
Abstract
African American caregivers of the elderly, including those who care for patients with Alzheimer's and other forms of dementia, remain underserved by Medicaid Assistance Programs. The purpose of this exploratory study was to ascertain to what degree participants in an Alzheimer's Association program that primarily targeted African Americans applied for and received Medicaid assistance, in particular for adult day care, in-home care, and respite care. Secondary data from the Delaware Regional Office of the Alzheimer's Association's 2006 Caregiver Survey of 38 caregivers were reviewed using descriptive, chi-square, and logistic regression analysis. Results indicate that 20 caregivers applied for Medicaid services, 12 of whom were approved. However, 18 caregivers did not apply for Medicaid mainly because they perceived that they would not qualify for benefits, without investigating their eligibility. Clearly more education is needed in African American communities about the eligibility requirements and benefits of Medicaid Assistance Programs because services such as adult day care, in-home care, and respite care have been shown to reduce some of the burden, stress, and strain associated with caring for elderly patients with Alzheimer's dementia. However, a multisystem approach should be used in the outreach and education processes. Finally, the Medicaid application process should be streamlined to make it less cumbersome. More financial and support services are needed by African American caregivers of Alzheimer's care recipients. (Population Health Management 2012;15:174–180)
Introduction
Despite efforts made over the years at outreach and to educate underserved communities about their eligibility for Medicaid Assistance, many African Americans, including those with Alzheimer's and other forms of dementia care recipients, remain underserved. 5 A study by Li et al 7 found that, although 80% of the study participants who were elderly care recipients may have been eligible for Medicaid, only 29% were enrolled in 1 or more of the programs. Additionally, a study by Pezzin and Kasper 8 found that as many as 45% of all elderly in the lowest income categories do not participate in Medicaid programs. According to Coogle, 5 African American caregivers generally do not consider formal health care resources to be a priority support option. Instead, many choose to rely on the resources that exist within the family system, creating a trend toward underutilization of available services and resources. 5,9 But Medicaid participation can significantly reduce the burden, stress, and strain often associated with caregiving by serving as an important vehicle for increasing formal service use for African American Alzheimer's dementia patients. 10 However, if their participation rates in Medicaid Assistance Programs are to increase, more culturally relevant, targeted outreach and educational strategies are needed for both care recipients and their caregivers, who are more likely to submit the application for Medicaid on their behalf. 5,10
Qualifying for 1 or more of the Medicaid programs is essential for African American Alzheimer's patients because their caregivers, when compared to their white counterparts, have been shown to have fewer financial resources with which to provide care. 9,11,12 Because African American caregivers of the elderly are more likely to be younger and still engaged in the workforce, 9,12 the use of adult day services, which have been shown to reduce caregiver burden, role strain, and stress, would provide much-needed support. 13 Without the financial assistance and support services that HCBS Waiver Programs provide, these caregivers are at risk of jeopardizing their ability to continue to provide quality care to their loved ones because of increased financial burden, physical and emotional stress, and eventually, “burnout.” 1 Unfortunately, in spite of the well-established need, many African American caregivers still are not motivated to submit applications for Medicaid assistance on behalf of their care recipients, primarily because of the perception that they will not meet the required financial criteria. Other perceptions also exist, such as the application is too difficult to complete, the process is too time consuming, and they will lose all of their assets including their homes. The important point is that misperceptions continue to persist among this at-risk population despite the education programs and outreach strategies that have been developed over the years to provide services and resources to African American and other underserved communities. 14
This study examined African American caregivers' perceptions about the obstacles they faced when accessing Medicaid Assistance Programs, and the reasons why some caregivers and their care recipients, though in need, chose not to apply for the programs.
Methods
This small exploratory study used secondary data from self-reported questionnaires administered by the Delaware Regional Office of the Alzheimer's Association staff for its 2006 Caregivers Survey. The research team reviewed only the completed surveys of a convenience sample of 38 caregivers who were caring for individuals diagnosed with Alzheimer's dementia, and who were receiving services from the Alzheimer's Association through a federal Administration on Aging (AoA) Demonstration grant. The 3-year AoA grant (2004–2007) established a program to provide education and resources to primarily African American families in Delaware who were struggling to cope with the challenges of dementia, especially those who lived in sparsely populated and underserved areas of the state and those encountering early onset (younger than 60 years of age) dementia. By the end of the funding year in June 2007, the program had served more than 2000 families by providing education, early memory/awareness screenings, counseling, referrals, respite activities, and financial assistance to families as they applied for long-term assistance.
Data collection
The Alzheimer's Association staff designed the self-reported questionnaire with input from the research team. The 27-item scale was first examined by professional staff in the Alzheimer's Association to help increase face and content validity, 15 and then pilot tested with a small sample of program participants to eliminate potentially confusing wording and to ensure clarity. Prior to conducting a Cronbach's alpha, 10 items were eliminated from the scale: The 7 questions to which caregivers could provide more than 1 answer were removed, along with the 2 questions to which they could provide a qualitative answer, and the 1 question that asked about their program attendance. The alpha coefficient of 0.808 for the reduced 17-item scale suggests the scale was reliable.
The first part of the survey requested information on caregivers' race/ethnicity, sex, and relationship to the care recipients. Questions 1 to 13 asked about the application and approval processes, the specific types of services they had applied for (ie, nursing facility, home care, adult day care, overnight respite), the length of time and number of attempts it took before receiving a decision, whether they received help with the application, and their experience with the application process. Questions 14 to 19 asked about the frequency with which caregivers used the Medicaid services, the usefulness of the services, and their involvement in a support group. Questions 20 and 21 asked about their attendance in the agency's programs and their perceived usefulness of those programs. Questions 22 and 23 asked about the biggest challenges that caregivers faced and the 1 service they believed would make their lives easier. Questions 25 to 27 were directed only to caregivers who did not apply for Medicaid and asked why they did not apply, what services they would use if they had Medicaid, what informal services they currently had, and the biggest challenges they faced as caregivers. (The survey instrument is available from the author upon request.)
First, descriptive analysis was conducted on the 27-item scale. This was followed by chi-square analysis to determine whether there was a difference between the variables of caregiver sex and Medicaid application rate. Finally, logistic regression was conducted on the variables of caregiver sex, caregiver relationship to care recipient, and Medicaid application rate to predict whether female caregivers were more likely to apply for Medicaid than male caregivers and whether children were more likely than spouses and other caregivers to apply for Medicaid.
In the fall of 2006, the program director sent a letter to the 45 AoA program participants who were receiving financial assistance, inviting them to participate in the program's Caregiver Survey at an upcoming meeting. The letter explained the purpose of the survey, which was to better understand the obstacles that caregivers were encountering during the Medicaid application process, and informed those who were unable to attend the meeting that they would receive a telephone call to assess their interest in completing the survey at a later date. The 11 participants who attended the meeting completed the survey. The other 34 received follow-up calls from the director and 1 additional staff member. Some participants were unable to be contacted after 2 or 3 follow-up calls and others declined to complete the survey when reached. As a result, 27 surveys were administered by telephone. The staff members read the questions and recorded the answers as they were provided. SPSS analytical software (IBM, Chicago, IL) was used and the data were examined using descriptive, chi-square, and logistic regression analyses.
Results
Medicaid applicants
Of the 38 caregivers, 20 indicated that they had applied for Medicaid. Fourteen of the caregivers identified adult day care as the service that most often triggered their application, while 6 said it was in-home or respite care. See Table 1 for demographic characteristics of the caregivers and Table 2 for the Medicaid application outcomes. The small sample size necessitated that the caregiver categories be collapsed into dichotomous variables “parent” and “nonparent.” Logistic regression was not able to predict whether the caregiver's relationship to the care recipient influenced the likelihood of submitting an application to Medicaid; for example, whether children are more likely to submit applications than spouses. Because 16 of the caregivers were female, the researchers anticipated an effect related to the sex of the caregiver. However, logistic regression analysis was not able to determine whether the caregiver's sex influenced the likelihood of submitting an application to Medicaid. Finally, logistic regression analysis also was unable to predict whether participation in support groups or other Alzheimer's Association programs influenced caregivers' likelihood of submitting applications to Medicaid on behalf of their care recipients. Table 3 contains the regression results for predicting Medicaid application rates.
Variables: caregiver sex, caregiver relationship to care recipient, participation in support groups, and participation in Alzheimer's Association programs in predicting the rate of caregiver application for Medicaid on behalf of care recipients.
Significance was measured at the P<0.05 level. Caregiver relationship was collapsed into the dichotomous variables child and nonchild. The variables of attendance at Alzheimer's Association programs was collapsed into the variable attend or not attend.
Application and approval processes
Table 4 contains more details on the application and approval processes. Most of the caregivers described the directions for completing the application as either “clear, easy to follow” or “somewhat clear, with minimal confusion.” Only 1 said that the directions were “very confusing, very unclear.” Two caregivers, who checked the “other” category, added that the directions “needed some clarification,” and “it takes too long, we need help now.” Caregivers were asked to describe the application process and could choose more than 1 answer. Eight indicated that the process was “too long,” “required too much documentation/too many records,” and was “frustrating.” Some also noted that the application process was “too complicated,” “sort of confusing,” and had a “long waiting period.” Only 1 caregiver said the process was “not difficult.” Eight caregivers said they received help with the application and 12 acknowledged that they received no assistance. When specifically describing the application directions, most caregivers indicated that they were “clear, easy to follow,” and “easy,” while some said they were “sort of confusing” and “too complicated.”
Non-Medicaid applicants
For the 18 caregivers who did not apply for Medicaid, the top 2 reasons for not submitting an application were “I thought we would not qualify” (selected by 10 caregivers) and “did not know about process” (selected by 3 caregivers). Five of the caregivers also selected the “other” category; 3 of those indicated that they “did not know about Medicaid.” One person chose the category “decided to postpone [the application],” 1 said that her father [the care recipient] “did not want to sell the house,” and another said that they were “waiting for a final prognosis of Alzheimer's [dementia] from the care recipient's doctor.”
Caregivers' participation in support groups
Study results indicated that the majority (33%–87%) of caregivers did not participate in a support group. The most common reason given for not participating in a support group was “time conflicts,” followed by “no one to care for loved one,” “not interested,” and “would not benefit.” None of the caregivers chose “no transportation.” Three of the caregivers indicated that they “did not know that support groups were available.”
Perceived obstacles
All 38 study participants were provided a list of 10 obstacles and asked to select and rank the 3 that they perceived to be most challenging as caregivers. Figures 1 and 2 present the obstacles identified by caregiver subgroups. The subgroup of caregivers who were not receiving Medicaid assistance includes caregivers who applied for Medicaid but were denied, or had applications pending approval at the conclusion of the study, and those who did not apply for Medicaid.

Obstacles that caregivers perceive as most challenging by subgroup: Caregivers whose care recipients receive Medicaid. ADLS, activities of daily living.
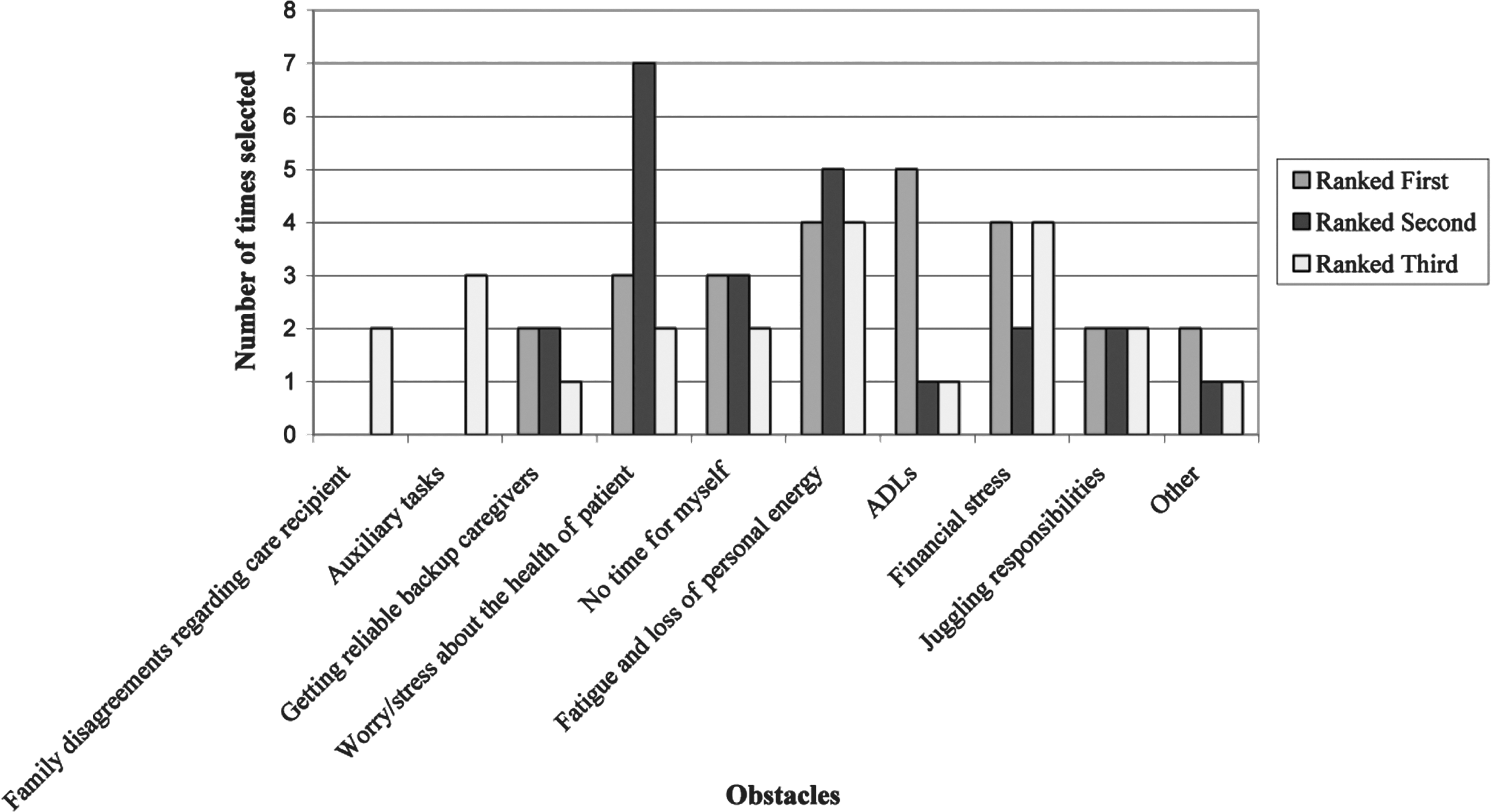
Obstacles that caregivers perceive as most challenging by subgroup: Caregivers whose care recipients do not receive Medicaid. ADLS, activities of daily living.
Expressed need for Medicaid-related services
The 12 caregivers who had applied for Medicaid and received approval were asked to identify 1 service that would make it easier for them to care for their loved ones. The 3 services that were most frequently identified were respite care, adult day care, and financial assistance. The 18 caregivers who did not apply for Medicaid were asked what services they thought they would use if they had Medicaid assistance. They could choose more than 1 service from a list that included in-home care, adult day care, and respite care. Adult day care was selected 11 times, overnight respite care was selected 10 times, and in-home care was selected 8 times. In addition, 5 of the caregivers indicated that they would use all 3 services, and 3 thought they would use 2 of the services. The caregivers who did not apply for Medicaid also were asked what informal services they currently had to support them in their caregiving role. Four indicated that they were receiving respite help from family members at least once a week, 3 said that they were receiving occasional respite (at least once a month), 4 said they had daily paid caregiver support, and 8 indicated that their care recipients attended adult day care.
Discussion
This results of this study help to identify and reconfirm some of the reasons why African American caregivers of Alzheimer's dementia care recipients continue to underutilize Medicaid Assistance Programs for which they may be eligible. They also highlight some of the obstacles these caregivers face that negatively affect both their physical health and mental well-being.
One of the most meaningful findings of the study was the reason many caregivers gave for not applying for Medicaid assistance for their care recipients: They thought they would not qualify for the services. Although this finding is unsettling, it is neither surprising nor unusual for a population who, because of a history of racial discrimination, has a high degree of mistrust for government systems such as Medicaid Assistance Programs. 16 Additionally, for those fortunate enough to own a home, the fear of losing it is real, given that the Medicaid process requires a great deal of financial documentation to determine eligibility. The majority of the caregivers who did not apply for Medicaid simply perceived that they would not meet the eligibility requirements. What is most troubling about this particular finding is that the caregivers' perception was determined without any investigation to determine their eligibility. Because the data instrument did not request income data, the researchers were unable to verify the accuracy of this perception. Future studies should include income as a variable. However, because African American elderly represent one of the poorest groups in the United States, 11,17 it is quite possible that more of the caregiver families in this study may have qualified for Medicaid assistance, had they applied. Using a multisystem approach similar to the one developed by Boyd-Franklin, 18 service providers (eg, social workers, nurses), particularly those who practice in the area of gerontology, can help African American families better understand the requirements and application process for Medicaid Assistance Programs. They can use systems that traditionally have been deemed trustworthy in African American communities, such as faith institutions and primary care physicians, for continuous outreach and education. They also can partner with social organizations such as fraternities, sororities, masons, and community centers, and utilize local radio and cable television stations to educate the community.
A second meaningful finding was the caregivers' description of the application process. Most of the applicants described the process as “too frustrating,” “too long,” and “requires too much documentation/too many records.” While the application itself does not seem to be difficult to complete, the process is perceived to be both cumbersome and lengthy. Service providers can advocate for Medicaid Assistance Programs to streamline the process and reduce the amount of paperwork that is currently required. Quarless Kingsberry and Thibault 19 suggest that, depending on size, every state Medicaid office should develop stakeholder task groups that include staff, service providers to the elderly, caregivers, social workers, nurses, and other key informants, such as policy makers, who can recommend concrete ways to streamline Medicaid application and eligibility processes. In addition, service providers can be more proactive by conducting culturally relevant outreach to educate underserved communities, especially those that are urban and rural, about Medicaid Assistance Programs and helping families with the application process from start to finish. A study by Li et al 7 found a dramatic increase in Medicaid enrollment when social workers assisted elderly care recipients and their families with the application process. In particular, social workers and nurses who are employed in health and behavioral health settings can serve as vital links, within agencies and in communities, to caregivers to help increase their success in accessing and utilizing Medicaid Assistance Programs.
A third and important finding was the expressed need for Medicaid-related services by both subgroups of caregivers. The caregivers who were receiving Medicaid services identified respite care, adult day care, and financial assistance as their most important needs. The caregivers who were not receiving Medicaid identified adult day care, overnight respite care, and in-home care as their top 3 service needs. Service providers should make a stronger effort to link African American caregivers with the services that are currently available in their states and local communities. They should advocate for more affordable adult day care and respite services, more well-trained respite providers, and more financial resources to subsidize care for poor and moderate-income caregivers. For example, they can partner with agencies that serve the elderly to advocate for increased funding for Lifespan Respite, “a coordinated system of accessible, community-based respite care services for caregivers and individuals regardless of age, race, ethnicity, special need or situation.” 20
A fourth, though not surprising finding, was the low rate of caregiver participation in support groups. The majority of caregivers (33/38) did not participate in a support group. This finding is corroborated by previous studies that show African American caregivers of the elderly have lower participation rates in support groups than their white counterparts. 21 The top 2 reasons given by caregivers for not participating in support groups were “time conflicts” and “no one to care for loved one.” But support groups have been shown to provide those who care for persons with Alzheimer's dementia with a network of individuals who understand their dilemma, offer empathetic ears for the physical and emotional challenges they are experiencing, and provide a rich exchange of resources that can help alleviate some of the burden, stress, and strain associated with caregiving. 22,23 Service providers must make conscious and deliberate efforts to help African American caregivers see the benefits they can obtain from support groups. With the explosion of technology, caregivers who have time conflicts, have no one to care for their loved ones, lack transportation, or are too fatigued to attend support groups (which are generally held in the evenings) can be presented with the option to participate in virtual groups via the Internet or the telephone. 24,25 Although African American caregivers rarely participate in support groups, when presented with a forum to discuss caregiving burden, stress, and strain, they may welcome the opportunity to share their experiences and form support networks. In fact, Jones-Cannon and Davis 21 found that African American study participants were inclined to use focus groups as if they were support groups. This finding further highlights the need for support and treatment groups that are offered during various times of the day and run simultaneously for both caregivers and care recipients who are able to participate.
Finally, the researchers had anticipated that both sex and caregiver relationship would influence Medicaid application rates. They hypothesized that women caregivers and children caring for parents would be more likely to apply for Medicaid assistance than caregivers who were caring for spouses/partners or other relatives. This study did not reveal a strong relationship between the variables. Future studies with larger randomized samples may uncover a statistically significant effect between the variables.
Limitations
There were several limitations to this study. First, the small sample was limited to 1 specific AoA program in a small state located in the northeast region of the country. Future researchers working with small programs should consider partnering with a few agencies in different locations, but with participants who have similar demographic characteristics, as a strategy to increase the sample size to at least 100. Second, because of time constraints to complete the survey and, to some degree, the inexperience of the staff and research team, the survey did not undergo sufficiently rigorous testing for validity and reliability. Given the small number of program participants who were available for the study, the researchers decided to limit the number of caregivers who pilot tested the survey. Increasing the sample size would eliminate this problem in future studies. Additionally, because the survey was constructed internally, an item analysis should have been conducted to eliminate those items with low correlations, which would have increased the questionnaire's internal consistency. The authors suggest that anyone considering replicating the study conduct an item analysis before administering the survey. Likewise, the staff should have received specific training in interviewing techniques, which would have increased the study's inter-rater reliability. Third, some of the questions required caregivers to answer retrospectively, and they may not have remembered accurately. This could have affected the validity of the findings. Additionally, questions on income and age were excluded but may have shed light on eligibility for Medicaid as well as on differences, if any, between younger and older caregivers. Finally, a question on the length of time caregivers had been caring for recipients may have uncovered differences between new caregivers and those who have been caring for a longer period of time. Because of these and other limitations, much caution must be exercised in generalizing any of the findings to other African American caregivers of Alzheimer's dementia care recipients.
Conclusion
Although this study was small and exploratory, it uncovered interesting findings that can be of value to service providers and other practitioners who work with African American caregivers of Alzheimer's and other dementia care recipients. They also may help the Medicaid Assistance Programs, in particular the HCBS-Waiver Programs, develop more culturally relevant, targeted outreach strategies to increase the participation rate of African American caregivers in their programs. 5,10 The financial assistance and support services that these programs provide can significantly reduce the burden, role strain, and stress that these caregivers experience. 13 Without the resources, their financial burden and physical and emotional stress are likely to increase, 1 which can result in their inability to care for loved ones at home in spite of their willingness and cultural values. This can lead to increased institutionalization of African American elders, which, in the long run, will be more costly to both families and society. Given that the number of Alzheimer's dementia patients is projected to almost triple by the year 2050, 1 and that the disease appears to affect African Americans disproportionately, 2 it makes good sense to identify strategies that will enhance the policies and services that have been developed to prevent institutionalization of the elderly. The study's results also provide data that can be used by Medicaid Assistance Programs to help streamline its application process; for example, reducing the number of documents that are required. In addition, the results support previous studies that provide empirical evidence that utilizing service providers such as social workers to assist elderly caregivers and recipients with the application process can increase their enrollment in the programs. 7 Overall, the study's results provide data that Medicaid Assistance Programs can use to improve service delivery to what continues to be a very vulnerable and at-risk population; African American caregivers of Alzheimer's dementia care recipients. However, there is need for further investigation of this topic.
Footnotes
Acknowledgments
The authors thank Edna Ellet and Annie Young, former administrators of the Delaware Regional Office of the Alzheimer's Association; Blair Thibault, MSW, Tiffany Reed and Deborah Powell, student interns; and, Judith Quarless, MA, William Bretzger, MA, and Linda Mayer, MSW, MA for their assistance during various phases of the research project and manuscript preparation.
Author Disclosure Statement
Dr. Quarless Kingsberry and Ms. Mindler disclosed no conflicts of interest.