All the measured outcomes showed significant differences (p < 0.001), with the superiority of Group A over the other groups (p < 0.001). Within groups, all groups showed statistically significant improvement from baseline across outcomes (p < 0.05).
Conclusions:
Adding PBMT to PFEs is recommended in the management of postpartum coccydynia as this combination resulted in greater reductions in pain and disability, along with improved lumbar flexion ROM.
Introduction
Gestation and childbirth are known as risk factors for reduction in the pelvic floor muscle (PFM) function. During delivery, the coccyx becomes hypermobile to facilitate childbirth, which predisposes it to injury and pain. Postpartum coccydynia is a painful tailbone condition that affects many women after childbirth due to inflammation as a response to childbirth trauma and the weakening of the muscles and ligaments attached to the coccyx. The incidence reported up to 86.5% in those with vaginal deliveries. This condition significantly impacts daily activities and quality of life. 1,2
Other risk factors for coccydynia may include the shape of the coccyx, body weight, type of delivery, ease of delivery, multiple parity, maternal age, shortness of perineum, and trauma to the levator ani, particularly the pubococcygeus. 3
Coccyx pain worsens with vertical pressure, prolonged sitting, leaning backward, or defecation. Unstable coccyx cases trigger pain when sitting or standing. Patients adjust their position to stretch their legs or lie on their sides, which can cause secondary issues such as sciatica, piriformis syndrome, and myofascial pain. These issues lead to pelvic floor dysfunction, worsening the primary pain. 1
In a previous study on the association of coccydynia with pelvic floor symptoms, pelvic examination of coccydynia patients revealed that muscles hypertonicity and spasm are more prevalent in coccydynia; however, a high percentage of examined patients had muscle weakness and endurance impartment. 4 Therefore, PFM strength and endurance impairments associated with coccydynia may need to be addressed in treatment considerations.
Different forms of manual interventions have been suggested for the management of coccydynia, such as gentle manual stretching, 5 joint mobilization, 6 coccyx manipulation, 7 biofeedback exercises, and pelvic floor exercises (PFEs). 1,8
Photobiomodulation therapy (PBMT) is an alternative nonsurgical intervention that demonstrates a reducing effect on pain and inflammation when applied at optimal doses. 9 It improves chronic musculoskeletal conditions, in part by enhancing mitochondrial energy production and microcirculation. PBMT also promotes tissue healing by affecting cell proliferation and inflammation. Laser stimulates cells to produce more adenosine triphosphate, which is the source of energy for cellular activities. Also minimizes proinflammatory cytokine production and increases anti-inflammatory mediator release. PBMT can help relieve coccydynia pain by modulating nerve transmission and reducing tissue damage in irradiated areas. 10
While some studies have demonstrated the individual benefits of nonsurgical interventions for the treatment of coccydynia, there is a lack of studies examining the effect of active exercise on the weak pelvic floor associated with childbirth as a primary cause of coccydynia. Moreover, there is limited research on the combined use of active exercise and PBMT as a treatment program, specifically for postpartum coccydynia. Combining PBMT with PFEs targets both the inflammatory and biomechanical components of coccydynia. PBMT is known for its anti-inflammatory and analgesic effects, while PFEs can restore PFM function, potentially stabilizing the coccyx. This dual approach may offer synergistic benefits not achievable by either modality alone. This study aimed to investigate whether adding PBMT to PFEs is more effective than PFEs alone in reducing pain, improving the lumbar range of motion (ROM), and enhancing daily function in women with postpartum coccydynia or not.
Methods
Study design
This prospective, randomized, controlled, double-blinded study was carried out from April to July 2023 at Cairo University’s Faculty of Physical Therapy Outpatient Clinic in Cairo, Egypt. Before each patient was assessed and enrolled in the trial, a thorough explanation of the study protocol was given, and an informed consent form was signed by all patients.
Participants
The study included 60 female patients with postpartum coccydynia who were diagnosed and referred for physical therapy by a specialist doctor based on physical and radiological examinations (X-ray or CT scan). 11 Their ages ranged from 25 to 35 years, with a BMI of less than 30 kg/m2. All participants were multiparous, having had 2–4 normal vaginal deliveries, and experienced postnatal coccydynia for more than 6 weeks. They also exhibited PFM weakness, as detected by the Oxford scale, scoring less than grade 3, while excluding cases primarily characterized by spasm and tightness. These selection criteria aimed to ensure a homogeneous sample with comparable levels of pelvic floor weakness, thus minimizing variability in baseline coccydynia severity. The age range of 25–35 years was selected because it represents a common age for childbearing, particularly in Egypt. This demographic is also at higher risk for postpartum pelvic floor disorders due to the cumulative effects of multiple vaginal deliveries. The exclusion criteria included genital prolapse, vascular conditions, rheumatoid arthritis, ankylosing spondylitis, skin infections in the treatment area, and bone deficits such as dislocation and partial dislocation of the coccyx.
Treatment interventions
The patients in this study were divided into three distinct groups. Group A was administered PBMT in combination with the local application of thermotherapy in the form of a hot pack in addition to PFEs, Group B received a hot pack then PBMT then a hot pack, while Group C was given a placebo of PBMT along with the hot pack and PFEs.
All interventions were delivered three times per week for 4 weeks and the duration of each session was about 50 min. PBMT was applied for 8–10 min, PFEs for 15–20 min, and hot pack for 20 min for every application.
PBMT application
A laser scanner applicator (SKW450-03/R2/AY) with a diversified power of 80 mW for 660 nm and 400 mW for 808 nm was used to deliver 12.7 J/cm2 to treated areas. Eye protection by laser glasses was provided for use by both the therapist and the patient (Table 1). 12 A physical therapist well-trained in the use of this laser device explained PBMT procedures and their effect on pain for each patient. Then, the patient was asked to lie prone, exposed the area to be treated, and adequately cleaned it with alcohol. The device was then switched on and adjusted to the size of the treated area. Accordingly, the device automatically calculated the treatment time depending on the size of the area to be treated. Subsequently, the therapist started the treatment, which took between 8 and 10 min to finish. After completion, the device was switched off automatically. For the placebo PBMT application in Group C, the same steps were performed, except that the therapist did not start the device after calculation of the area to be treated. The device was switched off and removed after the suggested time by the automatic calculation of the device (8–10 min).
Parameters of PBMT Used in this Study
PBMT, photobiomodulation therapy.
PFEs application
After explaining the anatomy and function of PFMs, also, the rationale of PFEs and their continuity to strengthen PFMs, the proper method of PFMs contraction was taught and practiced by an expert physical therapist. Patients were instructed to lie on their side, with their hips and knees flexed, while relaxing their abdominal and gluteal muscles and maintaining slow, natural breathing. 13 To learn how to exercise properly and be aware of the upward movement of the pelvic floor, after doing a glove, the patient placed her index on the anal opening and attempted to retract her digit while maintaining PFMs contraction, the so-called squeezing. Other muscle groups, including the gluteal and abdominal muscles, were encouraged to remain relaxed. The patient was then instructed to release tension in her PFMs and to allow them to return to their original state. Once the correct contraction was mastered, the patient was asked to contract as if she controlled her urethral orifice and bowel action, and then relaxed. The patient was asked to perform 10 maximal contractions voluntarily, each contraction maintained for 5 sec, with 10-sec rest intervals. These exercises were executed sequentially in three positions, side-lying, sitting, and standing. The session lasted for 15–20 min. 8
Hot pack application
All patients in the three groups received a hot pack application on the coccygeal region for 20 min during each session but Group B received it two times per each session. 14 The patient was asked to lie prone on the treatment table. The hot pack was then wrapped in a thin cotton towel and applied directly over the coccyx. Patients were monitored for discomfort and skin integrity every 5–10 min during the 20-min application, which allowed the transfer of therapeutic heat to the deeper musculature and joints in the coccygeal region.
Outcome measures
The outcome for all patients was the visual analog scale (VAS), which is a valid and reliable tool to determine the degree of pain. The modified Schober test (MST) for assessing the ROM of lumbar flexion and the Arabic version of the Oswestry Disability Index (ODI) for assessing disability level were also the outcomes of our study. All assessments were conducted before starting of the treatment and after 12 sessions of the treatment program.
Pain intensity
VAS was used to assess pain intensity. Patients were requested to mark on a 100-mL line the point that represented their severity of pain, with 0 being no pain and 100 being the maximum pain they have ever experienced. This is a valid and reliable tool to determine the degree of pain. 15
ROM for lumbar flexion
MST is a valid and reliable measure of lumbar flexion ROM. 16 The examiner palpated and marked the inferior edges of the posterior superior iliac spines and drew two horizontal lines, one 10 cm above and the other 5 cm below. Patients were asked to bend forward maximally until the onset of pain. Finally, the assessor measured the increase in distance between the superior and inferior lines. ROM of lumbar flexion was calculated from the difference in measurements between standing and maximum forward bending.
Functional disability
The Arabic version of ODI is a valid (r = 0.708) and reliable (ICC: 0.99) measure of functional disability. 17 It is a condition-specific self-reported questionnaire used to assess the functional disability level in patients with low back pain. It contains 10 sections covering common activities of daily living. Each section has six statements that describe the degree of disability for that activity ranging from 0 to 5. In this scale, 0 denotes “no disability,” while 5 signifies “maximum disability.” Patients selected the one statement in each section that best represents their current condition. If more than one statement was selected, the one with the highest score was recorded. For unanswered questions, the total maximum possible score was adjusted by subtracting five points for each unanswered section. The scores from all 10 sections were accumulated and then the total was divided by the adjusted maximum score possible and converted to a percentage to represent the patient’s overall disability level. The final ODI scores vary between 0% (absence of disability) and 100% (complete disability because of low back pain). 17
Sample size calculation
Considering the outcome measure of ODI score with an effect size of 0.53, based on data from a pilot statistical data analysis of the first 15 patients recruited. To determine the smallest sample size required to attain 95% statistical power and 5% alpha error, G*Power 3.1.9.2 software was used with the F-tests family, ANOVA statistical test, and fixed effect for three groups. Calculations indicated a total sample size of 60 patients, with 20 patients/group, would provide adequate power while minimizing unnecessary recruitment. This sample size balances scientific rigor with ethical concerns regarding excessive subject enrolment.
Randomization and blinding
After screening and obtaining informed consent, 60 patients were randomly divided into three parallel groups with a 1:1:1 allocation ratio: Group A (PBMT + hot packs + PFEs), Group B (hot packs + PBMT + hot packs), and Group C (placebo PBMT + hot packs + PFEs) using computer-generated blocked randomization. Group allocations were hidden within sequentially numbered, sealed, opaque envelopes, prepared by a statistician external to the study. Outcome assessors, data analysts, and patients were concealed to patients’ allocation. Primary (VAS pain scores) and secondary (MST spinal flexion and ODI scores) outcomes were measured at baseline and after 4 weeks of intervention by the same assessor. Statistical analyses were performed by a researcher blinded to group allocation using intention-to-treat principles.
Statistical analysis
Data statistical analysis for the study dependent variables was carried out by IBM SPSS Statistics version 26 (SPSS, Inc., Chicago, IL): VAS for pain, MST for lumbar flexion, and ODI for disability. After data cleaning, the Shapiro–Wilk test of normality showed that the VAS and MST data were not normally distributed, while the ODI data were normally distributed. Since data transformations did not significantly improve the normality of VAS and MST measures, nonparametric tests were employed. The Wilcoxon signed-rank test was used for within-group comparisons, while the Kruskal–Wallis test facilitated between-group comparisons for the non-normal VAS and MST data. Standard parametric tests—mixed design ANOVA for between-group analysis and within-group analysis—were used for normally distributed ODI data. For all statistical tests, the baseline alpha value for statistical significance was fixed at 0.05.
Results
Sixty female patients with a mean age of 30.1 ± 1.4 years were randomly allocated to Groups A, B, or C (n = 20 per group). All patients completed the 12-session study intervention with no dropouts. The flowchart diagram shows patient eligibility and the groups of patients (Fig. 1).
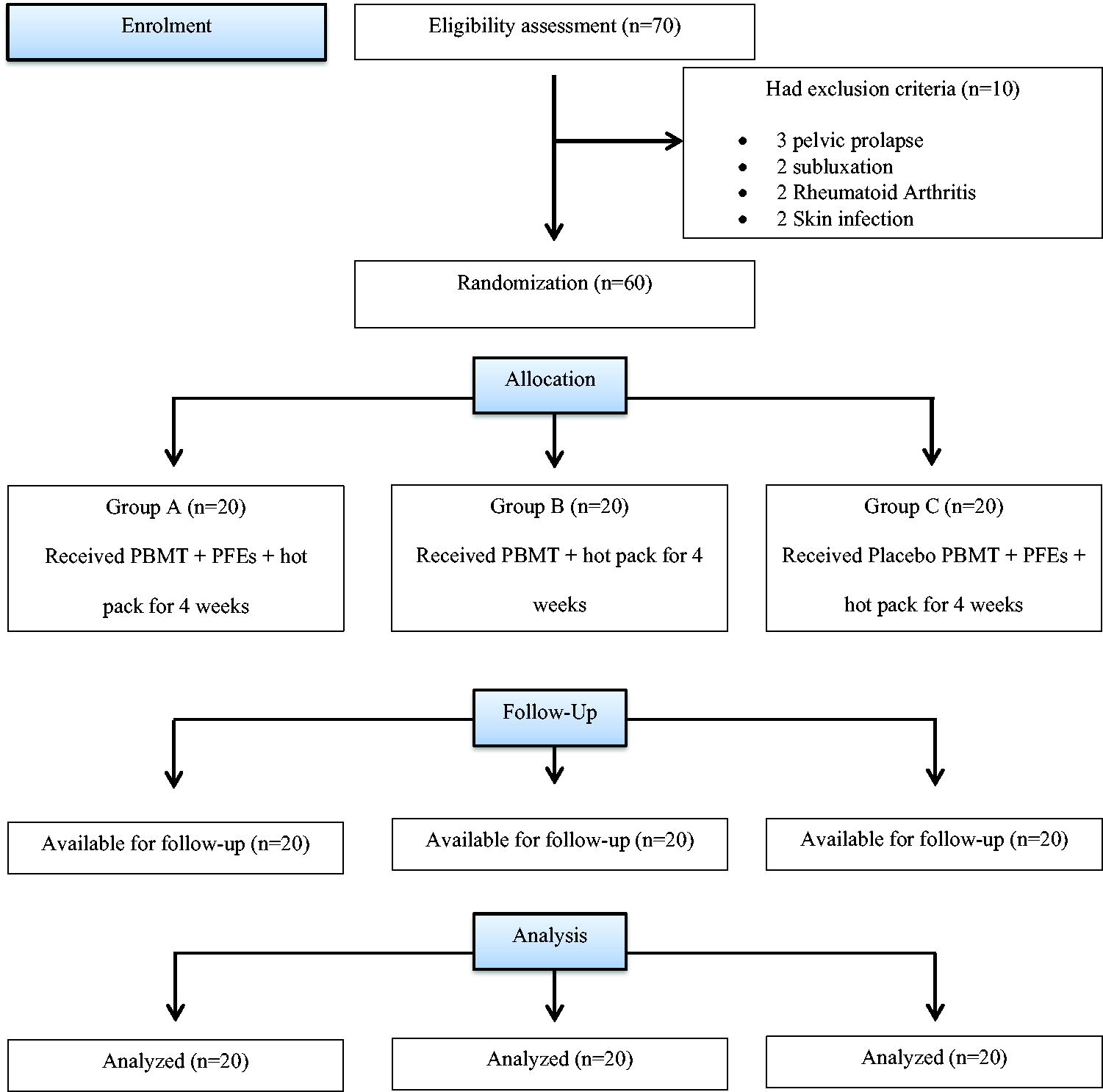
Flowchart of the study.
At baseline (before the intervention), there were no statistically significant differences between groups regarding patients’ general characteristics (age, weight, height, and BMI) with p values = 0.378, 0.692, 0.126, and 0.644, respectively. Also, there was no significant difference between groups regarding other outcome variables (VAS, MST, and ODI) at baseline with p values = 0.684, 0.457, and 0.225, respectively (Table 2).
Comparison Between Average Values of Outcome Measures Within and Between Study Groups Before and After Treatment
VAS, visual analog scale; MST, modified Schober test; ODI, Oswestry Disability Index; p value WG, within-group p value; p value BG, between-groups p value.
Within-group comparisons revealed statistically significant improvements in VAS and ODI scores, as well as a significant increase in MST values after treatment compared with baseline in the three groups (p < 0.05) (Table 2).
Moreover, after treatment comparison of all dependent variables showed significant statistical difference between the study groups (A, B, and C) (p < 0.001). To show the source of difference in VAS and MST after treatment, post hoc test (Wilcoxon signed rank test) was used and ODI (Bonferroni post hoc test) was used and revealed a significant difference between Group A versus both Group B (p < 0.001) and Group C (p < 0.001) in favor of Group A. No significant differences were found between Groups B and C for the measured variables, with p values of 0.313, 0.998, and 0.693, respectively (Table 3).
Post Hoc Test Between Study Groups After Treatment
Discussion
The current experiment aimed to determine the effect of combining the PBMT and PFEs on postpartum coccydynia. In our study post hoc test (Wilcoxon signed rank test) for VAS and MST and the Bonferroni post hoc test for ODI revealed a significant difference between Group A versus Group B and Group A versus Group C in favor of Group A. Group A demonstrated significantly greater improvement across all measured variables compared with Groups B and C.
The key finding of this study is that combining PBMT and PFEs resulted in significantly greater improvement in pain, lumbar ROM, and disability compared with using PBMT or PFEs alone for the treatment of postpartum coccydynia. This novel approach demonstrates the benefits of concurrently addressing both inflammatory processes and biomechanical factors that contribute to coccydynia. The reduction in VAS scores by an average of 6 cm in Group A represents a clinically meaningful improvement, corresponding to a significant decrease in pain perception. Similarly, the increase in MST by more than 4 cm reflects a functional enhancement that can substantially improve daily activities and mobility.
The marked reduction in self-reported pain levels with the combined protocol aligns with prior studies investigating the analgesic and anti-inflammatory effect of the PBMT on the coccyx and nearby structures. 12,18 Analgesic mechanisms underlying PBMT-mediated pain relief include suppressed production of inflammatory mediators, increased beta-endorphin levels, and reduced nerve sensitization. Also, it suppresses the nitric oxide synthase and microglial p-p38, which are proinflammatory cytokines, and increases release of natural pain-relieving substances such as β-endorphins, which centrally inhibit pain. 19
The pain-relieving effect of PFEs in coccydynia cases corresponds with findings from previous research, revealing a significant reduction in coccydynia-related pain. 1,8 In addition, properly performed PFEs provide mechanical stabilization of the coccyx through increased PFM strength and tone. 3 Moreover, PFEs can strengthen weak PFMs and assist the patient in adequately contracting PFMs, which would help in the biomechanical correction of the coccyx’ position. 20
The subsequent improvement in lumbar ROM and disability scores across all groups reinforces the close relationship between pain and physical function. This is consistent with prior evidence that pain reduction facilitates increased spinal mobility and ability to perform activities. 21,22
The vasodilation induced by the hot pack treatment in all groups enhances blood flow to the injury site, improving the supply of nutrients and oxygen. It also helps in eliminating pain-inducing substances produced during tissue damage. In addition, heat can influence the viscosity and density of connective tissues, positively impacting ROM and tissue extensibility. Further, recent findings suggest that localized, repeated heat therapy might promote angiogenesis and enhance muscular strength in addition to its effect on warming up before exercise. 23
Strengths and limitations
The current study used noninvasive interventions with no significant side effects. The inclusion of three study arms encompassing combination therapy as well as the two modalities individually enables analysis of potentially amplified effects with combined PBMT and PFEs. The use of blinded assessors enhances the reliability of the study’s findings, as it minimizes potential bias in outcome assessments. Finally, a predetermined sample size calculation helps ensure appropriate statistical power to detect meaningful differences between groups.
While these strengths contribute significantly to the study’s validity, some limitations need to be acknowledged. Psychological factors, lifestyle influences, and variations in postpartum recovery could potentially affect the results. In addition, the eligibility criteria, which restricted the sample to women aged 25–35 years with 2–4 vaginal deliveries, may limit the generalizability of the findings. While the short follow-up period allowed for the assessment of short-term effects, future research should investigate the long-term sustainability of improvements.
Conclusions
The combination of PBMT and PFEs led to greater reductions in pain and disability, as well as improved lumbar flexion ROM when compared with utilizing PBMT or PFEs individually. This synergistic treatment response likely stems from the simultaneous management of pain and musculoskeletal dysfunction, which are integral factors in post-childbirth coccygeal pathology. The findings of this study may be beneficial for the physical therapy practice in the treatment of multipara women with coccydynia due to pelvic floor weakness. Which will be a step toward an ideal physical therapy protocol for the treatment of those patients.
Footnotes
Authors’ Contributions
All authors conducted the idea, research design, data gathering, statistical analysis, and data interpretation. They collaborated to write, revise, and approve the final article before publication.
Ethical Approval and Consent to Participate
The study had ethical approval from the Cairo University’s Faculty of Physical Therapy Ethics Committee (P.T. REC/012/004253). In addition, it was prospectively registered with the Pan African Clinical Trials Registry (PACTR202305760876973). The study adhered to the Declaration of Helsinki’s guidelines for the ethical conduct of human studies. All patients received a thorough explanation of all study procedures before signing a written informed consent that acknowledged the security of their data and recognized the study’s nature, purpose, and the opportunity for them to withdraw from it at any point with no fear of implications.
Data Availability
The authors are ready to hand over raw data supporting this work’s findings upon request without unnecessary restrictions.
Author Disclosure Statement
There was no conflict of interest among the authors.
Funding Information
This work was supported by Princess Nourah bint Abdulrahman University Researchers’ Supporting Project number (PNURSP2025R117), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.