
Abstract
Nursing telephone calls after hospital discharge are commonly adopted as a tool to improve patient satisfaction and continuity of care. Previous research, however, has been inconclusive on the impact of telephone follow-up. The purpose of this study was to comparatively examine patients who received telephone follow-up for response differences on a mail satisfaction survey and 30-day readmission rates for a large health system in southeast Texas. Telephone follow-up, patient satisfaction, and administrative billing data from 2008 to 2009 were retrospectively examined across 10 nursing units that routinely performed calls after patient discharge. Patients eligible to receive a nursing call (N = 10,559) were categorized based on responses to nursing questions or if no contact was made. Logistic regression was used to evaluate whether call data significantly predicted survey response and 30-day readmission rates. Nonparametric analysis was used to evaluate whether survey ratings varied between groups. Completion of telephone follow-up was a significant (P < 0.01) predictor of patient response to the mail survey, with 62% more patients returning surveys after contact. Completion of a nursing call with a patient who reported a physician appointment was a significant predictor (P = 0.04) of lower 30-day readmissions. Readmission rates were 10.8% for patients who did not receive telephone follow-up compared to 9.5% for patients who received a call and who had a scheduled physician appointment. Mean nursing and overall satisfaction scores varied minimally between groups and telephone follow-up was not a significant predictor of patient satisfaction.
Telephone follow-up shows significant predictive value for mail survey response and 30-day readmission rates but does not correlate with patient satisfaction scores in the hospital setting. (Population Health Management 2011;14:249–255)
Introduction
One practice that has been adopted by many hospitals nationwide is telephone follow-up, also known as postdischarge callback, after patients depart the hospital setting. Although these interactions are not billable to payers, they have been recommended by industry experts as a means to improve continuity of care and provide customer feedback to frontline staff. 1 Clinician follow-up provides a vital opportunity to answer patient questions about medications and pain management while reinforcing the importance of physician follow-up outside the acute hospital setting. These activities help prevent adverse events after patients depart the hospital, and clinician calls have been packaged as part of comprehensive discharge redesign that demonstrates reduced 30-day readmissions. 2 –4 Studying the independent impact of a single telephone intervention has been problematic, however, due to the low methodological quality, small patient samples, and heterogeneity of study design. 5 Some studies have been supportive of the role of telephone interventions in patient satisfaction and readmissions, 6,7 while others have been mixed 8 or negative 9,10 in their findings.
The purpose of this observational study was to evaluate the relationship between nursing calls and several metrics for hospital transparency and future reimbursement. A first aim was to determine whether telephone follow-up correlated with return rates of a federally standardized survey instrument, known as the Hospital Consumer Assessment of Healthcare Providers and Systems, commonly referred to as HCAHPS. The second was to determine if call completion to a patient with scheduled physician follow-up was a predictor of 30-day inpatient readmission. A final study aim was to examine the relationship between nursing calls and patient satisfaction rankings of nursing and overall care as recorded in an HCAHPS mail survey.
Methods
The study setting was Memorial Hermann Healthcare System, an 11-hospital health system in southeast Texas. As not all hospitals utilize postdischarge callbacks, 10 nursing units across 4 hospitals were selected based on their usage of these calls between October 2008 and May 2009. The specialties of these units included medical, surgical, orthopedic, obstetrics, and cardiology. Only inpatient and observation encounters were included for analysis.
Nursing telephone follow-up
In 2004, Memorial Hermann developed an internal software application, known as the postdischarge callback system, to facilitate telephone contact with eligible patients after discharge. Clinicians in participating nursing departments perform the calls using a script of 6 standard questions (Fig. 1). Patient lists are populated daily with those who are discharged to home. One or 2 designated employees in each department perform all telephone follow-up; these employees typically are not a patient's caregiver during the inpatient stay. Answers to all questions are recorded in the postdischarge callback system and the sixth question is also transferred for employee-specific tracking. In addition to the standard questions, department-specific questions can be added based on unit preference. Managers and hospital executives receive reports on both the rate of call completion and patient feedback. Development and maintenance of the postdischarge callback system for all hospitals is split between 1 programmer and 1 business analyst and these tasks compose approximately one quarter of their job responsibilities. No new software licensing or hardware was required in the development of the postdischarge callback system.

Screenshot of standard script and questions for postdischarge callback.
Calls are generally placed during daytime hours 1 to 4 days after patient departure. Although multiple attempts may be made to contact a patient, not all patients are reached. Messages are not left for call return in those instances. For the 10 nursing units examined in this study, there were 13,970 patient discharges, 10,559 of which were populated in the postdischarge callback system; 4951 patients were successfully contacted for a response rate of 47%, with rates for individual units ranging from 33% to 59%. Call length averages approximately 3 minutes but may be longer based on the complexity of questions and answers from patients. Based on call length and unanswered attempts, approximately 1 to 2 hours each week per nursing department are spent conducting follow-up calls.
Mail survey administration
After all inpatient and observation discharges, Memorial Hermann transmits necessary data to Press Ganey, a third-party agency, for the mailing of a written survey. The first 27 items on this instrument are standardized HCAHPS questions, with topics on the care from nurses, care from doctors, hospital environment, hospital experience, discharge process, and overall rating of care. Two of these topics, the care from nurses and overall rating, were examined in this study. Surveys are mailed to patients 1 to 3 weeks after discharge; therefore, nursing telephone follow-up always precedes receipt of a mail survey. Patients mail surveys back to Press Ganey, where the responses are assembled into a patient-identified database and transmitted monthly to Memorial Hermann. Using patient medical record and visit numbers in Access 2003 (Microsoft, Inc, Redmond, WA), these data were linked to patients who were eligible to receive telephone follow-up in the postdischarge callback system.
Of the 10,559 patients identified in the callback system, 1947 responded to a single-wave mail survey by August 2009. Response rates for the 10 nursing departments varied from 12% to 28%. Fifty-two mail survey responses had missing values and were excluded from ratings analysis.
Administrative and readmission data
Memorial Hermann collects a large inventory of demographic, diagnosis, and billing information in an administrative decision-support application, known as Sunrise EPSi (Eclipsys, Inc, Atlanta, GA). For the 10,559 patient records identified from the postdischarge callback system, data from Sunrise EPSi were linked via medical record and visit number into this database. Data on patient age, sex, race, payer, and diagnosis were imported as potential adjustments for baseline differences between patients who received telephone follow-up and those who did not.
In addition, Sunrise EPSi was used to identify any patient record that had a subsequent inpatient readmission to a Memorial Hermann hospital in the 30 days after previous discharge. Although this underestimates the actual rate of readmission, given that patients may readmit to nonaffiliated facilities, a majority stay within the system. As the largest system in the Houston metro area, Memorial Hermann holds over a quarter of the inpatient market share. Previous research validated that of 7831 Medicare discharge claims with 30-day readmissions from 2007 to 2009, 85% of patients returned to a Memorial Hermann hospital.
After all patient data were assembled into a single database for analysis, patient identifiable elements were removed. Data were then released to researchers at the University of Texas Health Science Center at Houston for statistical analysis.
Measures
The first dependent variable in this study was patient response to mail surveys based on the presence or absence of completed telephone follow-up. The second dependent variable was 30-day inpatient readmission based on 3 groupings of telephone follow-up: no call completion, call completion with a scheduled physician appointment, and call completion without a scheduled physician appointment, based upon patient response to question 5 of the postdischarge callback system. Two final dependent variables were the satisfaction scores on nursing communication and the overall rating from the mail survey response.
Other independent factors in these analyses included age, sex, race, payer, the 5 largest diagnosis categories (circulatory, respiratory, digestive, musculoskeletal, and pregnancy-related) and the nursing unit before patient discharge. Nursing unit at discharge was a factor enabling examination across units because it adjusts for any baseline difference in departmental performance, but it is not displayed in regression results as it does not extrapolate to other populations. Diagnosis categories were assigned based on the coding of diagnosis-related groups, according to Medicare grouper v26.0.
Analysis
To examine baseline differences between patient groups, patients were segregated into those who received a postdischarge callback and those who did not. One-way analysis of variance tested for significant differences in means of age, average length of stay, charges, and acuity. Chi-square tests determined whether significant associations existed between completion of postdischarge callback and the categorical variables of race, sex, financial payer, and diagnosis.
For the dependent variables of survey response and readmission, logistic regression with hierarchical backward elimination was used to determine which variables were significant predictors. Variables were sequentially entered in the order of demographic (age, sex, race), situational (payer, diagnosis, nursing unit), and observational (status of telephone follow-up) blocks. Two-way and higher order interaction effects were analyzed for significant variables in the logistic regression.
For ratings of nursing communication and overall care, nonparametric multivariate analysis of ranked scores was used to evaluate if telephone follow-up was significantly related to score distribution. The use of nonparametric analysis was selected given the left-skewed nature of survey data and the aim to examine distribution as well as mean differences. Significance for nonparametric analyses was tested using the Puri-Sen L statistic. 11,12
All regression analyses employed the Fischer's “protected t” strategy, as recommended in the regression context, to prevent against alpha level inflation. 13 Data were processed and analyzed using SPSS 18.0 (IBM Inc, Chicago, IL).
Results
Baseline differences
Because patients were neither controlled nor randomized to receiving calls, baseline differences were examined between patients who were contacted with telephone follow-up and those who were not. Patients who were not contacted were significantly older, and more likely to be white and to have significantly different payer and diagnosis distributions (Table 1). No significant differences were observed based on sex, length of stay, acuity, or charges during the hospital stay.
*These variables are included in the baseline comparison of groups but were not used in regression or nonparametric analysis of readmission or survey data.
Patient response to mail survey
Controlling for other predictors, patients receiving telephone follow-up was a significant predictor (P < 0.01) of survey response, with a mean response rate of 22.4% (N = 1107) for patients who received postdischarge callback compared to 15.0% (N = 822) for those who did not. In addition, race, financial payer, nursing unit at discharge and 2 diagnosis categories were significant predictors of survey response (Table 2). No interaction effects were observed among the variables in the logistic regression. As a continuous variable, age did not show linearity of the logit, a requirement for logistic regression, and was removed from survey response analysis.
*Before backward elimination of nonsignificant variables from the logistic regression, the musculoskeletal diagnosis was a significant predictor of increased survey response. Its significance decreased (P = 0.06) after isolating other independent variables. HCAHPS, Hospital Consumer Assessment of Healthcare Providers and Systems; mgd, managed.
30-Day readmissions
Patients receiving telephone follow-up with self-report of a scheduled physician appointment was a significant predictor (P = 0.04) of 30-day inpatient readmission independent of other predictors (Table 3). The rate of readmission for patients who received callbacks with reported physician appointment was 9.5%. For those who did not receive a call, the readmission rate was 10.8%, while the rate was 11.9% for those who received a call and self-reported no scheduled physician follow-up. Call completion without consideration of patient feedback did not reach significance alone (P = 0.14).
*Because these are interaction terms, the true odds ratio is a product of this term with the base term. For example, a Medicaid patient who received telephone follow-up and did not have a physician appointment has odds of 4.30 (2.13 × 2.02) for readmission when compared to a patient with managed care insurance who did not receive postdischarge callback.
In addition, the financial payer, nursing unit at discharge, and pregnancy-related diagnosis category were significant predictors of readmission. Although age, sex, and race have been shown to significantly correlate with readmissions in national studies, 14 the size of those effects would not be sufficiently powered based on this research design.
A significant 2-way interaction effect was observed in the logistic regression of readmission, where the variable of financial payer moderated the predictive value of postdischarge callback (P = 0.02, Fig. 2). For Medicare patients with callbacks, lower odds for readmission were observed regardless of reported physician follow-up. For Medicaid patients with callbacks, patients reporting a scheduled appointment decreased the odds of readmission while the absence of reported follow-up significantly increased the odds. For other payers, telephone follow-up did not provide significant predictive value. Once interaction terms were included in the model, telephone follow-up was no longer a significant independent predictor of readmission in isolation (P = 0.46).
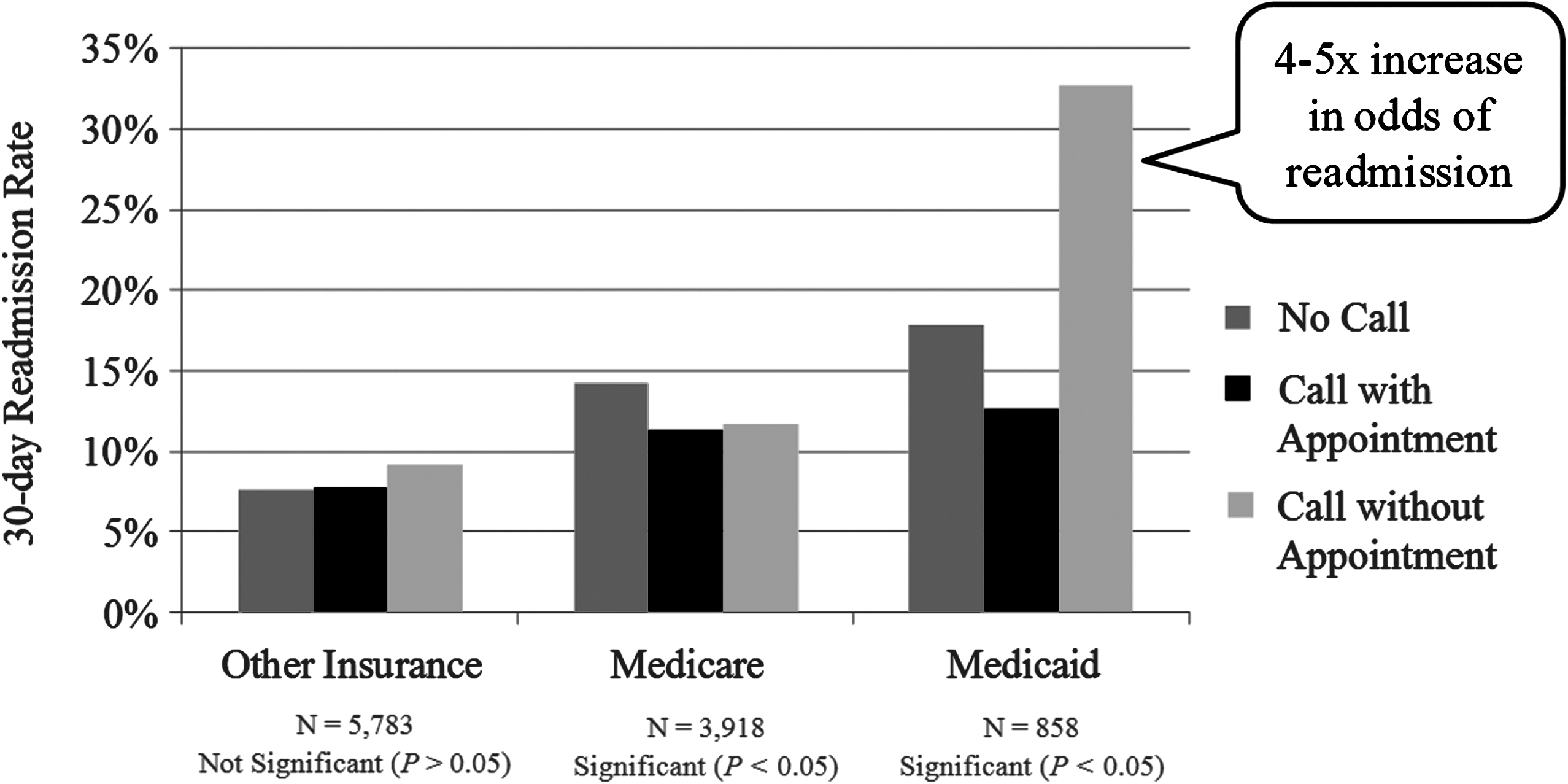
Mean readmission rates shown by telephone follow-up and payer.
Patient satisfaction
For survey ratings, the 3 questions on frequency of nursing communication showed high reliability (α = 0.86) and were assigned numerical values (Never = 1, Sometimes = 2, Usually = 3, and Always = 4) and compiled into a composite score. Overall rating was collected on a 0 to 10 scale from the HCAHPS survey. Mean nursing and overall care ratings were similar between patients who received a call and those who did not (Table 4). Using rank transformation and multivariate Pillai's Trace, the Puri-Sen L statistic showed no significant differences in distribution between the groups (L = 2.24, df 2, P > 0.25).
*Neither of the above categories was shown to be statistically different using nonparametric analysis of score distribution. HCAHPS, Hospital Consumer Assessment of Healthcare Providers and Systems.
Discussion
Contacting patients after a hospital discharge provides a key opportunity to answer questions about care, encourage necessary outpatient activity, and prompt patients to return more detailed mail surveys. While a short telephone conversation is a minor clinical intervention, it may be one of the few activities that help coordinate care during the transition from the hospital setting. This observational research demonstrates that patient response to mail surveys and 30-day readmissions can be predicted from telephone follow-up.
Contact with patients before the receipt of a mail survey predicted a large increase in eventual patient return rates. The observed increase of 62% from this study aligns closely with other research. 15,16 Given the increasing importance of mail survey data in evaluating hospital performance, techniques that increase response rate strengthen data validity and minimize the cost of other techniques such as second-wave mailings.
This research also finds that other factors such as race, financial payer, and diagnosis category are significant in predicting patient response. While telephone follow-up did not significantly interact with any of these factors, these findings support previous research and should be a consideration when examining HCAHPS data. 17
The relationship between telephone follow-up and 30-day readmission rates also suggests that opportunities exist to improve care coordination after hospital discharge. Previous research has found that nearly half of all Medicare patients with 30-day readmissions have no outpatient activity after their original hospital discharge and that $17 billion is spent annually on unplanned Medicare readmissions. 14 Although this study design does not establish causation, postdischarge contact encouraging physician follow-up and filling prescriptions would be a cost-effective tool for payers if shown to reduce readmissions. Because Memorial Hermann receives no reimbursement for patient follow-up, its investment focuses on coordinating care to improve quality. Beginning in October 2012, however, up to 1% of total inpatient Medicare revenue will be at risk based on 30-day readmission rates. This greatly exceeds the cost of developing and maintaining a program for postdischarge callbacks and may financially incentivize the expansion of such efforts.
The interaction between telephone follow-up and financial payer suggests that specific payer groups have varying circumstances influencing readmission. An issue facing Medicaid patients at high risk of readmission may be access and timely follow-up with a physician after a hospital discharge. On the other hand, although callbacks for Medicare patients overall correlated with lower readmission rates, physician follow-up did not provide predictive value. This study does not definitively explore these relationships, but financial payer and its interaction should be an important consideration for future analyses of telephone follow-up after hospital care.
An unexpected finding of this study was that telephone follow-up did not predict patient satisfaction ratings for nursing or overall care. Although consistent with other studies, 9,10 telephone follow-up is a prevalent tool among hospitals and other service industries with the expressed intent of increasing satisfaction. One consideration that may limit the influence of such calls on hospital satisfaction scores is federal regulation prohibiting providers from encouraging high ratings or asking HCAHPS-like survey questions. 18 This guided Memorial Hermann's script for the postdischarge callback system and necessitated compliance throughout the hospitals. Another possibility is that the units that participate in postdischarge callbacks have already achieved high satisfaction, both for patients who are reached by telephone as well as those who are not. This study cannot rule out any possible effects on patient satisfaction from postdischarge calls, but the data suggest any relationship to be more complex than a simple increase in scores for contacted patients.
The findings of this research prompted Memorial Hermann to review the aims of telephone follow-up after an inpatient episode. To prioritize the importance of follow-up care while speaking with patients, the postdischarge callback system has been enhanced. Clinicians making callbacks can now identify the primary care physician from the time a patient was admitted to the hospital. If a patient responds during the callback that he or she has not scheduled a follow-up appointment, a pilot program is under way to transfer patients to an internal referral center where operators can help patients select a physician. Operators then facilitate a physician appointment or transfer the patient to a doctor's office for scheduling. Memorial Hermann continues to expand its use of telephone follow-up with over 7000 monthly calls completed across the 11 hospitals in early 2010. As other organizations consider the use of telephone follow-up, this study should guide their goals and measures. Telephone follow-up provides predictive capacity for HCAHPS survey responses and 30-day readmissions but does not correlate with changes in patient satisfaction. Measurement of specific payers and patients who report no physician appointment should be factored into program design and the specific scripts that clinicians use when contacting patients.
This research was limited by the uncontrolled, nonrandomized basis for patient data. Although several known differences were adjusted for in the analysis, the possibility remains that unidentified factors may vary significantly between patients who received telephone follow-up and those who did not. In addition, this study was based exclusively on the hospital setting with a short follow-up call. A single postdischarge interaction does not substitute for coordinated disease management or a medical home, much larger factors in ultimate health outcomes. Finally, readmissions data were based only on Memorial Hermann facilities as patient admissions to other facilities were not identifiable for inclusion in this study. Despite these limitations, this study is rare in its size and in spanning multiple hospitals and specialties in its analysis.
Conclusion
Coordinating care after a hospital discharge is a fragmented process with many opportunities for suboptimal outcomes; nationally nearly 1 in 5 Medicare patients is readmitted to another inpatient facility within 30 days of discharge and patient satisfaction scores still show high inconsistency between providers.
Telephone follow-up in a consistent, scripted manner is a significant predictor of readmission and patient survey response. This tool may be part of effective hospital practices to help manage patients over the continuum of care settings. Postdischarge callbacks, however, present no clear relationship to HCAHPS score improvement in this study. This contrasts with recommendations from industry consultants that postdischarge callbacks are a systematic way to improve patient experiences.
Footnotes
Acknowledgments
Kimberly Dunn, M.D., Ph.D. of the University of Texas graciously provided guidance on this research and its publication.
Author Disclosure Statement
Mr. Murray and Ms. Powers are employees of Memorial Hermann Healthcare System in Houston, Texas. While enrolled in graduate studies at the University of Texas, Mr. D'Amore is an employee of Eclipsys, Inc, which offers Sunrise EPSi decision support and patient reporting applications to Memorial Hermann. Dr. Johnson disclosed no conflicts of interest.