
Abstract
Lack of medication compliance is harmful to health care systems from both a clinical and economic perspective. This study examines the methods that disease management organizations employ to identify nonadherent patients and to measure effectiveness of compliance programs for patients with diabetes, hyperlipidemia, and cystic fibrosis. In addition, this study investigates the degree to which disease managers assume risk in their contracts, and whether compliance strategies are being coordinated with payers' use of value-based insurance design, in which patient cost sharing is a function of the relative value of pharmaceuticals. This study's findings suggest that disease management may be falling short in terms of: (a) comprehensive commitment to expert-recommended at-home devices used to self-diagnose and measure health indicators; (b) early adoption of expert-recommended new technologies to measure and improve compliance; (c) intensity of use of standard tests in outpatient clinics; (d) coordination of compliance strategies with payers' use of value-based insurance design; and (e) the proportion of risk assumed in disease management contracts. (Population Health Management 2012;15:20–28)
Introduction
Our focus here is medication compliance. Compliance or adherence (we will use these terms interchangeably) typically is defined as the extent to which patients take medications as prescribed by a health care provider and in accordance with instructions on the label. This includes failure to fill prescriptions, improper timing, inappropriate dosing, and lack of persistency. 1 Approximately 50% of patients are noncompliant. 2 Noncompliance is comparatively high among vulnerable populations with chronic conditions, especially the elderly and the young.
Noncompliance is harmful to the health care system, from a clinical as well as an economic standpoint. 3 In the United States, poor adherence contributes $177 billion annually in total direct and indirect costs. 4 In addition, poor adherence causes 125,000 deaths each year. 5
Barriers to adherence include out-of-pocket costs for pharmaceuticals, side effects, difficulty of managing multiple prescriptions, patients' understanding of disease and ability to navigate the health care system, cognitive impairments, and in some cases, a reduced sense of urgency because of asymptomatic conditions.
In this study, we examine the role disease management plays in addressing adherence in patients with chronic diseases, specifically diabetes, hyperlipidemia, and cystic fibrosis. We chose these 3 diseases because each has distinct barriers to proper medication use. The background section provides context on the issues of chronic disease and medication compliance, and how disease management addresses these issues. The survey section consists of a survey of disease management organizations to examine current trends in compliance strategies.
Background
Medication noncompliance among chronically ill
Medication noncompliance is a significant problem that primarily affects patients with chronic diseases. The increasing prevalence of chronic diseases is well documented. According to the Centers for Disease Control, in 2005 almost 1 of every 2 US adults had at least 1 chronic illness. 6 Chronic diseases affect people of all ages. The number of patients with chronic diseases, many of whom have multiple comorbidities, is projected to continue increasing over time, particularly as the population ages. 7
It is estimated that 50% of patients are noncompliant with their prescribed medication regimens. 2,8,9 Noncompliance is pervasive, and high rates have been reported across all socioeconomic and age groups and in multiple health care settings. 10 Compliance tends to be more of a problem for the chronically ill who are on (multiple) medications for extended periods of time. In a widely cited study, a dramatic drop-off in compliance was observed 6 months after the initiation of drug therapy, with 50% of patients discontinuing regular intake of maintenance medications for chronic conditions, such as cholesterol-lowering drugs for hyperlipidemia. 11
Channels of expenditures on health care for chronic conditions have been changing, with comparatively more spending on outpatient care and prescription drugs and less on inpatient care. Because chronic diseases now are managed mostly on an outpatient basis, often at home, they require a significant amount of patient self-care. As reported by the World Health Organization (WHO), it has proven difficult to predict which chronically ill patients will be noncompliant with respect to medications that have been prescribed for them because patient characteristics are poor predictors of adherence behavior. 8 For example, race, sex, socioeconomic status, and even disease type have not been associated consistently with degree of compliance. 12 Indeed, the above-mentioned WHO report emphasizes: “Adherence problems are observed in all situations where the self-administration of treatment is required, regardless of type of disease, disease severity, and accessibility to health resources.” 8
Medication noncompliance is associated with increases in both the morbidity and the mortality of chronic diseases. 13 Poor compliance alone results in approximately 125,000 deaths in the United States each year. 5 The WHO report asserts that: “Increasing the effectiveness of adherence interventions may have a far greater impact on the health of the [global] population than any improvement in specific medical treatments” and that “poor adherence is the primary reason for suboptimal clinical benefit.” 8 Noncompliance not only contributes to substantial worsening of disease and death but also to increased health care spending. Hospital costs arising from poor medication compliance are estimated to be approximately $100 billion per year in the United States. 12 In aggregate, noncompliance is estimated to cost approximately $177 billion annually in direct and indirect health care costs. 14
Methods to identify and measure noncompliance
Compliance can be difficult to measure accurately. A variety of strategies have been explored to quantify compliance, but each presents challenges, such as reliability, feasibility, and cost. Examples of direct measurement include directly observed therapy (eg, pill counts), electronic medication monitors that record when medication containers are opened or medication is dispensed, and biochemical assays that measure concentrations of a drug, its metabolite, or a biological in the blood or urine. 12 Although direct methods are considered the most accurate to assess compliance, they are expensive, burdensome to providers, and invasive to patients. 12
Most methods for measuring medication compliance are indirect and include patient self-reporting through questionnaires, interviews, or medication diaries; provider estimates of their patients' compliance; and review of administrative data (eg, pharmacy claims, dispensing records). Derived from pharmacy claims data analysis, the medication possession ratio (MPR) is the most commonly used metric to track compliance. MPR summarizes a medication refill history over a period of time by calculating how many doses of medication a patient filled during a specific time period compared with how many doses should have been filled. Each method has its drawbacks, however. Patient self-reports can be subject to patient recall issues and have been found to be significantly biased in favor of unrealistically high rates of compliance. 10,15 Provider estimates of patient behavior similarly overestimate compliance, 16,17 and reviews of pharmacy claims and dispensing records can be “notoriously inaccurate.” 18
Barriers to medication compliance
Patients can be noncompliant with their prescribed medications for a myriad of reasons. First, disease-specific issues can lead to noncompliance. For example, patients with asymptomatic diseases often do not feel urgency to take medications because they do not perceive the benefit, especially when their health care provider fails to educate them about their disease and the benefits of taking medication. Even in the presence of severe disease symptoms, medication side effects, uncomfortable administration, length of treatment, unpleasant or inconvenient frequency of dosage, and complex medication regimens are all associated with decreased medication compliance. 10,12
Second, patient-specific issues also play a role. To illustrate, a patient's health literacy is critical because patients cannot take their medications correctly if they cannot read instructions or properly interpret the label. 5 Other reasons that patients typically cite for medication noncompliance include forgetfulness, particularly among seniors, emotional factors, and even conscious decisions to forgo doses. 12 To illustrate, compliance among children with chronic diseases is often below 50% and is thought to be the “single greatest cause of treatment failure” for these patients. 19 Children often resist taking their medications because of a lack of understanding of their disease and its progression, as well as defiant contrarian behavior. 15
Third, financial constraints contribute to medication noncompliance. Financial constraints impact 3 subgroups in particular: those without prescription coverage; low-income seniors; and the chronically ill. In 2007, one in 7 Americans younger than age 65 reported not filling a prescription in the previous year because they could not afford their medication, an increase from 1 in 10 in 2003. 20 This number rises to as many as 25% among seniors, a group with the highest prevalence of prescription drug use. 21 The high rate of medication use among seniors compounds the financial constraint barrier in that it drives up out-of-pocket costs; nearly one third of seniors on fixed incomes reported having spent $100 or more per month on prescriptions in 2003. 21
Disease management
Disease management is a comprehensive tool used to address noncompliance. Given the increased need for patient self-care and the accompanying problem of medication noncompliance among patients with chronic diseases, strategies to improve compliance are essential features of successful disease management programs. Programs differ fundamentally in rationale and content, ranging from patient-directed education with relatively little practitioner involvement to intensive practice-based efforts to redesign and realign entire care delivery systems. 22 Strategies range from “passive” (periodic sending of educational materials to patients and providers) to “active” (intensive identification and measurement of noncompliance, as well as promotion of compliance). 23 Despite variability in program content, certain general approaches are common across the industry. Most programs identify at-risk patients, offer patient self-management education, follow evidence-based clinical practice guidelines aimed to modify patient and provider behavior, and evaluate clinical and cost-effectiveness outcomes.
The disease management industry is characterized by heterogeneity in organizational structure; volatility as vendors enter, merge, and exit the market; and complexity, owing to wide variations in utilization of specific strategies, extent and mode of patient and physician interaction, and methods of tracking clinical and economic outcomes. Indeed, disease management organizations come in all shapes and sizes. These include independent commercial vendors such as Matria, Healthways, and Health Dialog, but also subsidiaries of payers, such as Aetna, Humana, and WellPoint, and not-for-profit hospital-based entities, such as the Mayo Clinic, the Joslin Diabetes Center, and the Cystic Fibrosis Center at Stanford. Disease managers contract with national and regional health plans, large self-insured employers, as well as hospitals and large medical groups.
Disease managers utilize 3 categories of technologies to reach patients, monitor, and coordinate care: data capture and monitoring systems that collect information about a patient's health status and prescription records; audiovisual communication systems that link patients, providers, and pharmacies; and telephone-, Internet-, CD-ROM-, or DVD-based self-help, education, and training systems. 24 In recent years, some disease managers have offered services providing reminders by way of text messages on cell phones, personal digital assistants, and pillboxes with paging systems. 12
Disease management seems an intuitively appealing way to improve the quality and reduce the cost of care, as well as to enhance health outcomes for the chronically ill, but is it worth the investment? Return on investment (ROI) can be measured in terms of cost-effectiveness or cost savings. 25 A cost-effective program implies that the additional resources expended on disease management result in an improvement in health outcomes. As such, disease management may be considered value for money, despite the fact that more money is being spent than without the program in place.
Conversely, a cost-saving program implies that the additional resources spent on disease management are more than compensated for by a decrease in total health care spending (ie, hospital, physician, outpatient care savings). 26 Conflicting reports on ROI have sparked a contentious debate on the value of disease management. Thus far, no consensus has been reached, as studies have shown ROI ranging from negative (not cost-effective or cost saving), to no impact at all, to positive (cost-effective or cost saving). 27 –29 Because numerous factors may affect patient outcomes as well as inter-patient variability, calculating cost-effectiveness and cost savings is inherently difficult. The long time frame during which benefits associated with an intervention are likely to appear makes it particularly challenging to unequivocally demonstrate cost-effectiveness or cost savings. To illustrate, improved compliance with diabetic medication regimens is likely to increase pharmaceutical costs in the short term, but it could take at least several years of improved glycemic control to reduce overall medical costs. 25
Survey
To empirically evaluate the role disease management plays in strategically overseeing compliance, we examined 2010 trends in the management of hyperlipidemia, diabetes mellitus, and cystic fibrosis. Effective management of cystic fibrosis requires adherence to a daily, life-long regimen of a low-fat, high-protein diet, oral pancreatic enzymes, vitamins, caloric supplements and, in some cases, special dietary formulas, bile salts, and antacids to control gastrointestinal malabsorption. To prevent harmful secretions from accumulating in the bronchial tree, patients require routine airway clearance therapy, traditionally administered via chest physiotherapy, accompanied by inhalation of nebulized drugs. Additional therapies include bronchodilators, inhaled mucolytic agents, oral expectorants, and sometimes long courses of antibiotics (eg, aimed at combating chronic sinusitis). 30 Hyperlipidemia requires relatively “light” management focused on chronic outpatient management, regular follow-up through lipid screening and blood pressure control, and an emphasis on self-management skills. 31,32 A portion of the population whose short- or long-term risk for coronary heart disease is high will require low-density lipoprotein (LDL)-lowering drugs in addition to therapeutic lifestyle changes to reach designated goals for LDL cholesterol. Diabetes mellitus is a special case in that its management rarely involves only 1 disease. Common features of disease management programs include patient education on the appropriate use of a glucose meter, the role of diet and exercise, the importance of HbA1c testing, blood glucose, and retinal exams, microalbumin tests, medication management, and the management of hypoglycemia.
Per disease, by way of survey, we explored methods used to identify nonadherent patients, to improve medication compliance, and to measure the effectiveness of compliance programs. Further, we probed the correspondence between disease management organizations' compliance strategies and clinical practice guidelines, as well as payers' use of value-based insurance design.
Based on contacts previously established for our published work in the early 2000s, we selected 5 experts to pilot interviews to help design and refine the survey instrument.
27
–29
Subsequently, the following inclusion criteria were used to identify 58 leading disease management organizations: • Organizations that offer “disease management” programs that specifically target 1 or more of the following diseases: diabetes, hyperlipidemia, and cystic fibrosis; • Organizations that have direct patient and provider contact; • Organizations that are hospital based, or accredited by the National Committee for Quality Assurance, or the Utilization Review Accreditation Commission, or members of the Care Continuum Alliance, or members of the International Disease Management Association.
Our inclusion criteria narrowed the pool of survey candidates to entities that conformed to the standard definition of comprehensive disease management. As a result, we excluded entities that strictly focus on medication therapy management and educational software. We note that there are inherent limitations with respect to the self-reported data we collected, such as bias, as respondents may report what they think others want to hear. To address the potential for bias, we attempted to verify self-reported findings as best we could by examining publicly available data
Thirty-one respondents completed our survey, which is a 53% response rate. There were 3 categories of respondents: heads of clinical programs; chief nurse care practitioners; and media affairs specialists. Twenty-three respondents offered diabetes programs, 18 offered hyperlipidemia programs, and 6 offered cystic fibrosis programs. Only 1 respondent offered programs targeting all 3 diseases. Three offered only cystic fibrosis programs, 3 provided only diabetes services, and none offered only hyperlipidemia disease management. Of the 31 survey respondents, 48% were independent vendors, 26% were payer based, and 26% were hospital based. Of the 23 disease managers who offered diabetes programs, 56% were independent vendors, 22% were payer based, and another 22% were hospital based. Of the 18 respondents who have hyperlipidemia programs, 61% were independent vendors, 22% were payer based, and 17% were hospital based. Finally, of the 6 organizations that provided cystic fibrosis programs, half were independent vendors, one third were hospital based, and one sixth were payer based.
Results
Sponsors or purchasers of disease management services were mostly regional, local, or national health plans, and large self-insured employers. Of the 31 survey respondents, 65% contracted with regional or local health plans, 54% with large self-insured employers, 50% with national health plans, and 31% with hospitals or large medical groups. Approximately 40% of respondents reported contracts with more than 1 type of contractor.
We analyzed disease manager concordance with the use of at-home devices used to self-diagnose and measure health indicators, outpatient clinic tests to track health, identifiers of noncompliance, promoters of compliance, and patient reminders, recommended in nationally recognized clinical practice guidelines (Fig. 1). 27 –29
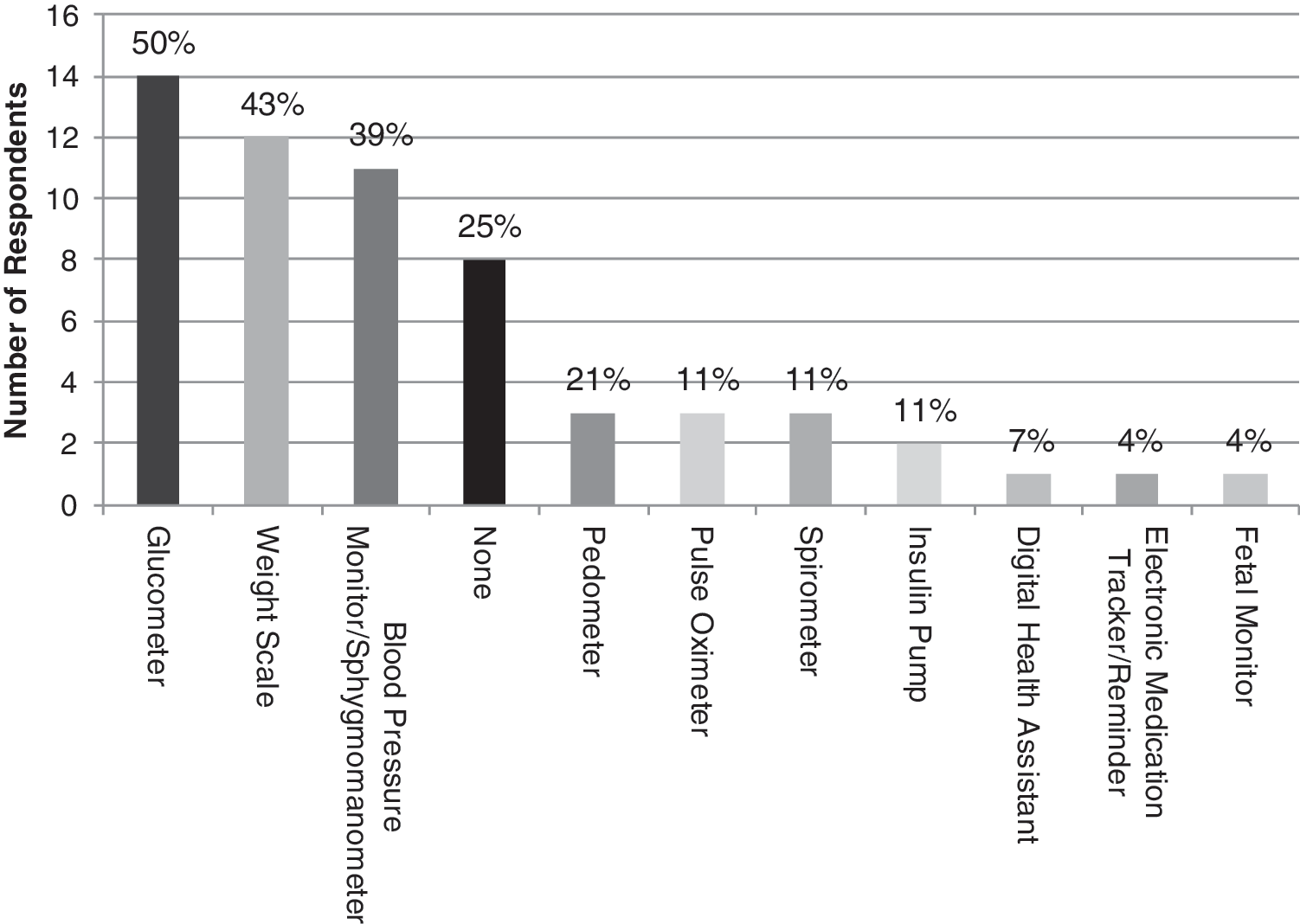
At-home devices. Percentage of disease managers who incorporate expert-recommended at-home devices in their programs to self-diagnose or monitor health.
Across disease management programs that target the 3 diseases, the use of expert-recommended at-home devices to monitor health or self-diagnose is both low and uneven. Not a single device, not even a weight scale, was incorporated by the majority of respondents; 25% of respondents did not report the use of any at-home device.
In the outpatient clinic, most disease managers adopted tests considered “routine” (conducted at each physician visit) in clinical practice guidelines to track diabetic patients' health. In Figure 2, these routine tests are the first six, from left to right. However, a significant drop-off in incorporation of tests in diabetes programs occurs the less routine the tests.
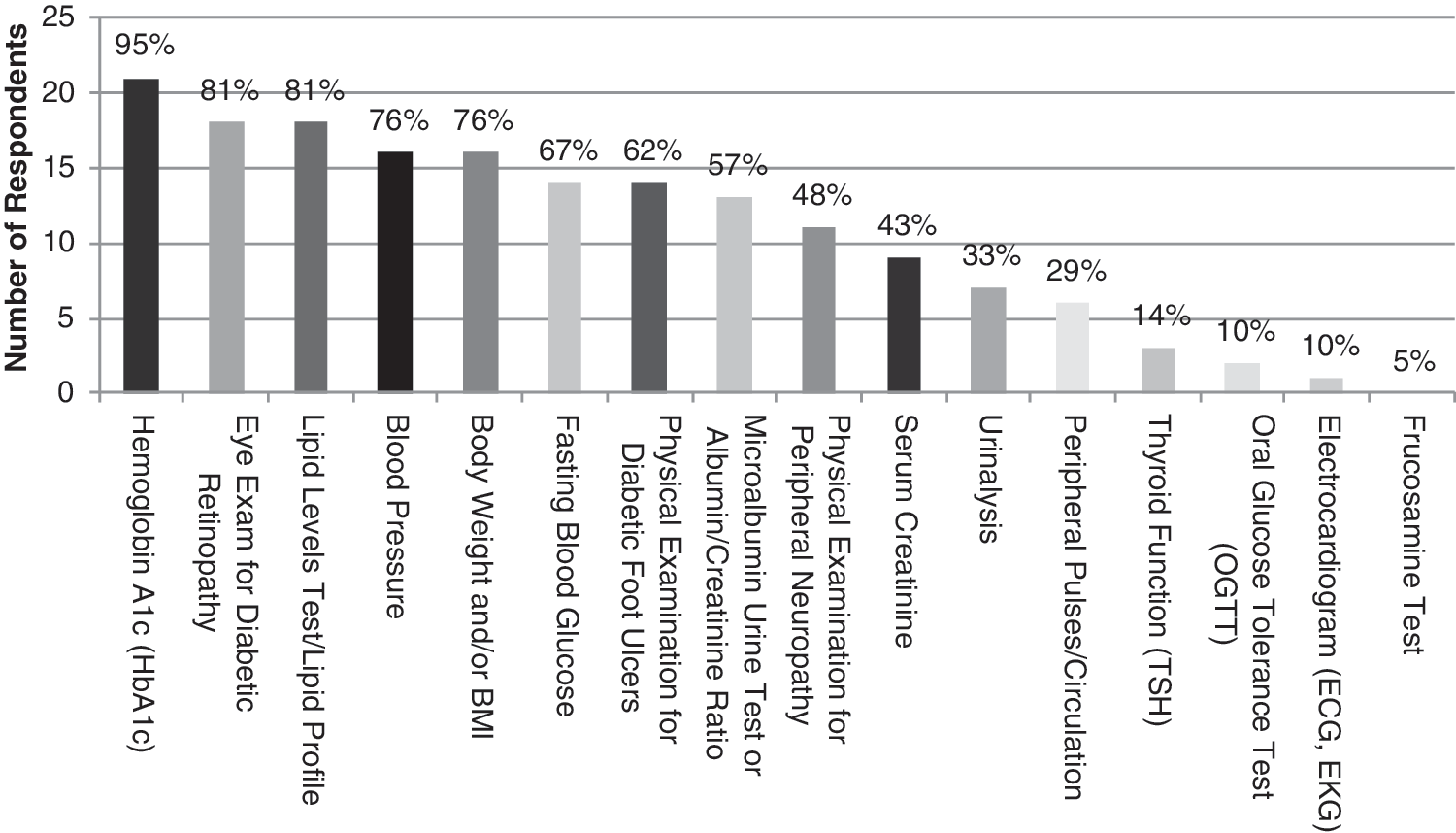
Diabetes tests. Incorporation by disease managers of diabetes tests, from routine, conducted at each physician visit (first 6 tests from left to right), to less routine (the last 10 tests).
We observed a high degree of incorporation by disease managers of expert-recommended routine tests for hyperlipidemia in the outpatient clinic (Fig. 3), with the exception of the electrocardiogram. However, this is not considered a routine test.
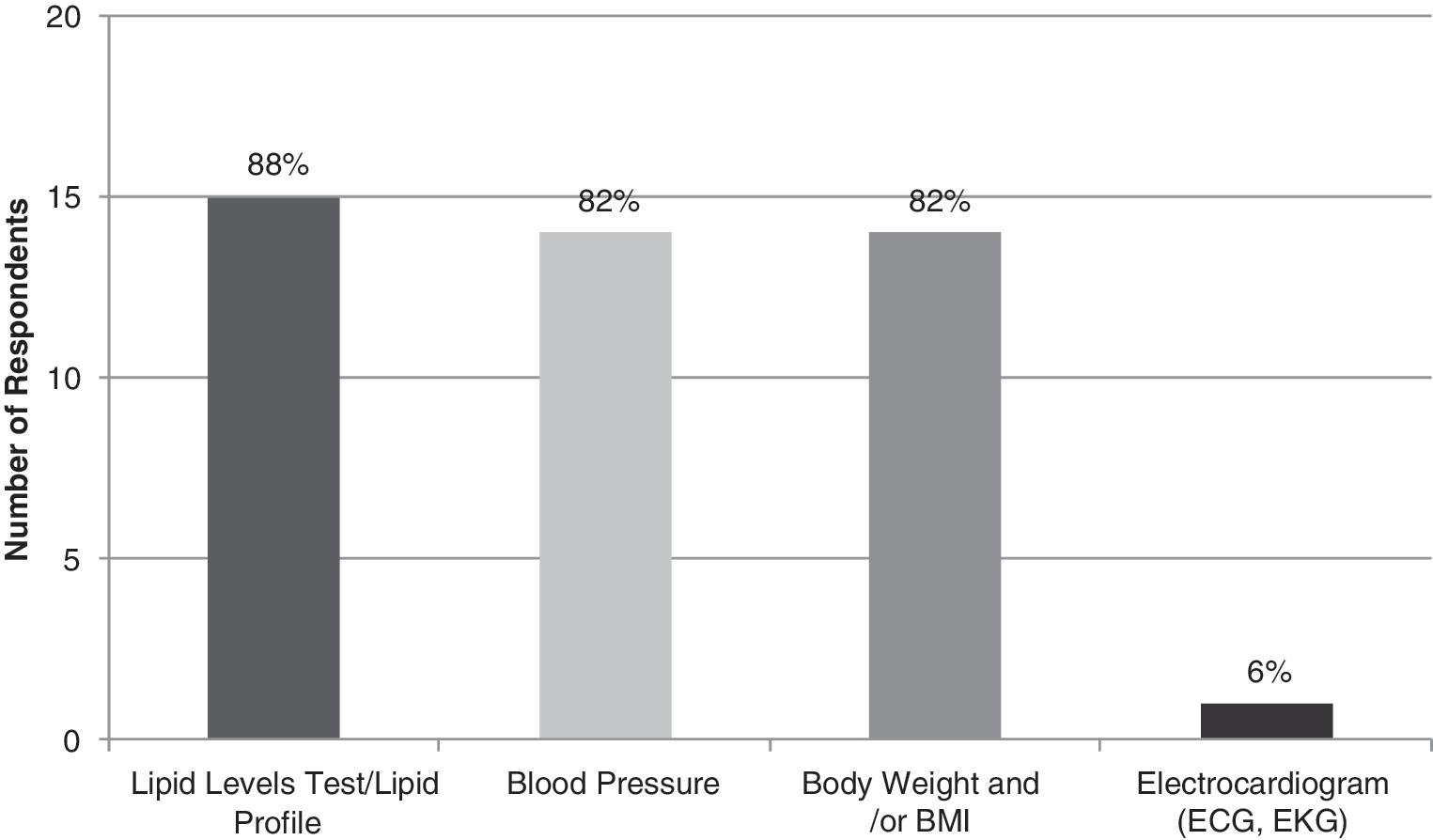
Hyperlipidemia tests. Use of expert-recommended hyperlipidemia tests. In outpatient clinics, the use of routine tests (first 3 tests from left to right) by disease managers is high.
We observed low and uneven incorporation by disease managers of tests considered routine (first seven in Fig. 4, from left to right) in the outpatient clinic to track the health of patients with cystic fibrosis.
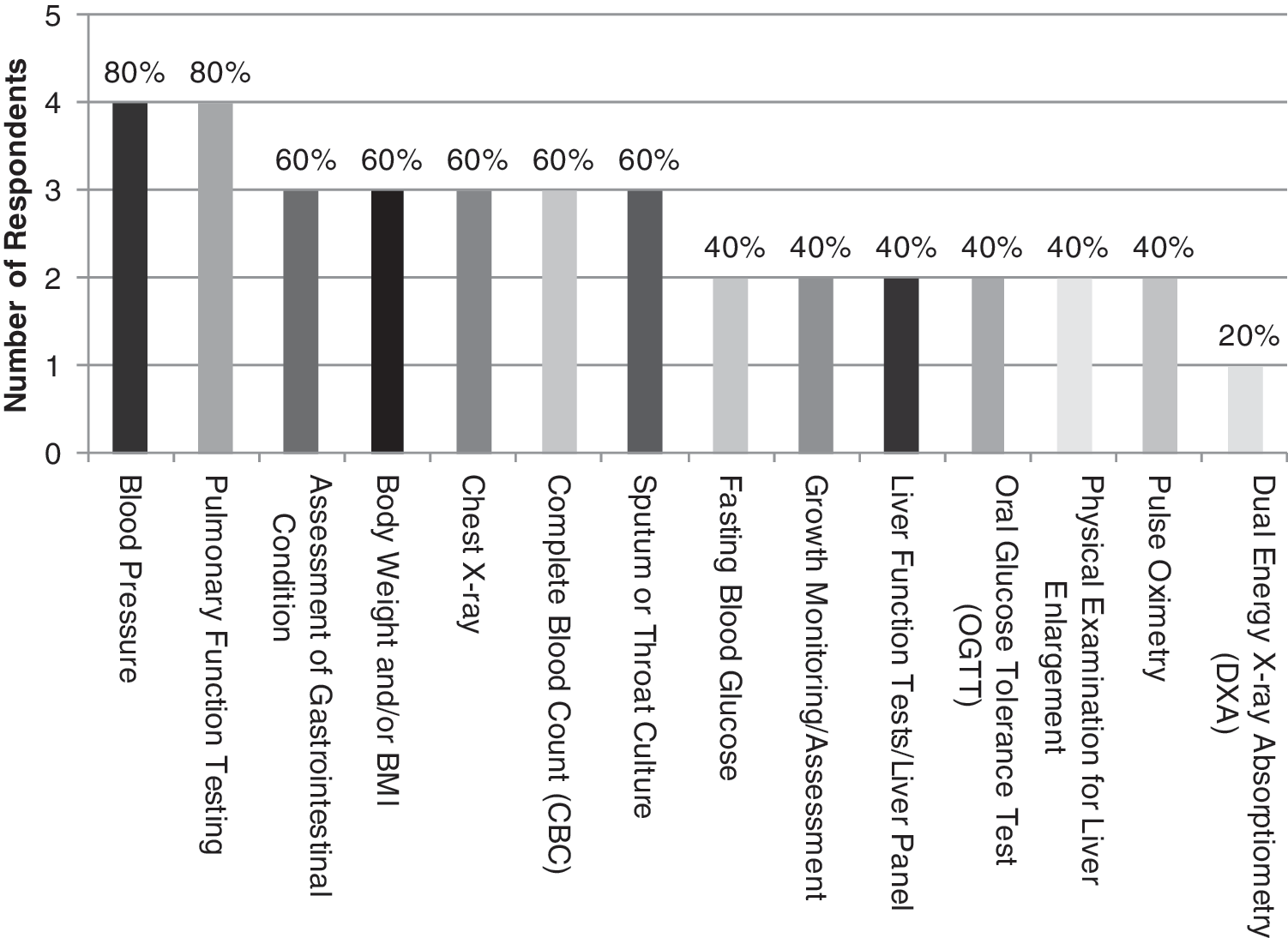
Cystic fibrosis tests. Disease manager incorporation of expert-recommended cystic fibrosis tests. The majority of respondents incorporate routine tests (first 7 from left to right), while a minority incorporation less routine tests (last 7).
Health care providers must assess levels of patient compliance before making initial prescribing decisions, but also prior to laying out a treatment plan. Figure 5 reports the methods used by disease managers to identify medication noncompliance. Although all reported they identify noncompliance, we observed a lack of consistency across respondents in terms of the methods used. Among the survey respondents, there is greater use of low-tech self-management tools than high-tech devices. In fact, there is hardly any use of new technological devices, such as: • MEMS caps (medication bottle cap with embedded microchip to record bottle openings); • Smart blisters (foil technology that saves information on drug blister package); • Ingestible event markers; • Pill counters.
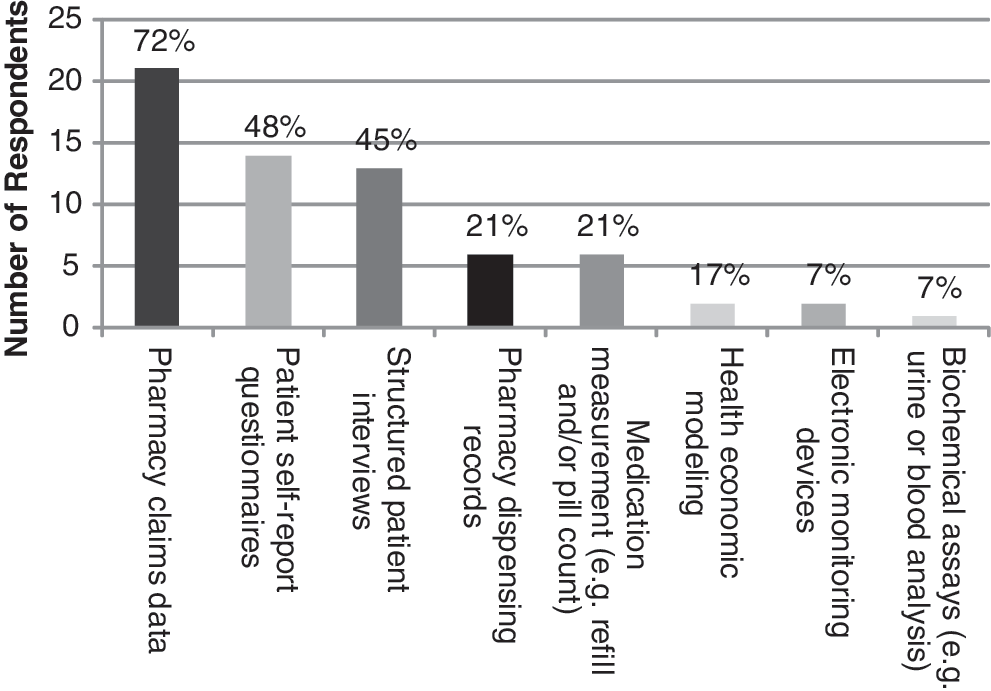
Identifying noncompliance. Methods used by disease managers to identify noncompliance.
Almost all respondents use multiple methods to promote appropriate compliance (Fig. 6). Most methods focus on patient self-management, through educational brochures and guidelines and telephone support. It is noteworthy that less than half of the respondents use intensive in-person monitoring to promote compliance.
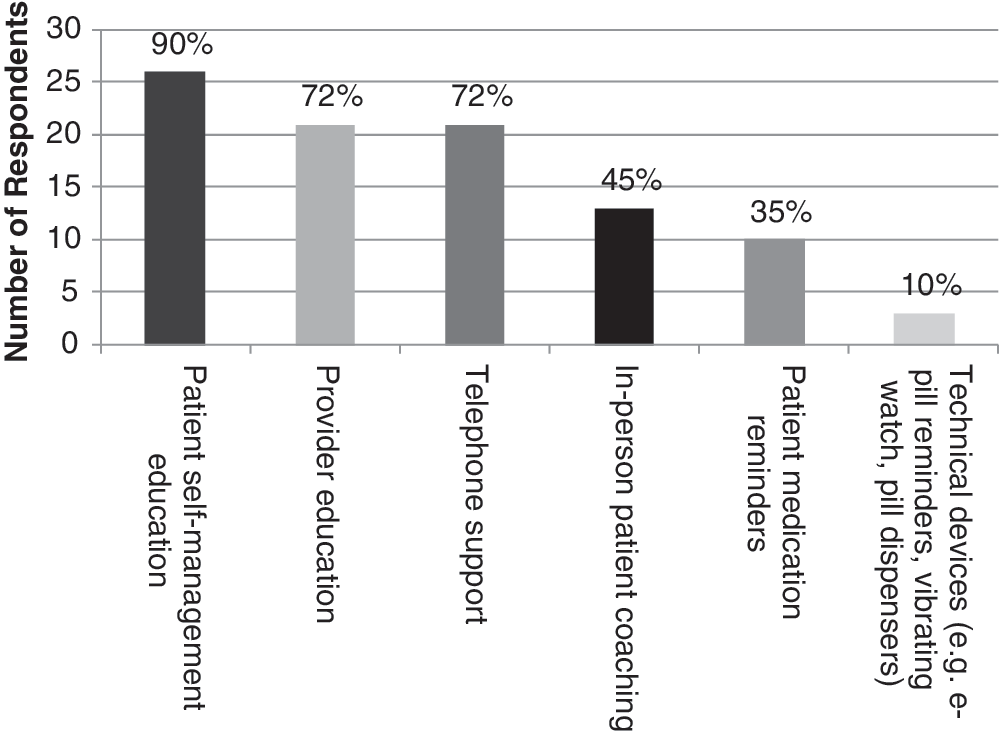
Strategies used by disease managers to promote compliance. Almost all respondents (29/31) use 2 or more methods to promote appropriate compliance.
Fewer than 50% of survey respondents employ any patient reminders. When patient reminders are used, disease managers contact patients mostly with low-technology tools, such as phone calls (Fig. 7).
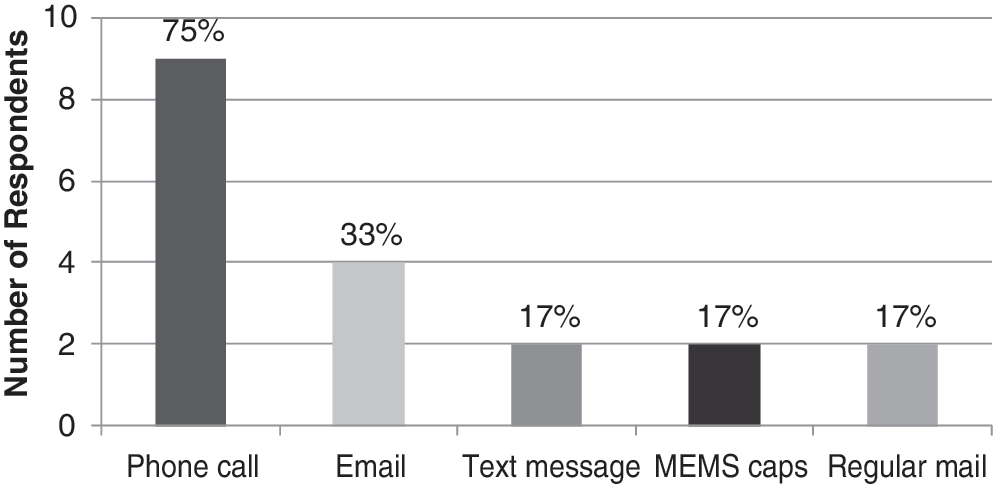
Patient reminders used by disease managers.
We observed that respondents considered patient and physician communication and support the most important features of a successful disease management program aimed at increasing medication compliance (Fig. 8). Respondents considered a program's cost-effectiveness or cost savings less important.
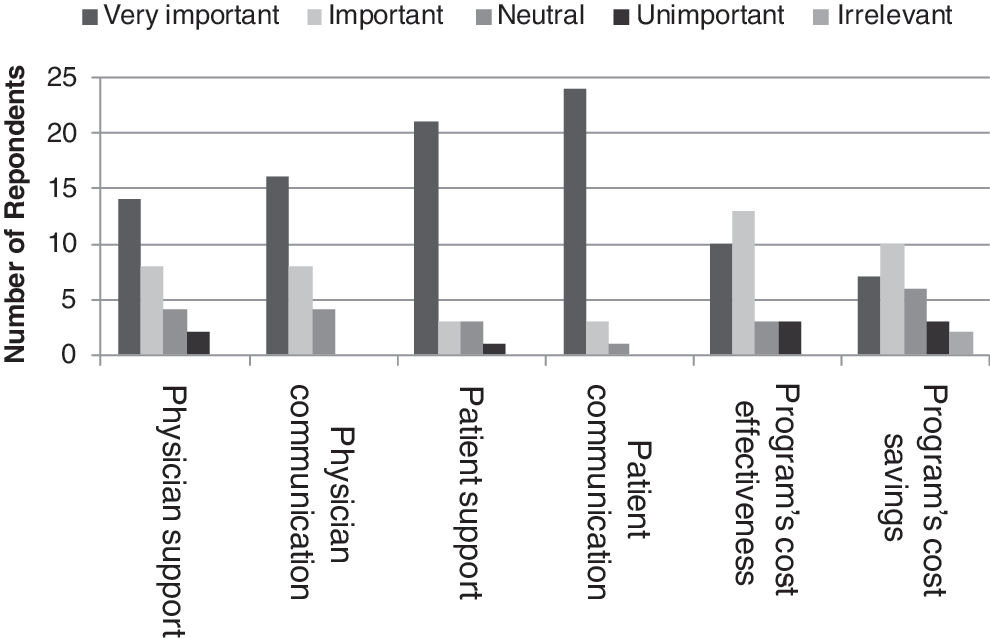
Relative importance of features of compliance programs, framed as selling points to potential contractors.
About 70% of all disease managers we surveyed reported measuring the effectiveness of their compliance programs (Fig. 9). Of those, more than two thirds use pharmacy and medical claims data reviews, and close to 60% employ patient self-reports. Few, however, utilize newer technologies, such as MEMS caps, smart blisters, or ingestible event markers; none do pill counts.
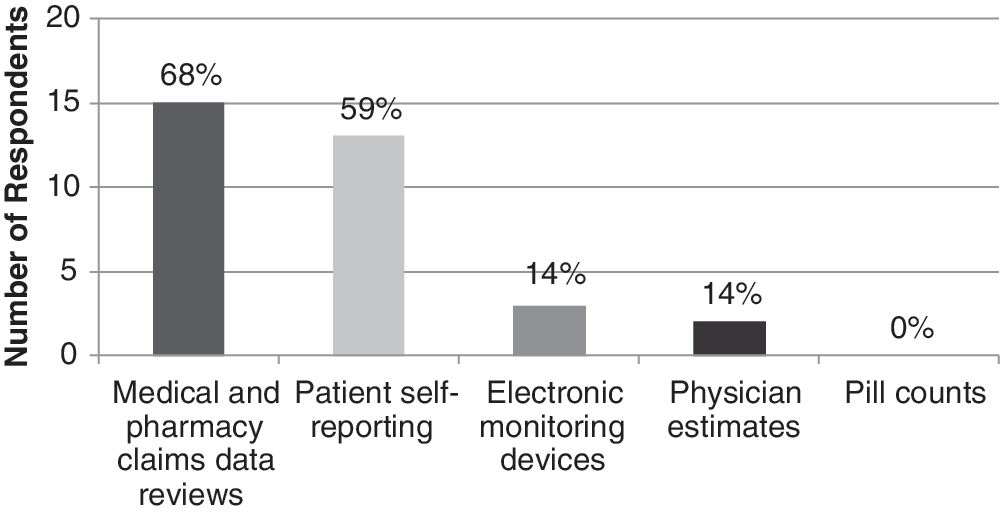
Methods disease managers use to measure the effectiveness of their compliance programs.
As a follow-up question, we asked which methods were used to measure compliance, and what kinds of results were being obtained. Two thirds (20) of respondents answered our follow-up query. About one third (7) of those who responded stated that their method of measuring compliance was proprietary. The other two thirds (13) who did specify a method used retrospective databases. The most commonly used method reported (almost all who responded) was the MPR. Other methods include a continuous measure of medication gap, which provides an indication of the percentage of time the patient does not have the medication available for use. Respondents reported a median baseline (preintervention) MPR of 65%, while the median compliance rate achieved postintervention was 78%. Measurement occurred over a time period of roughly between 6 months to 1 year.
Disease managers report having an almost equal division of contracts between fully capitated (27%), hybrid (40%), and fee-for-service (33%). This is contrary to what we expected. In a previously conducted survey of the disease management industry from the early 2000s, almost all respondents voiced confidence in the ability to achieve cost savings, and therefore assume risk in the form of capitated contracts. 33
In economic terms, 55% of disease managers describe their programs as cost-effective, 40% as cost saving, and 5% as having no effect on costs. There appears to be an inconsistency between the importance disease managers attribute to cost-effectiveness and cost savings as selling points to potential contractors of programs targeting noncompliance (Fig. 8), and whether they deem their programs cost-effective or cost saving, This is also reflected in the relatively low proportion of risk disease managers assume in their contracts, as well as in the fact that only one third of survey respondents incorporate pay-for-performance measures in their contracts, and only one quarter explicitly coordinate drug compliance strategies with payer value-based insurance design.
Discussion
The original promise of disease management targeting noncompliance is that it would represent a win–win situation for all stakeholders involved—patients, payers, health care providers, the pharmaceutical industry—as improved adherence likely would lead to better health outcomes, which in turn would yield increased revenue for the industry and reduced costs for payers.
With some exceptions, however, the promise of a win–win situation for all stakeholders involved has yet to be fulfilled in terms of consistent use of compliance strategies that correspond with current best practices and new technological development. We observed low and inconsistent incorporation of expert-recommended evidence-based strategies. Further, many respondents claim their programs are cost-saving or cost-effective, yet there appears to be an inconsistency between this claim and the relative proportion of risk they assume as well as pay-for-performance measures in their contracts. Also, the majority do not coordinate drug compliance strategies with value-based insurance design (ie, tailoring pharmaceutical cost sharing to its value).
Value-based insurance design incorporates 3 pillars of potentially successful, patient-centric policies aimed at improving compliance: (1) address financial barriers to the patient; (2) improve data infrastructure in order to identify nonadherent patients and measure outcomes; (3) implement payment reform that rewards value to the patient, not services per se.
First, because one of the largest barriers to compliance is relatively high patient cost sharing, it is imperative that cost-effective therapies be adequately covered. Payer reduction of co-payments for cost-effective medications, in addition to use of disease management initiatives, has been shown to increase medication compliance compared to disease management programs alone. 27 Several large payers, including 2 respondents to our survey, have instituted programs that reduce patient co-payments for drugs considered to have relatively high clinical value in order to encourage their utilization. These include beta-blockers, statins, calcium channel blockers, hypoglycemic agents, and asthma medications. 26,28
However, on the whole, it appears that health plans' formulary design–use of co-payment systems to signal that certain drugs are relatively good value for money—has not been consistent with disease management strategies that target compliance. 29,34,35 Indeed, in recent years, payers have been raising financial barriers by increasing patient cost sharing of virtually all pharmaceuticals, ostensibly to economize health care resources. 27 Between 2003 and 2007, average tiered co-payments on brand-name and generic drugs increased by 20% or more. 20,36 Perhaps the fact that so few disease managers coordinate their compliance programs with value-based insurance design has more to do with payers not instituting such policies than lack of coordination on the part of disease managers.
Second, for disease management to demonstrate cost savings or cost-effectiveness of compliance programs, they must be able to identify avoidable adverse health outcomes, such as hospital admissions and emergency room visits, with adequate pharmacy and medical claims data at their disposal. 33 Therefore, a suggestion for evaluating the cost-saving potential of a compliance program would be in terms of inpatient hospitalization days and emergency department visits, because these measures enable “number needed to decrease” analysis. 37 Further, ideally, to evaluate the cost-effectiveness potential of a compliance program entails measurement of incremental cost-effectiveness, that is, comparing the costs and effectiveness of a compliance program to one that does not target compliance. In both instances, measurement of cost savings and cost-effectiveness, inclusion of control groups is necessary because pre–post studies are potentially confounded by environmental changes unrelated to the specific interventions. 18
However, as shown in our survey and also reflected in the literature, at present there appears to be a lack of consistent application of evidence-based protocols to identify noncompliance and to promote compliance. This may change with continued institutionalization of accreditation programs, which seek to establish national standards to evaluate disease management programs. 27
Third, the fee-for-service structure that is still predominant in disease management must be replaced by bundled payment systems that reward value to the patient, rather than services per se.
There have been empirically verifiable instances in which disease management organization strategies have led to improvement in medication compliance rates, consistent with the reports of gains in compliance rates by our survey respondents. 38 Most successes involve a combination of well-designed disease management strategies, rigorously conducted outcomes research, value-based insurance, and bundled payments. 23,39,40,41,42
Footnotes
Author Disclosure Statement
Dr. Cohen, Ms. Christensen, and Ms. Feldman disclosed no conflicts of interest.
This work was supported by a grant from Bayer Schering Pharma.