
Abstract
The impact of a hypertension awareness and educational program, BP DownShift, was evaluated among school bus drivers in a southern US state. At baseline (August 2007), blood pressure (BP) measurements, self-reported demographics, and hypertension awareness and management practices were collected from drivers who consented to participate in the study. Interventions included 4 educational mailings, installation of BP machines at all bus terminals, and access to free dietitian consultations and gym memberships. BP was evaluated using Department of Transportation guidelines. BP was remeasured and a survey was administered at follow-up (May 2008). At baseline, 208 drivers consented to the BP screening; 120 (58%) returned for a follow-up assessment. Most participants completing the study were female (73%) and African American (72%). Mean age was 50 years and mean body mass index was 32 kg/m2; 52% of participants were obese. In all, 58% of participants reported a prior diagnosis of hypertension by a physician, and 63% reported taking antihypertensive medication. Both systolic and diastolic BP (SBP and DBP) were lower at follow-up (135/82 mmHg vs. 145/87 mmHg at baseline; P < 0.001, both comparisons); 42% had a reduction in SBP > 10 mmHg, and 44% had a reduction in DBP > 5 mmHg. At follow-up, 58% were controlled to BP < 140/90, compared to 38% at baseline (P < 0.001). At follow-up, an increased proportion of previously diagnosed drivers reported home BP monitoring, healthy diet, and regular exercise as components of hypertension self-management. The implementation of our hypertension education, self-management, and awareness program was associated with an improvement in BP control, which may positively impact commercial driver's license recertification as well as improve employee health. (Population Health Management 2010;13:97–103)
Introduction
In the United States, the total estimated cost of high BP was $69.4 billion in 2008. 1 Employers are faced with substantial costs related to hypertension; across all employees, the overall economic burden of illness, including inpatient and outpatient services, prescription drugs, absenteeism, short-term disability expenditures, and productivity losses, has been estimated to be $392 per employee per year. 4 However, organizations that employ a significant number of commercial bus drivers may bear even greater hypertension-related costs, as research has suggested that bus drivers may be at an increased risk for hypertension as compared to other occupations. 5 –7 Because hypertension is asymptomatic, and elevated BP is associated with increased risk of an acute life-threatening event, such as a myocardial infarction or stroke, it poses a particular problem for bus drivers, as the occurrence of such an event while on the job could have serious consequences for passengers and/or other motorists. The US Department of Transportation (DOT) acknowledges that cardiovascular health should be an important focus for the commercial driver population 8 and, consequently, regulates commercial driver's licenses (CDLs) for employees with elevated BP. CDL employees with hypertension are permitted only a 1-year certificate for BP at DOT Stage 1 (systolic BP [SBP] 140–159 mmHg or diastolic BP [DBP] 90–99 mmHg), a 3-month certificate for Stage 2 (SBP 160–179 mmHg or DBP 100–109 mmHg), and immediate disqualification for Stage 3 (SBP ≥ 180 mmHg or DBP ≥ 110 mmHg). 9 Employer-sponsored educational programs that target hypertension management can be an effective strategy to reduce BP and improve recertification rates for CDL populations. 10
The primary objective of this study was to evaluate the impact of a hypertension educational initiative, the BP DownShift Program, on a CDL employee study population of school bus drivers with respect to BP control. Secondary objectives included the assessment of program participant awareness of hypertension management practices, understanding participating drivers' behavioral practices to manage their BP, and assessment of participant satisfaction with the BP DownShift Program.
Methods
BP DownShift is a hypertension education and awareness program designed specifically for CDL holders. The program provides free resources for distribution to study participants that include multiple BP educational mailings designed specifically for CDL holders containing the following: information about BP, appropriate BP goals, approaches to reducing modifiable risk factors, and BP guidelines that are part of CDL certification requirements; job-related information on ways to manage hypertension; options and tips to assist employees to measure and track their own BP; suggested strategies to achieve individual BP targets; and, finally, examples of other CDL holders' personal experiences with hypertension. Participants were also provided with information regarding use of the BP DownShift Web site to obtain additional information.
A BP screening was conducted in August 2007 for school bus drivers from a public school district in a southern US state who consented to participate in either the BP screening only, or both the BP screening and the BP DownShift Program. The school district employs 1191 CDL employees for student transportation; the majority of drivers are African American (85.0%) and female (69.4%). The screening was conducted at the bus drivers' annual mandatory meeting prior to the commencement of the school year, and all drivers who attended the meeting were encouraged and given the opportunity to participate, regardless of hypertensive status. BP measurements were performed according to American Heart Association recommendations, 11 and were obtained by medical personnel who were trained to perform BP measurements; driver self-reported age, height, weight, and racial/ethnic background were also obtained.
Drivers who also consented to participate in the study completed a brief, 11-item survey about hypertension knowledge, satisfaction with the presentation, and self-management behaviors. Subjects were asked whether a health care professional had ever told them that they have hypertension or high BP, if they had a household family member with hypertension, and for their evaluation of the BP DownShift educational presentation. Subjects were also asked to report BP self-management activities, including home BP monitoring and frequency, exercise, diet modification, regular physician visits, and oral antihypertensive medication use. Patient self-reported compliance with antihypertensive medication was assessed at follow-up (but not baseline) using the question, “How frequently do you take your medication as prescribed?” and assessed using multiple-choice, scaled responses ranging from “always” (7 days/week) to “never” (0 days/week).
The intervention phase began subsequent to study baseline, with an educational BP DownShift presentation and video testimonials from commercial drivers during the school district's annual bus drivers' meeting. Four hypertension educational mailings were sent to program participants via interoffice mail during the subsequent 6 months. In addition, to facilitate self-monitoring of BP, BP kiosks were installed at all bus terminal locations (Life Clinic Blood Pressure Monitors, Model LC-300-15); 12 however, these machines were not used for the BP measurements analyzed in our study. Free private dietitian consultations were made available to those who elected to participate, and free gym memberships were made available to all school district CDL employees.
A follow-up BP screening and survey were conducted during 2 weeks in May 2008 at all driver bus terminal locations. The follow-up survey contained items similar to those in the baseline survey regarding prior diagnosis of hypertension by a health care professional and reporting of BP self-management strategies. The follow-up survey also included a question about antihypertensive medication compliance for subjects who reported antihypertensive medication use, and assessment of changes to exercise habits since program participation. In addition, the follow-up survey contained items to measure the satisfaction with the interventional components of the BP DownShift Program and subjects' perceived impact of the program on their health status.
BP control was defined as <140/90 mmHg in accordance with DOT guidelines. BP was also analyzed according to DOT BP classifications (Table 1). Body mass index (BMI) was calculated based on self-reported height and weight as kg/m2, and was categorized as normal (BMI < 25 kg/m2), overweight (BMI 25–29 kg/m2), obese (BMI 30–39 kg/m2), and morbidly obese (BMI > 39 kg/m2).
Classification is performed based on the riskiest category, systolic BP or diastolic BP (ie, a measurement of 180/80 would be classified as Stage 3 based on elevated systolic BP).
Statistical methods
For categorical variables, screening and survey data were analyzed qualitatively using crude frequency statistics, and statistical comparisons were performed using the chi-square test. For continuous variables, such as SBP and DBP, age, and BMI, means, medians, and standard deviations were calculated, and statistical comparisons were performed using the t test and analysis of variance. Primary study outcome variables were related to changes in BP subsequent to the intervention; SBP and DBP at 6-months follow-up were compared to study baseline. SBP and DBP at baseline and at follow-up were compared using the paired t test. The proportion of patients with controlled BP at baseline versus follow-up was compared using McNemar's test. All study analyses were performed using SPSS version 16.0 (SPSS Inc., Chicago, IL).
Study protocol, survey, and informed consent forms were approved by an independent Institutional Review Board. Survey instruments and informed consent forms were made available in English and Spanish. Participating drivers received a small nonmonetary incentive (ie, an insulated lunch cooler) for the completion of both baseline and follow-up BP screenings and program surveys.
Results
At study baseline in August of 2007, 208 school district CDL employees had a baseline BP screening, representing 18% of the district's total CDL population; 66% (138) of these employees consented to the study and completed a baseline survey (Fig. 1). At follow-up subsequent to the BP Downshift interventions, 120 employees had a follow-up BP screening; 96 of these drivers also completed a follow-up survey. BP results for baseline were compared to follow-up results for the 120 drivers with both BP screenings (regardless of completion of the surveys).
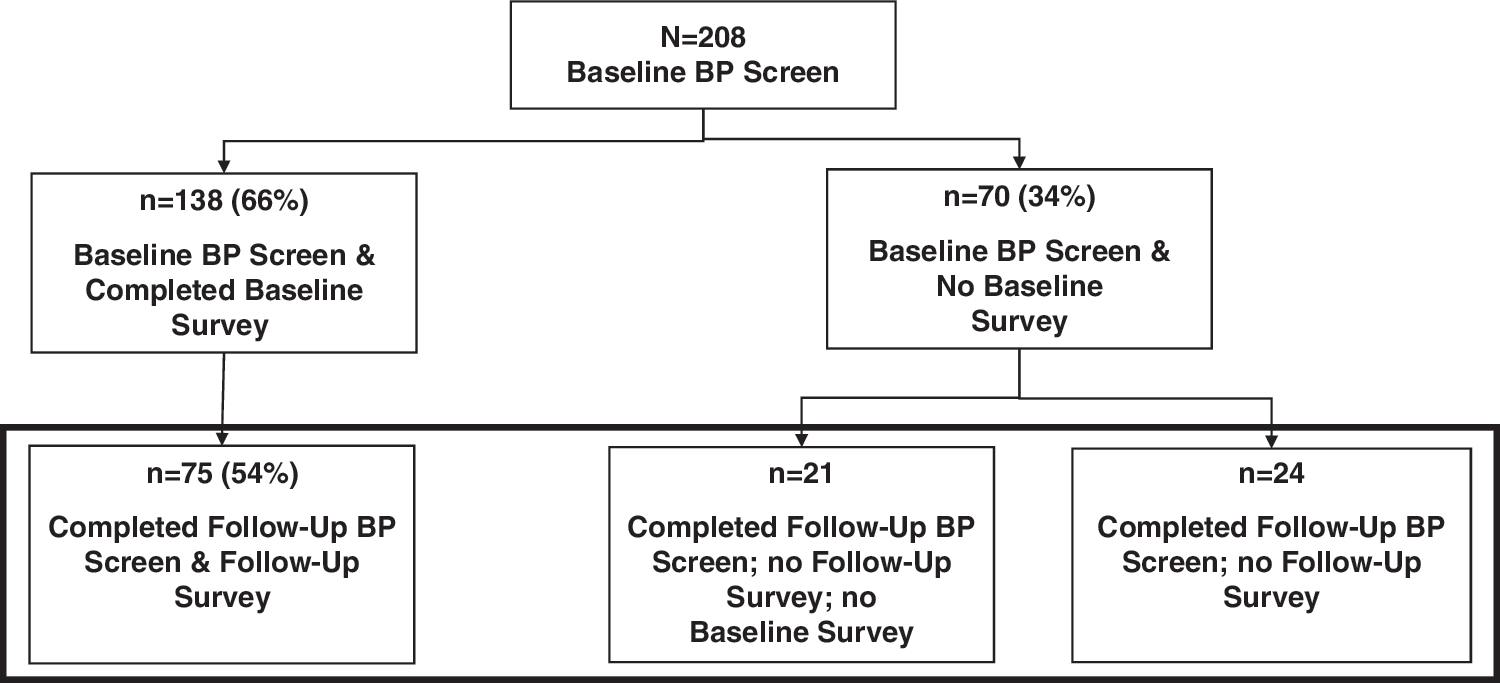
School district CDL employee BP DownShift Study, baseline, and follow-up population flowchart. At baseline (August 2007), 208 school district CDL employees participated in a BP screening. Subjects were also asked to complete a BP Downshift survey. At follow-up (May 2008), 120 of these drivers (75 who completed the survey + 45 without complete survey information) had BP measurements available for comparison to baseline. BP, blood pressure; CDL, commercial driver's license.
Study population demographic characteristics are depicted in Table 2. The baseline population of screened drivers (n = 208) were predominantly female (73%), and mean age was 49 years. The majority of the study baseline population was obese (61%); 13% were morbidly obese. More than 3 of every 4 study participants were African American, and slightly more than half (54%) reported a prior diagnosis of hypertension by a health care professional. Mean BP at study baseline was 144/86 mmHg; 40% of participants screened at baseline had BP controlled to <140/90 mmHg. Among participants who reported a prior hypertension diagnosis, 61% reported using antihypertensive medication. Study participants who received a baseline BP screening (n = 208) did not differ from those who also received a follow-up BP screening post intervention (n = 120) with respect to baseline BP, sex, age, BMI, race/ethnicity, prior hypertension diagnosis, or antihypertensive medication use (Table 2).
Among persons who participated in the baseline BP DownShift survey (n = 138) or the follow-up survey (n = 96).
Based on self-report among persons who indicated a prior physician diagnosis of hypertension (n = 75, baseline, and n = 56, follow-up).
Analysis of the survey instrument at baseline (n = 138) revealed that 3 in 4 (75%) rated their overall health status as excellent, very good, or good. Almost half (46%) of survey respondents indicated that they had at least 1 other family member in their household with hypertension. Among drivers who reported a prior diagnosis of hypertension (n = 75), 67% identified regular physician visits, 51% a healthy diet, 44% home BP monitoring, and 39% regular exercise as strategies used to control their BP. About 6 in 10 (61%) reported using oral antihypertensive medication, while 5% reported doing “nothing” to manage their BP. About 4 of 5 (83%) respondents rated the BP DownShift educational presentation at study baseline favorably (ie, excellent, very good, or good).
At follow-up, mean BP for the 120 drivers, subsequent to the BP DownShift intervention phase of the study, was 135/82 mmHg, a mean reduction 9/4 mmHg from baseline (P < 0.001 for SBP and DBP comparisons). Reductions in SBP and DBP from baseline are shown in Figure 2. Among the 120 participants with a baseline and follow-up BP screening, 42% had a reduction in SBP greater than 10 mmHg, while 44% had a DBP reduction greater than 5 mmHg. Figure 3 illustrates the comparison between baseline and follow-up BP according to DOT classification of hypertension stages, for all baseline and follow-up screened participants (n = 208 at baseline, n = 120 at follow-up) and for the subset of participants who reported a prior health care professional diagnosis of hypertension (n = 75 at baseline, n = 56 at follow-up). An increase in the proportion of subjects with normal BP was evident for all subjects and previously diagnosed subjects. At study baseline, 7% of all screened subjects, and 12% of previously diagnosed screened subjects, were classified as having Stage 3 hypertension according to DOT guidelines; at follow-up, no study participants were classified as having Stage 3 hypertension. Among participants who received both a baseline and follow-up BP screening regardless of prior diagnosis status (n = 120), 58% were controlled to BP < 140/90 at follow-up, compared to 38% at baseline (P < 0.001).
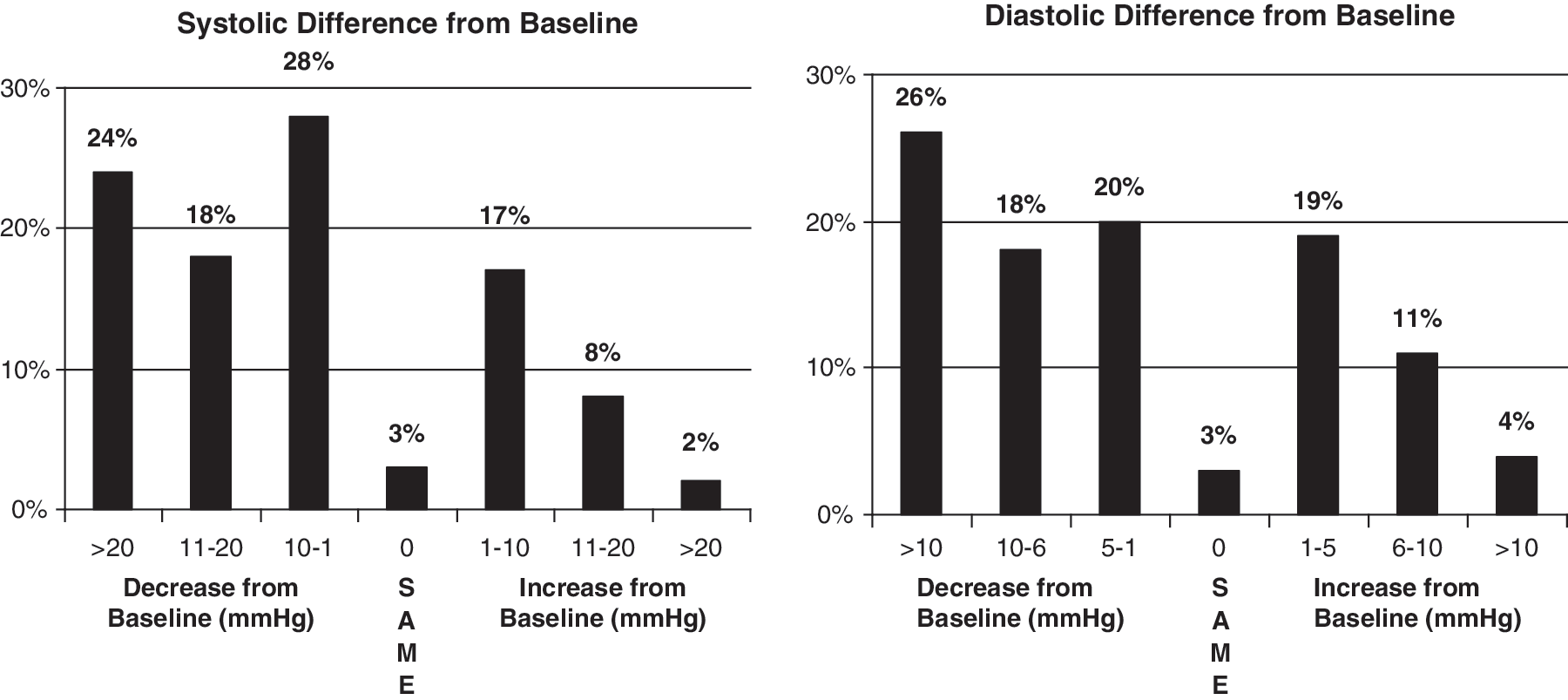
Difference in systolic and diastolic blood pressure (BP) among participants: baseline vs. follow-up (n = 120). Among drivers with BP measured at baseline and follow-up (n = 120), 42% had a reduction in systolic BP > 10 mmHg, while 44% had a diastolic BP reduction >5 mmHg.

Comparison of baseline and follow-up blood pressure (BP) for entire screened study population and subset with diagnosed hypertension. At follow-up, among both the entire BP screened population and those with a previous diagnosis of hypertension, increases in the percentage of subjects with “normal” 1 BP were evident, compared to study baseline. *HTN, hypertension; CDL, commercial driver's license.
Analysis of survey results revealed improvements in participants' health behaviors and personal health perceptions subsequent to the educational phase of the program. Comparison of results from baseline to follow-up revealed an improvement in overall self-reported health status. At baseline, 34% reported their overall health as excellent or very good, while 41% cited their health status as good. At study follow-up, 59% of participants reported health status as excellent or very good, while 34% responded that their health was good. Figure 4 illustrates the comparison of hypertension self-management behaviors at baseline and follow-up for drivers who reported a prior physician diagnosis of hypertension. Compared to baseline, a higher proportion of drivers reported performing home BP monitoring, regular exercise, and following a healthy diet as hypertension self-management behaviors. About 3 in 4 (77%) of survey respondents who exercise to control their BP said that they exercise more often since BP Downshift enrollment. Based on the follow-up survey, 93% of drivers indicated that they had made changes in their BP management based on the BP DownShift program, and 82% said that they suggested that a family member with hypertension make changes to their BP management strategy. Overall, participant satisfaction with the program was high: 97% of participants were satisfied with the quality of the program, 96% felt that the content of the educational material was easily understood, 94% felt that the materials were interesting and informative, and 89% believed that the number of educational mailings was satisfactory. Furthermore, 94% of participants indicated that they took their enrollment in the program seriously and believed that they participated fully in the program offerings.

Comparison of hypertension self-management behaviors among previously diagnosed hypertensive subjects: Baseline vs follow-up. As compared to study baseline, at follow-up more drivers reported performing home BP monitoring, regular exercise, and following a healthy diet to control BP. *Question was not included on the baseline survey. BP, blood pressure; CDL, commercial driver's license; MD, medical doctor.
At follow-up, medication compliance was evaluated for diagnosed hypertensive subjects who reported use of oral antihypertensive medication. Approximately 3 in 5 (58%) participants reported that they always take their BP medication as prescribed. An additional 19% reported “often” taking their medication as prescribed. However, approximately 1 of every 5 participants (21%) were less than compliant (“never,” “seldom,” or “sometimes” take prescribed medication) with their prescribed antihypertensive medication regimens.
Discussion
Our study, which measured the impact of an educational program, BP DownShift, among a largely female, African American bus driver population from a public school system in a southern US state, found significant improvements to participant health status. Both SBP and DBP were significantly lower at follow-up (135/82 mmHg vs. 145/87 mmHg at baseline). At a BP screening subsequent to the program intervention, 58% were controlled to BP < 140/90, compared to 38% at baseline (P < 0.001). Furthermore, an increase in self-reported hypertension health management strategies was evident among participants at study follow-up; more previously diagnosed drivers reported home BP monitoring, healthy diet, and regular exercise. Participants also rated the BP DownShift program favorably, as almost all (97%) participants reported a high level of program satisfaction, and 95% would recommend the BP DownShift program to a coworker.
At baseline, 54% of participating drivers reported a prior physician diagnosis of hypertension. The National Health and Nutrition Examination Survey (NHANES) 2003–2004 data have been used to estimate a current hypertension prevalence of 29.3% overall, and 34.4% for non-Hispanic blacks. 2 However, as the majority of our driver population were female and African American, these comparisons are difficult to interpret. NHANES data from 1999–2002 have been used to estimate the prevalence of hypertension in non-Hispanic black women at 42.6%. 13 Being employed as a commercial bus driver may also be a risk factor for hypertension. One study conducted among transit vehicle operators of the San Francisco Municipal Railway, and a control group of individuals newly hired but not yet working as operators, found that hypertension prevalence, adjusted for age, race, and sex, steadily increased from 28.8% in the group with no exposure to 38.9% among drivers with more than 20 years of service. 14 Only 25% of our baseline study population with a prior diagnosis of hypertension had BP controlled to <140/90 mmHg; these figures are slightly lower than US normative data, which indicate that in 2003–2004, 33% of all hypertensive persons, and 29% of non-Hispanic blacks, had controlled BP. 2 However, subsequent to the BP DownShift program, 57% of these participants had BP controlled to <140/90 mmHg, a proportion that compares favorably to US normative data for both blacks and nonblacks. Obesity rates in our study were considerably higher as compared to US normative data. In the current study, 61% of participants screened at baseline were obese, compared to 41% of US hypertensive adults in 2003–2004, 2 32% of all adults regardless of hypertensive status, 15 and 51% of all adult non-Hispanic black women. 15 The positive impact of the BP DownShift program suggested by the current study is particularly noteworthy given that this population, which is largely African American, female, and obese, has historically been at an increased risk of high BP.
Many employers are taking a proactive role in implementing such programs to improve the health of their employees. A number of published studies have documented the benefits of health education and disease management programs across many different chronic disease states. A comprehensive meta-analysis of disease management programs across 11 chronic conditions demonstrated improvement in patient satisfaction, medication adherence, and markers of disease control. 16 The BP DownShift approach has been used in other employer transit settings with demonstrated improvements in participant health status. Harshman et al 10 studied 501 randomly-selected CDL employees of a utility company in the southeastern US, and demonstrated a significant reduction in the proportion with uncontrolled hypertension subsequent to the educational program (from 26% to 17%).
Although our study provides important information regarding the positive effects of an educational program on BP control in a CDL employee population, some limitations are important to consider when interpreting our study's findings. The sample size for this study was relatively small, and participants were not randomized to participation. Thus, generalizability of results to the entire bus driver population of the participating school district is difficult, as study participants may not have been representative of the larger population as a whole. It is possible that drivers who were concerned about their BP were more likely to participate; this could have led to selection bias and a potential overestimation of baseline hypertension prevalence, as well as an overestimation of poor BP control rates in the overall district school bus driver population. This would also partially explain the discrepancy between the baseline hypertension prevalence found in our study and comparisons to normative data. Because the baseline BP screening occurred subsequent to the annual summer recess, participants may have been less likely to be compliant with prescribed antihypertensive medication prior to the screening than during the school year. Some study information was collected via subject self-report, including height and weight (BMI), age, prior diagnosis of hypertension, and self-management behaviors. Information regarding participant antihypertensive medication compliance was not obtained at study baseline. While self-reported antihypertensive medication compliance was assessed at follow-up, we did not have an objective source of compliance information. We did not have information regarding whether study participants may also have had diabetes; more aggressive BP targets may be important to consider for persons with diabetes, in accordance with recommendations from national guidelines for diabetic hypertensive persons. 3 As the employer did not wish to withhold from nonparticipants some of the self-management resources (ie, access to BP kiosks for self-measurement, free gym memberships) available to participants, a study design that employed a control group was not used, and frequency of self-monitoring of BP using the installed kiosks was not recorded. Thus, it is difficult to ascertain which components of the program were the most important to the overall intervention. Nevertheless, while taking these important caveats into account, our study provides evidence that a simple, multifaceted, employer-based intervention focusing on hypertension education, self-management, and awareness can produce health benefits and lead to positive changes in health behavior in a high-risk population.
Conclusion
Our study demonstrates reductions in BP subsequent to the implementation of a multifaceted hypertension management program in a CDL employee population. Subsequent to implementation of the BP DownShift program, participants experienced a reduction in BP and an improvement in hypertension self-management health behaviors. In addition, participating drivers expressed a high level of satisfaction with the components of the educational program. Further research is warranted using controlled studies to evaluate the impact of hypertension management programs in CDL populations. Hypertension management programs, such as the one described in this paper, may benefit other employers with CDL drivers by improving driver health, reducing the number of commercial drivers potentially facing medical disqualification, and improving safety not only for participating drivers, but also potentially for their passengers and other motorists.
Footnotes
Acknowledgments
This study was funded by Novartis Pharmaceuticals Corporation, the manufacturer of several drugs indicated for the treatment of hypertension.
Author Disclosure Statement
Mr. Doyle and Ms. Frech–Tamas are employees of Novartis Pharmaceuticals Corporation, and both own stock and stock options in Novartis. Ms. Wogen's organization, MedMentis Consulting, received financial compensation from Novartis for assistance with the conduct of the study and preparation of the manuscript. Ms. Severance–Fonte and Ms. Morandi–Matricaria have no potential conflicts of interest to disclose.