
Abstract
The 2000 United States Public Health Service (USPHS) clinical practice guideline, “Treating Tobacco Use and Dependence,” recommends systems interventions to integrate the treatment of tobacco into routine health care. The Tobacco Control Initiative employed a systems approach to integrate evidence-based treatment for tobacco use into patient care practices in Louisiana's safety net health care system. The purpose of this study was to assess changes in awareness and implementation of the USPHS clinical practice guideline. Surveys were administered to a purposive sample of hospital personnel from key departments in the Louisiana State University system of public hospitals in 2003 (n = 24) and 2007 (n = 44). Perceptions of implementation success improved for 50 of 59 distinct survey items. Rasch scaling was used to assess overall (scaled) change and showed substantial improvement from 2003 to 2007 (P < 0.001). Survey items also were grouped into 6 logical key concept sets. Improvement occurred in perceptions for all 6 key concepts; however, not uniformly. Results of the 2003 and 2007 surveys illustrate the potential effectiveness of using a systems approach to integrate the assessment and treatment of tobacco use into routine care practices in a public health care delivery system that serves medically vulnerable populations. (Population Health Management 2011;14:79–85)
Introduction
Health care delivery systems have the capacity to reach large populations of smokers. 6 Recognizing the potential to increase tobacco cessation, the 2000 United States Public Health Service (USPHS) Clinical Practice Guideline, “Treating Tobacco Use and Dependence,” recommended strategies to facilitate integration of cessation services into health care systems. 6 The strategies focused on system-level changes to ensure identification and treatment of tobacco users during clinical encounters. 6 In 2002, the Louisiana State Legislature enacted a tobacco excise tax, dedicating a portion to the establishment of a comprehensive tobacco control program and mandating the provision of cessation services in the state's public hospital system. 7
Louisiana's public hospital system in 2002 was the 5th largest “safety net” health care delivery system in the nation, serving over 1.2 million Louisiana residents, 8 with smoking prevalence estimated to be similar to that observed in other low-income populations such as Medicaid recipients (∼ 36%). 9 This integrated state-run health care network comprises 10 facilities located in population centers across the state and operated by the Louisiana State University (LSU) System. Every resident of the state is entitled to receive care in any facility. Many of the state's most medically vulnerable are served; 49% of patients are uninsured, and eligible for free care, while the remainder are covered by Medicaid (26%), Medicare (7%), self-pay (14%), commercial insurance (5%), or third-party liability (3%) (LSU finance department, written communication, August, 2009). Hospitals in the Louisiana system record a 25:1 ratio of outpatient to inpatient visits, and the emergency departments and 350 primary care and specialty clinics provide approximately 2 million clinic visits annually. 10 Seventy-seven percent of patients in the network are nonwhite; 52% are female (LSU finance department, written communication, August, 2009). The Tobacco Control Initiative (TCI) was established to provide cessation services in Louisiana's public hospital system. The mission of TCI is to integrate evidence-based treatment for tobacco use into patient care practices using the system interventions recommended in the 2000 USPHS Clinical Practice Guideline. The interventions include implementing a tobacco user identification system; providing training, resources, and feedback to providers; dedicating staff to provide treatment of tobacco use; promoting hospital policies that support treatment of tobacco use; and reducing patients' out-of-pocket costs for evidence-based treatments (eg, counseling and medication). 6 These organizational strategies were paired with a clearly delineated clinical practice protocol that included 5 major steps—the 5 A's (ie, Ask, Advise, Assess, Assist, Arrange)—to intervene with tobacco users. 6
By combining the resources provided through TCI with the public hospital systems' Medication Assistance Program, all patients have access to standardized evidence-based cessation services including low- or no-cost medications (eg, nicotine replacement therapy patches, bupropion, and varenicline), free on-site group behavioral counseling, facilitated access to free telephone counseling via the state Quit Line, individual bedside consultation for hospitalized smokers, and instructional self-help materials at all clinic visits. TCI also provides education and training to ensure clinicians have the skills to intervene with smokers, and TCI facilitates adoption of systemwide policies to support and encourage treatment of tobacco users.
In 2003 and 2007, TCI conducted surveys to assess awareness and implementation of the USPHS (2000) clinical practice guideline “Treating Tobacco Use and Dependence.” It was expected that, if implementation was successful, in 2007 providers and administrators at participating facilities would have greater awareness of the USPHS clinical practice guideline, as well as more positive perceptions regarding implementation of the guideline, than they had in 2003.
The purpose of this article is to present the results of both surveys and discuss changes in tobacco control policies and practices observed over the first 4 years of the systemwide implementation.
Methods
The 2003 and 2007 surveys were adapted from a series of surveys conducted by the American Association of Health Plans (AAHP). 11,12 The AAHP instrument was the most comprehensive and widely used assessment of tobacco-related interventions in health care systems. The 2003 and 2007 surveys consisted of 35 items, 23 of which were identical. All necessary human subject protections were employed and, consistent with exempt status research, this study received approval from appropriate system administrators.
Survey implementation
In order to obtain a broad view of clinician awareness and implementation of the USPHS (2000) guideline, it was determined in conjunction with system administrators that respondents should represent the functional units of a facility (ie, administration, inpatient, outpatient, quality assurance). The 2003 survey was mailed to 1 informant per department at each facility. In 2007, the survey was mailed to 3 different informants per department at each facility in an effort to obtain input from all departments. E-mail and telephone follow-up was conducted 2 and 4 weeks after the return due dates.
Given the nonprobability sampling design of the study, descriptive statistics are reported. These include changes from 2003 to 2007 for each survey item, as well as aggregate change within 6 key concept item groupings. Rasch analysis 13 was used to assess the magnitude of change from 2003 to 2007 survey administrations.
Results
Eight of the 10 facilities (80%) in the LSU Hospital System participated in the study. In 2003 a total of 24 surveys were received (75% response rate) representing 3 of 4 departments: hospital administration (hospital administrator, assistant nursing director), outpatient clinics (family practice, pediatrics, ob/gyn), and inpatient units (nurse supervisors). In 2007, a total of 44 surveys were received (46% response rate). All 4 departments were represented: hospital administration (medical directors, hospital administrators, nursing directors, employee health directors), quality assurance (managers, compliance officers), and inpatient and outpatient areas (RN supervisors and managers).
The survey items resolve into 59 unique binary items that were asked on both surveys. Table 1 displays the 2003 and 2007 results for those items.
NRT, nicotine replacement therapy; US DHHS, United States Department of Health and Human Services.
The items in the table are grouped by key concept rather than by survey order. Most items were asked in such a way that positive responses correspond to improved implementation of cessation programs. Those items for which negative responses correspond to improved implementation were reversed for all analyses described here, and the wording of those items in Table 1 was reversed as well. Figure 1 presents the Table 1 results graphically.
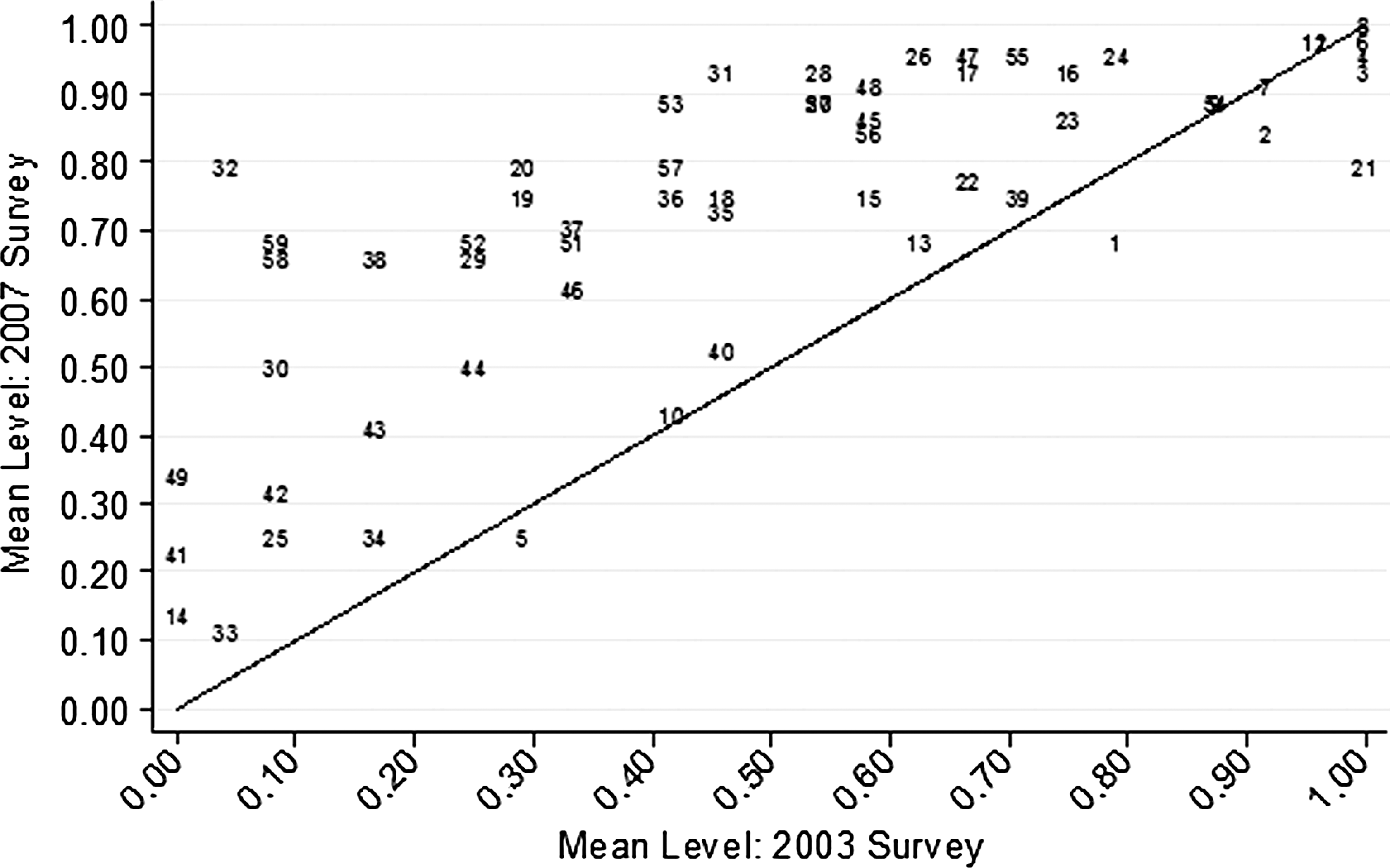
Mean levels of survey items. 2003 survey vs 2007 survey.
In Figure 1, the diagonal line represents equal response levels in 2003 and 2007, so that items showing little change from 2003 to 2007 will lie near the diagonal. The area above the diagonal represents positive change from 2003 to 2007 (ie, improved perceptions regarding implementation success). In the upper right corner of Figure 1 is a collection of items on which the sites scored very high on both the 2003 and 2007 surveys. These items are largely a collection of potential barriers to implementation, and the high scores for these on both 2003 and 2007 surveys imply that sites did not perceive these barriers to exist either in 2003 or 2007. In particular, sites perceived no barriers due to lack of organized cessation services (Item 6), perceived validity problems with guidelines (Item 8), or provider requirements for other patient care (Item 3). However, sites clearly perceive that some barriers exist. Items 5 and 10 also assessed perceptions regarding barriers, and scores for items 5 and 10 are both low and show little change from 2003 to 2007. Sites perceived neither resource barriers to tobacco control program implementation (Item 5) nor system barriers to program implementation (Item 10). Overall, among the item categories, the set of “barriers” items showed the least change from 2003 to 2007.
At the bottom left of Figure 1 are those items for which scores were low in both 2003 and 2007, although perhaps showing modest improvement over time. Among these items are: site has computerized reminders to encourage providers to remind patients to quit (Item 33), no limitation due to how often the intervention may be offered (Item 14), site uses incentives for providers and staff to implement cessation activities (Item 41), face-to-face cessation counseling is available to patients (Item 25), and site has patient incentives for adherence to cessation treatment (Item 34).
Figure 2 compares the 2003 to 2007 mean response by item category. Those results show perceptions of implementation success improved in all item categories, although less so in the “barriers” category as noted earlier. By contrast, improvement was very strong on items assessing awareness of tobacco cessation treatment guidelines.

Mean level by item group. 2003 survey vs 2007 survey.
Random effects Rasch analysis 13 was also used to scale the items (after discarding several items that did not appear to satisfy the unidimensional assumption of Rasch analysis.) This was done primarily to facilitate an overall statistical comparison of 2003 and 2007 responses. A t test was used to compare the 2003 and 2007 scaled responses, and found the difference between 2003 and 2007 aggregate scaled responses to be statistically significant (P < 0.001). Indeed, on the Rasch analysis-derived latent factor, the aggregate 2007 response was over 2 standard deviations higher than the aggregate 2003 response. Responses from 2003 and 2007 were compared by item category and by site using the Rasch-derived latent factor scores. The results (not shown) are similar to those shown in Figure 2.
Implementation of the clinical practice guideline is also reflected in process measures reported quarterly. Each quarter's measurements were calculated using the cohort of unique smokers who visited Health Care Services Division (HCSD) clinics during the quarter. Calculations were based on referred patients only. For the fiscal year ending June 30, 2007, 81,828 unique individuals were identified as smokers among LSU HCSD facilities (both inpatient and outpatient); these individuals represent approximately 30% of the LSU HCSD adult patient population. A majority (65%) of the identified tobacco users was uninsured, 59% were female, and 85% were younger than 50 years of age. A total of 14,729 of this cohort of 81,828 tobacco users were referred to the TCI program for cessation services, an 18% referral rate (largely from providers in outpatient clinics). Eighteen percent of the referred patients were given a prescription for cessation medications; 5% attended at least 1 group behavioral counseling class; and TCI staff conducted 297 bedside consultations for hospitalized smokers. Seven percent of the patients who attended at least 1 group class reported quitting, while 58% reported quitting or significantly reducing their tobacco use at 1 year follow-up.
Discussion
Results of the surveys indicate that respondents perceived both progress in and barriers to integrating evidence-based cessation services. Overall, respondents reported consistent positive improvements in awareness and implementation of the guideline, practices and policies regarding tobacco control, and identification and monitoring of tobacco use among patients. Activities related to the 5 A's approach were also reported to have increased substantially. The USPHS guideline endorses creating a supportive environment that facilitates treatment of tobacco users. 6,14 Consistent with this recommendation, results showed all facilities developed written policies for treating tobacco use and that treatment of tobacco use had become a higher priority for facility medical directors.
The use of electronic systems to identify tobacco users and document smoking status increases provider intervention with patients who use tobacco. 6,14 The dramatic improvement in electronic identification and documentation of tobacco use observed at follow-up can be attributed to the establishment of an electronic “Tobacco Registry” created from patient certification processes (to determine financial class), which occur every 180 days. The registry was developed as a component of TCI to identify smokers for analytical and evaluation purposes.
Respondents also noted changes in tobacco control practices and policies at the provider level. These changes may be attributed to several factors. Starting in 2005, TCI hired and trained 1 tobacco specialist for each facility to coordinate and deliver standardized evidence-based cessation services. By 2007, cessation coordinators, along with a clinician “tobacco champion” at each facility, made a uniform presentation to in-service providers and staff on the prevalence of tobacco use among facility patients, the benefits of cessation, the availability of evidence-based cessation services, and the procedure for referring patients for treatment. Additionally, treatment of tobacco use was the focus of a spring 2007 systemwide quarterly health care effectiveness meeting that demonstrated the administration's support for making tobacco cessation a priority. The meeting was highlighted by the adoption of a systemwide policy to treat tobacco use and dependence in inpatient and outpatient care. Finally, the state's comprehensive tobacco control program conducted a series of external media campaigns promoting prevention and cessation of tobacco use. Additional resources, administrative endorsement, and public sentiment may have synergistically impacted the adoption of tobacco-related policies and practices in the hospital system.
The slight increase in respondents citing lack of staff and requirements for other patient care as barriers to implementation may be an unintended consequence of TCI. With the advent of the program several things may have contributed to an increase in perceived barriers: (1) as noted, TCI staff consistently in-serviced clinic providers and staff on the importance of and methods for intervening with tobacco users; (2) treatment of tobacco use was integrated into the systemwide disease management program as a modifiable risk factor for chronic illnesses and viewed as a crosscutting initiative; 15 and (3) tobacco-related performance measures were displayed for each hospital on the systemwide Web-based Disease Management Statistics Report System, making providers accountable for clinical intervention. As a result, there was increased demand for assessment of tobacco use, smokers' readiness to quit, and subsequent referral for treatment using a paper referral form (ie, application of the 5 A's). The ideal panacea for these barriers, an electronic health information system, was under development in 2007 and not fully operational to document tobacco-related intervention. TCI management team worked with the LSU system information technology group to design tobacco-specific items for inclusion in its evolving Clinical Inquiry (CliQ) system. 15 It is expected that the number of staff and the time required to document the use of the 5 A's approach will be substantially reduced as CliQ use expands.
Among the limitations of the study are the varied response rates within and among facilities. Response bias thus stands as a distinct possibility. Efforts were made to achieve a balanced view by targeting respondents from 4 major departmental functions. However, given the sample size and some variation in response rates across departments, our results are subject to possible bias.
Conclusions
Health care delivery systems hold great promise to address tobacco use. 6,14,16 At least 70% of all smokers come in contact with the health care system annually, providing an opportunity to treat large populations of tobacco users. 17 Few studies examine the comprehensive implementation of clinical practice guidelines for the treatment of tobacco use in hospital systems that serve the most medically vulnerable. 18
Louisiana's statewide integrated system of safety net hospitals provided an organizational structure in which to initiate standardized systemic changes. The allocation of cigarette excise taxes makes it possible to offer ongoing evidence-based cessation services to all patients of this public hospital system, irrespective of geographic location, financial class, or health status. The results of the 2003 and 2007 surveys illustrate the potential to provide access to evidence-based cessation services to large populations of smokers by implementing recommended system-level policies and procedures in a statewide safety net health care delivery system.
Footnotes
Author Disclosure Statement
Drs. Moody-Thomos, Horswell, Dellinger, Kaiser, Butler and Mr. Celestin, have no institutional or commercial affiliations that might pose a conflict of interest regarding the publication of this manuscript.
Acknowledgments
The authors wish to thank Monica L. Moffett, M.B.A. and Krysten D. Jones, M.P.H. for assistance with instrument revision and data collection related to this project.