
Abstract
Adherence to recommended preventive services and immunizations in adults is suboptimal and often associated with socioeconomic status, race, and access to care. The aim of this study is to evaluate adherence in a cohort without these barriers to ascertain realistically optimal adherence rates and to examine remaining barriers among relatively advantaged individuals. Specifically, it employed a sample of 6889 patients presenting for executive health care from 2005 to 2009. Adherence varied across colorectal cancer screening (79%), mammography (89%), cervical cancer screening (91%), tetanus immunization (82%), and pneumococcal vaccination (62%). Multivariate logistic regressions revealed that age, education, alcohol use concerns, and being married were positively associated with adherence to certain services. Individuals without the usual barriers to care have variable, less-than-ideal rates of adherence to preventive services, which correlate with some health behaviors and demographics. Understanding the predictors of adherence may inform quality improvement processes aimed at optimizing disease prevention. (Population Health Management 2012;15:65–70)
Introduction
Yet many eligible people fail to receive recommended preventive services and immunizations. 2,7,8 Despite awareness efforts, such as Healthy People 9 and the publication and dissemination of USPSTF and the Centers for Disease Control and Prevention (CDC) recommendations, 10 –12 adherence to these recommendations remains highly variable and, for some populations, remarkably low. Screening rates for cancer are variable and often suboptimal. Adherence to USPSTF colorectal screening guidelines is between 25% and 50% 13 –16 ; adherence rates to mammography and cervical cancer screening usually range between 39%-86% and 57%-75%, respectively, 15,17 –20 although some have found higher adherence. 21 Adherence to age-appropriate CDC recommendations approximates 60% for tetanus and pneumococcal vaccinations (with large variations depending on socioeconomic, racial, and ethnic characteristics), with comparable or lower rates for influenza vaccination. 22,23
Underutilization of preventive services may reflect several barriers that are rooted in social structure, clinical practice, and personal circumstances. 18,19 Although some authors have examined provider practices, 17,24 –26 most have emphasized patient characteristics as key determinants. These include age (with screening adherence clustering around the ages identified in recommendations), 14 comorbid conditions (eg, diabetes), 16,27 body mass index (BMI), health behaviors (eg, smoking), 16,21 stress and major life events, 16,20 and social-structural considerations, such as socioeconomic status (SES), racial/ethnic disparities, and access to care. 13,15,19,20,28,29 Accordingly, many examinations of preventive service utilization have focused on lower income or minority individuals. 8,15,18,28,30 –32
This article assesses the utilization of preventive services by patients at the other end of the socioeconomic spectrum; those who are relatively privileged. Specifically, it examines a sample of patients presenting for a first visit to an executive health program. Patients presenting to these programs are usually of relatively high SES, predominantly white, and have excellent access to care. 33,34 Consequently, because of its selective nature, this population is relatively free of some of the main risk factors for low adherence to the preventive service recommendations outlined. Despite study of less-advantaged populations, little is known about prevention and screening among these individuals. If adherence to preventive service recommendations among these patients is still suboptimal, then factors other than access, coverage, SES, or minority status should be considered as the enduring risk factors for underutilization of preventive services. Such factors may include health beliefs and behaviors, education, patient values and preferences, or other as yet unidentified systemic factors. Furthermore, if adherence to such services is less than ideal in a relatively advantaged population, then goals for optimal adherence may require adjustment for consideration of realistic maximal levels. What are the realistically optimal levels of adherence to preventive service recommendations as evidenced by this relatively privileged population? What are the personal and lifestyle barriers that remain after selecting out many of the commonly identified barriers to preventive services?
The aim of this study is to determine the baseline adherence rates to several evidence-based preventive and screening recommendations in patients presenting for a first visit to an executive health program. This means that it examines adherence to preventive services prior to enrollment in the executive health program; thus, the authors are not evaluating the impact of this program per se on adherence. Doing so allows for controlling, via selection or inclusion, several confounding or explanatory variables, and measuring the prevalence and correlates of adherence to preventive service recommendations in a population for whom access should not be restricted by economic or educational factors.
In addition to evaluating rates of adherence to selected USPSTF recommendations for preventive services, the authors also assessed how such rates differ by education level, sex, and other sociodemographic factors, and examined the interrelationships between adherence rates, individual characteristics, and other health-related behaviors.
Methods
Sample
Data were extracted for all consecutive patients who had not previously been seen in the Executive Health Program at the Mayo Clinic, Rochester, Minnesota between January 3, 2005 and December 28, 2009, who offered informed consent for the use of their information for research purposes, and for whom this information was available in the record (total sample size = 6889). The study was approved by Mayo Clinic's Institutional Review Board.
Data
Data included information on screenings and immunizations, anthropometric information, health behaviors, and demographics. Patient information was extracted from the electronic medical record. This record consisted of the comprehensive intake note by physicians, immunization modules, and patient provided information (self-reported standard forms filled by new patients online or on paper prior to the first visit). The data included only patient information at entry; that is, we examined preventive service utilization and patient status prior to care initiation in the Executive Health Program. Medical records from outside institutions usually are obtained and electronically scanned after relevant information is documented in the appropriate part of the medical record. Typically, the dates of the last preventive interventions are verified in 3 steps: (1) patient-reported on the intake forms, (2) face-to-face by the clinical assistant rooming the patients on their first visit, and (3) by the examining physician.
Dependent variables
All dependent variables were binary composite measures, coded such that 0 = nonadherent and 1 = adherent. Preventive services were selected that are recommended for adults, rated grade A or B by USPSTF or recommended by the Advisory Committee on Immunization Practices, applied to most patients without significant restriction to special populations, and which were documented sufficiently in the medical record. Recommended preventive services that met these criteria and were selected for analysis included colon, breast, and cervical cancer screening, and tetanus and pneumococcal vaccination. Examples of recommended preventive services that were not selected include: (1) bone mineral density, because the indications for testing in women > 60 were not easily extractable from the medical record and may have variable documentation across providers; (2) herpes zoster vaccination, because of repeated vaccine shortage from the manufacturer that may lead to false low adherence; (3) influenza vaccination, because it is often given at the workplace or retail stores and not well documented in the charts; and (4) recommendations pertaining to sexually transmitted disease, because they are restricted to patients at risk and will affect a small proportion of this cohort.
For all dependent variables, cutoffs covered up to and including the maximum time between screens/immunizations (eg, up to and including 10 years since the last colonoscopy) to ensure relatively conservative estimates of nonadherence.
Colorectal screening was a binary composite measure, derived from data on colorectal cancer screening measures (date of last screening) and age, and constructed according to USPSTF guidelines. Specifically, the variable was limited to those ages 50–74 years, and coded such that 1 (representing adherence to USPSTF guidelines) meant having a colonoscopy within the last 10 years and/or a sigmoidoscopy or barium enema screen in the last 5 years; 0 represented not having any of these screens within the respective time frames.
Mammography was derived from data on the date of last mammogram, sex, and age. Specifically, the variable was limited to women ages 50–75 years, and coded such that 1 represented those who had had a mammogram within the last 2 years (adherent) and 0 represented a last mammogram more than 2 years prior.
Cervical cancer screening was a binary composite measure derived from data on Pap tests and demographic information. This measure was limited to women ages 21–65 years, and coded such that 1 (meaning adherence) represented a Pap test within the last 3 years and 0 indicated a test outside that range.
Tetanus vaccination was a binary composite measure derived from immunization data and was coded such that 1 meant the individual had received tetanus immunization (with or without diphtheria and/or pertussis) within the last 10 years.
Pneumococcal vaccination was a binary composite measure derived from information on immunizations and age. It applied to individuals age 65 and older, and was coded such that 1 represented an individual who had ever had a pneumococcal vaccination and 0 represented not having received a pneumococcal vaccination.
Independent variables
BMI was extracted from records and used untransformed.
Alcohol concerns, included as a health attitude/behavior, was a dummy/indicator variable that relied on screening questions from the CAGE questionnaire, 35 included in the patient provided information, indicating whether the individual had reported that other people had expressed concerns about his/her drinking or that he/she had personal concerns.
Smoking, included as a health behavior, was a dummy/indicator variable representing current smokers (1 = current smoker; 0 = have quit/never smoked).
Psychological stressors were extracted as a summed index of 6 possible life stressors (range: 0 to 6), asked routinely upon first visit to the program. These pertained to whether the person's relationship status changed in the past 12 months; ever feeling afraid at one's home; ever being fearful for one's own safety; having been physically abused; having been sexually abused; and having been emotionally abused. This is similar to stress scales validated in prior literature. 36
Demographic covariates included age, sex, marital status, and education.
Analysis
Analyses were completed using StataSE, version 11 (StataCorp LP, College Station, TX). The authors first used descriptive statistics to characterize the sample in terms of demographics, health status, and health behaviors, and then assessed the extent to which patients were adherent to USPSTF and CDC recommendations for colorectal cancer, breast cancer, and cervical cancer screens, and vaccinations for tetanus and pneumococcus. Next, to examine the patient factors predicting adherence, the authors performed logistic regressions of adherence to each screening/immunization on variables, available in patient records, which have been identified as potential barriers/facilitators to service utilization in prior literature (demographics, BMI, stress, and health behaviors).
Results
Table 1 displays descriptive statistics for the sample. As expected, the sample was relatively older, better educated, and reported relatively few stressors compared to the general population.
Total N = 6889
Valid percents (percent of non-missing cases for each variable).
Figure 1 displays adherence rates; which were fairly high, yet variable.
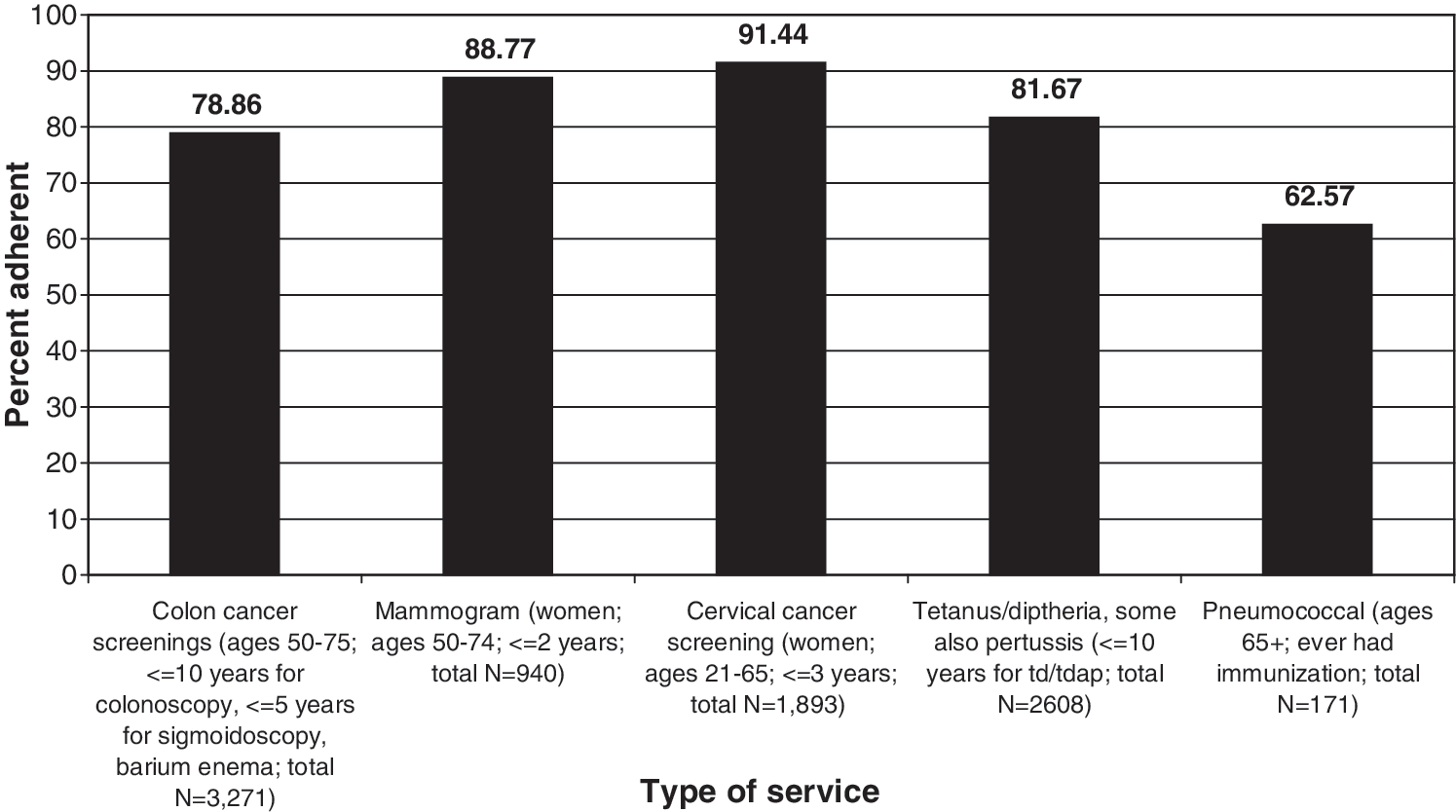
Percent adherent to preventive service recommendations upon presentation to an executive health program.
Among individuals for whom each screening or immunization was age/status appropriate, we examined the effects of commonly identified barriers to preventive services (eg, BMI, health behaviors, stress, demographics) on adherence to recommendations. The results of these analyses are in Table 2. Increasing age was a significant predictor of adherence to recommendations for colorectal cancer screening and pneumococcal vaccination, with each incremental year associated with 0.2 to 0.4 greater odds for adherence.
Each model is applied only to those groups for whom recommendations are relevant. * P < 0.05, ** P < 0.01, *** P < 0.001.
BMI, body mass index; OR, odds ratio; SE, standard error; TD, tetanus-diptheria vaccine; TDaP, tetanus-diptheria-acellular Pertussis vaccine.
Education and alcohol use concerns were positively associated with adherence for colorectal cancer screening. Being married was a positive predictor of adherence to mammography. BMI and current smoking were negatively associated with adherence to cervical cancer screening. Current smoking was negatively associated with adherence to tetanus vaccination. Alcohol use concerns were positively associated with adherence to pneumococcal vaccination.
Discussion
The present study examined the prevalence and correlates of patient adherence to USPSTF and CDC recommendations for preventive services among a sample of individuals newly presenting to an executive health program. Because studies focusing on barriers to the use of such services tend to emphasize vulnerable populations, this study examined a relatively advantaged group to examine (1) realistic optimal rates of adherence and (2) the remaining barriers/facilitators of adherence among a population with generally optimal access to care.
In general, there was relatively high adherence to colorectal, breast, and cervical cancer screening, and for tetanus immunizations, as compared to prevalence rates reported in existing literature. However, pneumococcal immunization had rates of adherence to recommendations that were similar to typical rates reported in the literature. Moreover, at best, adherence rates tended to peak between 80% and 92%. This suggests that even among relatively advantaged individuals who have relatively few barriers to care (and who are seeking preventive care at a tertiary center), prior adherence to preventive services guidelines may reach an upper threshold of approximately 90%. In addition, underutilization of pneumococcal vaccinations represents a continued, avoidable, and unmet need among adults older than 65 years of age—even for individuals with relatively great access to care. This is especially worthy of attention given that pneumococcal vaccinations (or tetanus immunizations, for that matter) are relatively undisruptive to daily life and scheduling when compared to, for instance, colorectal screenings. As such, and given the relatively low discomfort associated with these immunizations (versus the screenings we analyzed), the adherences rates for them may, speculatively, reflect provider practices or low perceived need among patients (rather than patients' wishes to avoid immunizations). Future research should examine other immunizations (eg, influenza) that may be more normalized in patients' experiences and practice.
Multivariate regression results suggest that, even after removing many of the socioeconomic, cultural, and other barriers identified in the existing literature, systemic/organizational and health behavioral factors remain that impede utilization of preventive services. In some cases, as age increased, so did the likelihood of utilization. This indicated that the nature of most testing recommendations (which are based on age above most other factors) may create a systemic pattern of time-based adherence. In other words, patients and/or providers may see the adherence time windows (eg, 10 years for colonoscopy) or age categories (eg, beginning at age 50) as an acceptable time frame for utilizing a service, with the odds of adherence greater as patients' ages approach the edges of these markers. 14
In terms of health behaviors, alcohol use concerns positively predicted adherence for colorectal screening and pneumococcal immunization. Although the present data do not allow pinpointing the reasons, the authors speculate that self-identified or other alcohol concerns may reflect an environment of generalized health concern/consciousness (considering that it is a measure of concerns, rather than amount or frequency of drinking). Further analyses are needed to examine this association among similarly advantaged populations. Smoking behavior, however, may have signified a lack of concern for health consciousness, a wish to avoid clinician “lecturing,” or a point of discriminatory recommendations by providers, as it was negatively associated with Pap testing and tetanus immunization, consistent with previous literature on other populations. 21 Also consistent with findings in other studies, the association here between high BMI (overweight/obesity) and lower adherence to cervical cancer screening may reflect lack of concern by either patients or providers. Finally, being married positively predicted adherence to mammography, suggesting that married women might either have a greater sense of responsibility for their health, or that their spouses may provide greater support or pressure to obtain mammograms.
The strengths of this study include the large sample size and a design that controls for confounding variables and provides a unique view of preventive service adherence in this usually less studied population. Use of a consistent structured patient questionnaire and a consistent patient rooming process provided consistent high yield of some less common behavioral and life-history measures (alcohol use concerns, stressors, vaccine history). The limitations include limited generalizability. Thus, while this study identified patterns in service utilization from which clinicians and researchers can learn, this consecutive sample itself remains unique. Also, the data are essentially cross-sectional, in that they do not follow individuals over time—they capture individuals at initial presentation. Although this helps to limit the focus to their utilization prior to admittance to the executive health program, it also would be useful to examine similarly advantaged populations over time to understand individual trajectories of preventive service utilization, and how life events at any given time may affect their utilization patterns. Despite coding conservatively, it is plausible that adherence was underestimated as a result of obtaining data retrospectively from the medical record: recall bias and poor documentation of services provided outside the institution could be present. Nevertheless, data were verified by using patient provided forms, patient interview by the clinical assistant, and patient interview by the physician. Also, when available, outside records were used to document receipt of preventive services.
Despite its limitations, this study takes a distinctive viewpoint on the problem of preventive services utilization that can persist even beyond relative socioeconomic equality/prosperity. Guidelines recommending these services must have better patient representation to inform how the guidelines are to be applied and provide platforms for implementation.
Lastly, patients may not adhere to recommendations based on their own values, beliefs, and personal context. This specific latter case of lack of adherence, if patients are well informed, should not be considered an indicator of poor quality of care. Nevertheless, it is fair to assume that the values of participants in this study, who are self-selected patients seeking an examination focused on prevention and early detection, are consistent with wanting these services. Thus, low rates of adherence highlight either suboptimal care or a poorly designed infrastructure for the administration of these services. Recognition and documentation of the reasons for patient nonadherence are important in the era of physician scorecards and pay-for-performance reimbursement methods.
Conclusions
Advantaged individuals disposed favorably to preventive care and without most of the usual barriers had almost perfect adherence to some preventive service recommendations and less-than-ideal rates of adherence to others. Although certain demographic and health-related correlates were present, further examination of the characteristics of each preventive service, patient preferences, and other predictors of adherence in this population may inform innovative quality improvement processes for optimizing disease prevention.
Footnotes
Acknowledgments
This research was supported by the Mayo Clinic Division of Preventive, Occupational, and Aerospace Medicine and the Mayo Foundation for Education and Research. The content herein is solely the work of the authors and does not necessarily represent the official position of the Mayo Clinic.
Author Disclosure Statement
Drs. Shippee, Nabhan, Kermott, Hagen, Montori, and Murad, and Ms Mullan disclosed no conflicts of interest.