
Abstract
Chronic obstructive pulmonary disease (COPD) affects approximately 7% of Americans. COPD impacts productivity and forces 1 in 5 employees ages 45–65 years old to retire prematurely. Our objective was to quantify the direct and indirect costs of COPD in an employed population in the United States. A retrospective analysis using Thomson Reuters MarketScan commercial claims and Health and Productivity (HPM) databases (2000–2007) identified employees (ages 18–65 years) with ≥ 1 COPD medical claim, ≥ 6 month insurance eligibility pre and ≥ 12 months post diagnosis, and ≥ 12 months HPM data post diagnosis. COPD subjects were matched to non-COPD subjects using propensity scores to create a comparison group with similar characteristics. Differences in medical and pharmacy utilization and productivity (absence and short-term disability [STD] days) were examined using negative binomial regression, and cost differences using Heckman selection models. A total of 27,612 COPD patients were matched in a 1:1 ratio to 825,884 non-COPD patients; 80% were ages 36–65 years, and 59% were male. COPD employees had about twice the rate of emergency department visits and hospitalizations compared to non-COPD employees (P<0.0001). The rate of absence and STD days was approximately 1.5 times higher (P<0.0001) compared to non-COPD employees. Yearly direct and indirect expenditures were higher ($3609 and $909, respectively; P<0.0001) for COPD versus non-COPD employees. Excess utilization and associated costs of COPD to employers was quantified. By understanding these costs, employers may evaluate disease management programs and treatment to improve outcomes for employees with COPD. Improved treatment options may reduce the direct and indirect costs of COPD. (Population Health Management 2012;15:267–275)
Introduction
Aggregate costs associated with COPD have been well documented. The total economic burden of COPD in 2010 was estimated at $49.9 billion, including $29.5 billion in direct health care expenditures, $8.0 billion in indirect morbidity costs, and $12.4 billion in indirect mortality costs. 8 COPD is ranked sixth among the top 10 costliest diseases to employers; in 1999, the cost of COPD to employers was estimated at $65 per eligible employee per year, excluding presenteeism costs, with 43% of costs attributable to absence (ABS) and disability. 9 A systematic literature review published in 2006 identified 13 studies that presented comprehensive cost estimates of direct costs associated with COPD, with COPD-attributable cost estimates ranging from $2700 to $5900 annually and excess cost estimates (compared to non-COPD patients) from $6100 to $6600 annually; however, few studies were identified that reported on work productivity-related COPD costs in the United States. 10 COPD significantly impacts productivity in working individuals affected, as about half of persons with COPD report that their ability to work is limited by their disease. 1 Although these national estimates present the economic burden of COPD to employers, a focused examination of the direct and indirect costs associated with COPD, and specific cost drivers, among a nationally-based US employed population remains inadequately addressed in the published literature.
The primary objective of this study was to estimate total direct and a subset of indirect expenditures associated with COPD among an employed population in the United States. The authors also sought to identify drivers of direct medical expenditures (eg, emergency department [ED] visits, hospitalizations, outpatient visits) and indirect expenditures (ABS and short-term disability [STD] hours per month). A secondary objective was to identify employer segments with the highest prevalence of COPD and to examine the variation in direct and a subset of indirect expenditures by employer segment.
Methods
Study population
The authors conducted a retrospective study using the Thomson Reuters Health and Productivity Management (HPM) and the Thomson Reuters Commercial Claims and Encounters (CCAE) databases, linking individuals across these 2 data sets. Employees aged 18 to 65 years with at least 1 medical claim for COPD (International Classification of Diseases, Ninth Revision [ICD-9]=490.XX, 491.XX, 492.XX, 494.XX, 496.XX) at any time during 2000–2007 in any of the CCAE databases were identified for preliminary study inclusion. The date of each subject's first visit during 2000–2007 with a qualifying ICD-9 code for COPD was termed the study “index date.” Subjects were required to have continuous enrollment in the CCAE for at least 6 months prior to and at least 12 months subsequent to the index date. Subjects also were required to have prescription drug benefit eligibility and available drug data throughout the study period. Enrollment in the HPM database for at least 12 months following the index date with eligibility for either ABS or STD also was required for study inclusion. Less than 5% of the study sample had both ABS and STD data. Thus, separate samples were created for those who had STD data and those who had ABS data to examine the impact of COPD on productivity.
Subjects who met all of the eligibility criteria were evaluated against a comparator group, which was selected from a population with the following characteristics. The comparator population comprised employees ages 18–65 years who were selected from the CCAE databases from among enrollees with no medical claims for COPD at any time during 2000–2007. Eligible employees were required to have continuous enrollment in the CCAE for at least 18 months to match the 6 months pre and 12 months post index date inclusion criteria for the study group. The index date for each potential employee in the comparator population was set at 6 months into that employee's enrollment period. Comparator participants were required to have prescription drug benefit eligibility and available drug data throughout their entire study enrollment period. Employees comprising the comparator population were required to be enrolled in the HPM database for at least 12 months subsequent to the index date. Consistent with eligibility requirements for COPD subjects, comparator population employees were required to be eligible for ABS or STD for a minimum of 12 months following the index date in the HPM database, and separate samples were created in a similar manner to that described for the study population.
Study outcome measures
Primary study outcomes included overall and COPD-related ABS and STD hours per month, overall and COPD-related medical and pharmacy utilization, and overall and COPD-related direct and indirect expenditures (amount paid). Total ABS and STD hours per month were determined by summing the total hours per week and normalizing to 30 days. The mean number of STD and ABS days also was determined. Direct expenditures and utilization were first classified as either medical or pharmacy. Using the Milliman Health Cost Guidelines, medical cost and utilization categories included hospitalizations, ED visits, office visits, laboratory/diagnostic tests, outpatient surgeries, durable medical equipment, and other services. Pharmacy utilization and associated costs included all medications (orals and injectables), including COPD-related medication, for the study group. Indirect costs were estimated using hourly wage data with industry groupings, which was obtained from the US Bureau of Labor Statistics (
Type of employment industry for each employee was defined according to the categories designated in the MarketScan database, as follows: oil/gas, manufacturing of durable goods, manufacturing of nondurable goods, transportation, retail services, financial services, and other services. Risk score was calculated using the Chronic Illness and Disability Payment System (CDPS). 11 CDPS is a diagnosis-based risk assessment model that has been used in prior studies to adjust for patient comorbidity burden 12 –14 ; the CDPS assigns each participant to at least 1 of 67 possible medical condition categories based on diagnosis codes and to 1 of 16 age/sex categories. Because the CDPS model originally was designed for use with a Medicaid population, the CDPS was recalibrated for the commercial population using the full 2000–2007 MarketScan population for use in this study.
Statistical analysis
Propensity score methodology was used to create a matched sample of employees without COPD (the comparator group) to those with COPD (the study group). 15,16 Given the inherently different characteristics between the study and comparator groups in terms of disease severity, propensity scoring allowed the creation of groups that were as similar as possible, thereby reducing the bias associated with these differences. Propensity scoring was performed with logistic regression models using the presence/absence of COPD as the dependent variable. Demographic, clinical, and employment characteristics were used in the propensity scoring to create the matched samples. These variables included the following: employee age, sex, risk score, index year, type of health plan (managed care, fee for service), number of enrollment months following the index date, geographic region, type of employment industry, and presence of selected comorbid conditions. COPD and comparison population employees were then scored using the resulting logistic equation that weighed together the characteristics described, providing a propensity score between zero and 1.0. Comparison population employees were matched to employees with COPD in a 1:1 ratio using propensity scores in a greedy matching algorithm.
To compare adjusted differences for primary study outcomes between the COPD and comparison groups, the “double robustness” approach was used, in which variables used to create the propensity-matched samples also were used in the adjusted analysis. As an alternate to Poisson regression, a more robust negative binomial model was used to estimate adjusted differences between the COPD and comparison groups for all count-based outcome variables in the study, such as ABS and STD hours per month, and medical and pharmacy utilization. Negative binomial models were used because Poisson regression assumes the response variable has a Poisson distribution, with its mean equal to its variance. 17 However, in many cases, the observed variance is greater than the mean, which results in dispersion and non-robust estimates. Negative binomial regression addresses this issue and is a robust alternative to analyze count data. 18 The adjusted incident rate ratios (IRRs) were reported for each regression. Medical cost data exhibit unique statistical properties that require the use of appropriate econometric techniques. 19 Cost data are strongly right-skewed and have a significant percentage of zero-cost observations. Many methods have been developed to deal with these unique properties of cost data. Most studies use the transformed expenditures data. Logarithmic transformation is the common statistical procedure used, but this transformation does not solve the zero-clustering issue. The maximum likelihood Heckman selection model simultaneously takes into account the likelihood of having positive health care expenditures and estimates the relationship between independent covariates and logarithm of cost, 20 and has been used previously in analyses of health care costs. 21 Thus, the Heckman selection model with logarithmic transformation was used in this study for indirect and direct expenditure analysis.
The primary dependent variable was the group membership variable indicating whether an individual was in the COPD group or the comparator group. Independent variables included in these models were as follows: age (stratified as 18–25, 26–35, 36–45, 46–55, 56–65); sex; CDPS risk score; type of health plan (managed care, fee for service, or other); number of enrollment months following the index diagnosis claim (index date for the comparison group is 6 months into their CCAE enrollment period of at least 18 months); US geographic region; type of employment industry (based on categorization in the MarketScan database); and presence of common comorbidities in the general population (ie, asthma, congestive heart disease, depression, diabetes, dyslipidemia, hypertension, rheumatoid arthritis). All study analyses were conducted using SAS, version 9.2 (SAS Institute Inc., Cary, NC).
Results
In the HPM database (N=1.7 million), the overall proportion of employees with COPD was 2.9% and did not vary greatly by type of industry, ranging from 2% (oil/gas/mining, transportation, finance, and other services) to 4% (manufacturing of durable goods). Among employees with COPD, the majority worked in manufacturing (45%) or transportation (39%). Overall, 27,612 employees with COPD met all inclusionary criteria, and an initial comparator group of 825,884 employees without COPD met original comparator population inclusion criteria. Baseline characteristics of the COPD and comparator groups, prior to and subsequent to propensity score matching, are shown in Table 1. Prior to propensity score matching, employees with COPD were significantly older, more likely to be female, and had a greater chronic disease burden than the comparison group. Demographic and clinical characteristics of propensity-score matched employees with COPD (n=27,612) and the comparator group (n=27,612) were similar (Table 1). Mean age was 44 and 40% of the cohort overall was female. The most prevalent comorbid conditions among the study population were dyslipidemia and hypertension.
Note that index year was not included as a variable in the propensity equation.
CDPS, Chronic Illness and Disability Payment System; CHD, congestive heart disease; COPD, chronic obstructive pulmonary disease.
All and COPD-related medical and pharmacy utilization for employees with COPD and the comparator group are shown in Table 2. Employees with COPD had higher utilization in all categories.
Utilization shown represents per subject per month, adjusted for age, CDPS risk score; type of health plan; number of enrollment months following the index diagnosis claim, US geographic region; type of employment industry; and presence of comorbidities that include asthma, congestive heart disease, depression, diabetes, dyslipidemia, hypertension, and rheumatoid arthritis.
CDPS, Chronic Illness and Disability Payment System; COPD, chronic obstructive pulmonary disease; IRR, incident rate ratios.
Adjusted differences in total and COPD-related direct expenditures for employees with COPD and the comparator group are included in Table 3. Adjusted mean total direct expenditures per year were higher for employees with COPD versus comparator employees. The largest contributors to the difference in total direct expenditures were all prescriptions, physician visits, and other medical services. COPD-related accounted for $365 in direct costs for employees with COPD. Among employees with COPD, the largest contributors to COPD-related direct expenditures were inpatient hospitalizations and COPD prescriptions.
Expenditures shown are per study participant per year. Expenditures were adjusted for age, CDPS risk score; type of health plan; number of enrollment months following the index diagnosis claim, US geographic region; type of employment industry; and presence of comorbidities that include asthma, congestive heart disease, depression, diabetes, dyslipidemia, hypertension, and rheumatoid arthritis.
CDPS, Chronic Illness and Disability Payment System; COPD, chronic obstructive pulmonary disease.
Mean total and COPD-related direct expenditures by industry type are shown in Table 4. Across all industries represented, adjusted differences in direct total costs were significantly higher for COPD subjects (P<0.0001, all comparisons). Adjusted costs were highest among workers employed in durable goods manufacturing, and lowest for those in the transportation industry.
COPD, chronic obstructive pulmonary disease.
ABS hours and STD days were significantly higher among employees with COPD than among comparator workers (Fig. 1). Employees with COPD had 20% more total mean ABS hours than comparator employees (IRR=1.21, P<0.0001), and 53% more total mean STD days (IRR=1.53, P<0.0001). Adjusted differences in indirect total and COPD-related expenditures were significantly higher among employees with COPD and are depicted in Figure 2. Among employees with COPD, indirect costs accounted for 61% of total (direct+indirect) COPD-related costs measured in this study.

Adjusted differences (all and COPD-related) between absence hours and STD days (per study participant per month) for COPD and comparator groups. COPD, chronic obstructive pulmonary disease; STD, short-term disability.
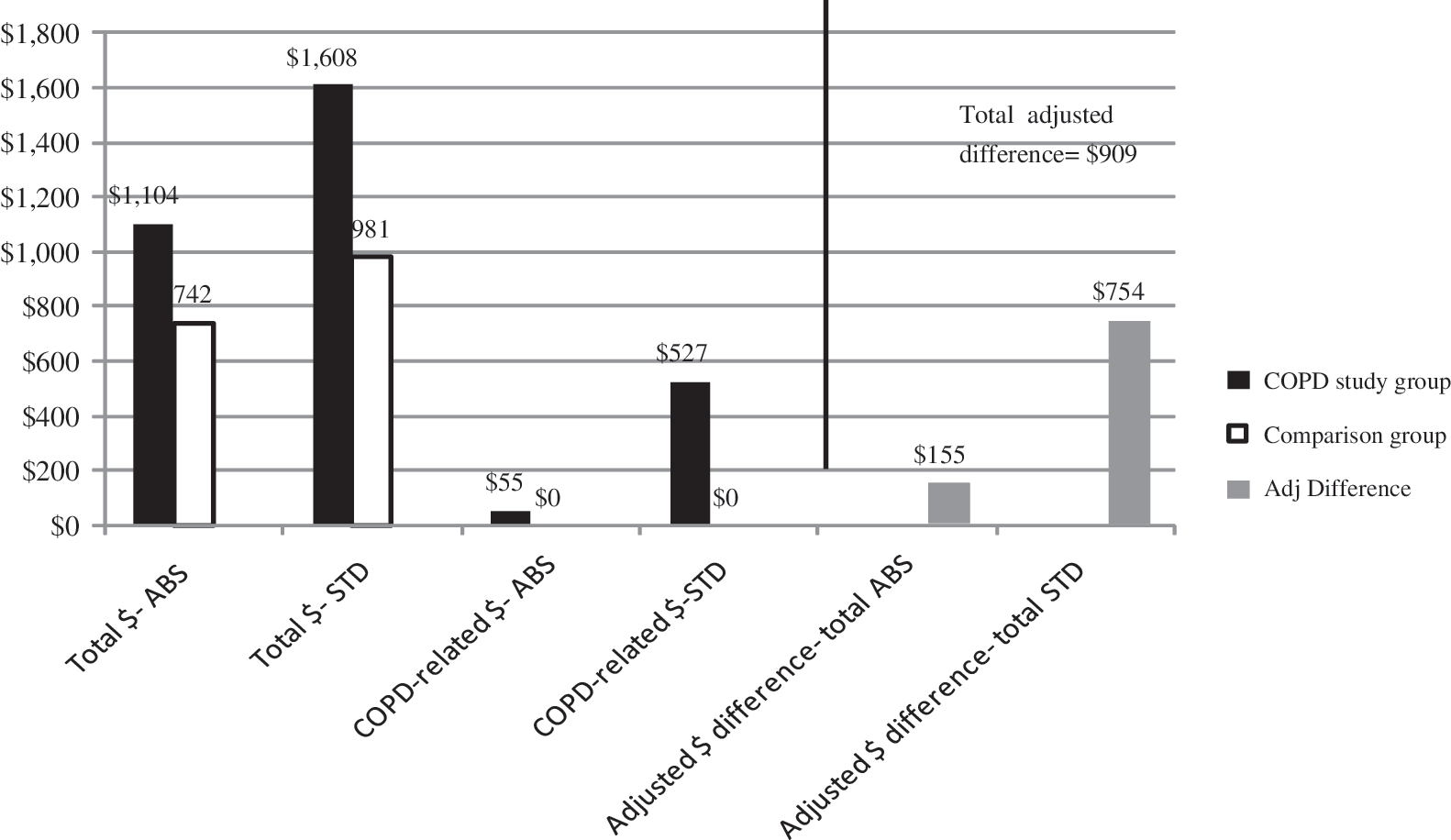
Adjusted differences in total and COPD-related indirect expenditures for COPD subjects and comparison patients (per member per year). ABS, absence; COPD, chronic obstructive pulmonary disease; STD, short-term disability.
Discussion
Among an employed US population, COPD was associated with about twice the rate of all-cause ED visits and hospitalizations as compared to the experience of a sample of non-COPD employees with similar baseline demographic and clinical characteristics. The rate of ABS and STD days was about 1.5 times higher among employees with COPD. Both direct and indirect yearly expenditures were significantly higher for employees with COPD. This study, therefore, presents unique findings about the specific drivers of direct and indirect costs for a COPD population and how they compare to a non-COPD population. To our knowledge, previous research has not been conducted to examine these drivers in detail prior to the current study.
COPD is costly to employers, especially in the manufacturing and transportation industries. Annual total direct expenditures were $3609 higher for employees with COPD as compared to those without COPD, and annual indirect costs measured (ABS and STD) were $909 higher among employees with COPD. Successful COPD management of affected employees will become increasingly important as employees continue to work longer and the US workforce ages. Previous research has shown that COPD disease management programs can lead to improved health-related quality of life, 22,23 decreased health care utilization, 22 –24 and lower health care costs. 24 Improved disease treatment options, in conjunction with prevention-based smoking cessation initiatives, 25 may be valuable management options for employers, particularly those in manufacturing or transportation because, at least in the current study, these industries had the most employees with COPD. Initiatives such as these eventually may result in a partial offset of some portion of the COPD-related costs measured in this study.
Goetzel and colleagues identified COPD as ranking sixth among the 10 costliest medical conditions to employers in 1999, using the Thomson Reuters HPM database for 1997–1999. 9 Goetzel estimated a yearly per eligible employee cost of $65 attributable to COPD; this was comprised of $37 in total health care payments, $23 in total ABS payments, and $5 in total STD payments per eligible employee in 1999 US dollars. Notably, among the top 10 conditions identified by Goetzel and colleagues, COPD ranked among the highest in terms of ABS/STD proportion of total direct plus indirect costs, at 43%. The current study was conducted with more recent data (2000–2007) and thus, as expected, higher costs were observed. However, this study found that lost productivity accounted for 61% of total direct and indirect COPD-related costs, suggesting a trend toward increasing indirect costs associated with COPD over time. Neither study includes indirect costs associated with presenteeism or long-term disability, thereby underestimating the total employer cost burden of COPD among employees.
Three recent studies reporting indirect costs of COPD in the United States were identified, using different data sources and study methodologies. The NHLBI calculated indirect costs to be $20.4 billion in 2010 US dollars, including costs resulting from loss of work productivity associated with morbidity and early mortality among COPD patients. 8 Darkow et al studied 1349 employees with COPD (mean age=52 years) from 2001–2004 who were matched to similar employees without COPD. These authors found that employees with COPD were significantly more likely to utilize short-term, long-term, or any disability; associated costs were $8559 for COPD versus $5443 for non-COPD employees. 26 Halpern and colleagues used US subject responses to the Confronting COPD in North America and Europe survey of working-age COPD subjects, who reported losing about 19 days of work annually as a result of COPD, or almost $2000 per patient/year. 27 Finally, data from the National Health and Nutrition Examination Survey III were used to estimate that in 2004, COPD resulted in almost $10 billion in productivity loss in the United States. 28
A comparison of our study's results to prior research indicates that direct medical costs were higher among other studies compared to what we observed. Many published studies of COPD direct costs are focused primarily on an older Medicare population, making comparison to a younger employed population difficult. Not surprisingly, studies conducted among Medicare patients aged 65 years or older indicate higher attributable costs for patients with COPD. 29 Nurmagambetov et al used the Thomson Reuters MarketScan database to estimate the direct yearly medical costs for COPD at $1138 for patients ages 35‐65 years during 1999–2003. 30 Another study evaluated 6738 California (mean age=56 years) and 18,017 Florida (mean age=60 years) Medicaid patients age 40 years or older during 2001. This study estimated that the mean excess cost (comparing total medical costs for COPD patients to costs incurred by a matched non-COPD patient group) attributable to COPD per patient was $6500 for California and $5200 for Florida Medicaid; among COPD patients, mean costs attributable to COPD were similar ($2200 and $2300 per patient, respectively). 31 Tinkelman and colleagues examined direct costs incurred by COPD patients aged > 45 years old and estimated total mean monthly health care costs for COPD patients (all expenditures) were 4–6 times higher than matched controls without COPD, at $2556 for patients 45–54 years old, and $2650 for those 55–64 years old. 32 In the current study, total all-cause direct costs were $6910 for COPD versus $4434 for employees without COPD. These findings, consistent with the published literature, 31 –33 suggest that COPD employees also incur higher non-COPD-specific direct expenditures compared to those without COPD, as reflected by excess cost estimates. A 2006 systematic review identified 13 published studies estimating the direct costs of COPD, with COPD attributable costs estimated at $2700–$5900 annually, and excess cost estimates (compared to non-COPD patients) of $6100–$6600 annually, in 2005 US dollars. 10 Notably, the authors of this review acknowledge that the wide degree of variability of cost of illness estimates is not surprising, given different data sources, particularly those limited to working-age patients versus those conducted among elderly Medicare beneficiaries, different time periods, inclusion of different cost components, and disparate methodologies. 10
Finally, in our study, the overall proportion of employees with COPD was 2.9%, and is somewhat lower than published estimates of the US population as a whole (7%). 1 National estimates represent all COPD patients, including the elderly, and COPD prevalence increases with age. 4 Our study looked at an employed population, which is likely to be both younger and healthier than the entire US population. In addition, our study identified newly diagnosed patients (using a 6-month washout period), while US prevalence estimates are based on the presence of a COPD diagnosis regardless of the duration of disease.
Limitations
Although this study provides important information about the economic burden of COPD in the US working population, several study limitations should be considered when interpreting the results. A retrospective claims-based study has advantages for evaluating costs and utilization experienced by patients in a “usual care” setting. However, selection bias resulting from the assignment of patients to study groups based on the presence or absence of COPD may play a role in our study's findings. Employees with COPD in this study were identified using the presence of 1 or more claims with an ICD-9 code for COPD, whereas other studies have required 2 or more claims with an ICD-9 code for inclusion. We included patients with 1 COPD-related ICD-9 code because our patient population was working age and thus was considerably younger than most COPD study cohorts; this enabled us potentially to capture employees with milder disease. In addition, a recent sensitivity/specificity analysis of the number of COPD-specific claims required for subject identification concluded that using the criteria of 1 or more claims with a COPD ICD-9 code yielded acceptable sensitivity and specificity. 34 Nevertheless, we cannot ascertain whether some employees in our study with only 1 COPD-specific claim actually may not have had a diagnosis of COPD. Similarly, we included patients with an ICD-9 code of 490.xx (bronchitis, not specified as acute or chronic); although used in prior studies, 28,35 –37 the inclusion of this diagnostic code is somewhat controversial and may have erroneously included some patients without COPD. 38 However, as other investigators have hypothesized, 37 it may be that a proportion of study patients identified solely via ICD-9 code 490.xx represent a patient group with early COPD. Patients with a COPD diagnosis are likely to have a smoking history, and may have more comorbid conditions and an overall lower health status than patients without COPD. In fact, results presented in Table 1 confirm that, prior to propensity score matching, non-COPD patients were healthier than COPD patients, as evidenced by a comparison of risk scores and the prevalence of comorbid conditions. We employed propensity scoring methodology to minimize the differences in clinical and demographic characteristics between study groups. Although this propensity score methodology controlled for these differences to some extent, it is possible that factors that were unavailable for analysis may have impacted our study's findings. Second, many variables were unavailable for study inclusion, including the stage and duration of COPD, patient racial/ethnic background, and patient body mass index. Because our study included patients with medical and pharmacy benefit coverage, it may not be representative of the uninsured population. Our study did not evaluate the impact of comorbid asthma on COPD-related costs within our study population. Finally, although our study provides important information on both direct and indirect costs associated with COPD, because we evaluated only typical working-age persons, our study's findings pertaining to direct costs may not be applicable to persons older than 65 years of age, who represent a sizable proportion of the prevalent COPD cases in the United States.
Conclusion
COPD clearly poses an economic burden to employers, especially in the manufacturing and transportation industries. Effective COPD management strategies may include increased access to existing treatment options as well as new treatment options, removal of COPD treatment barriers, and strategies to promote both smoking cessation and earlier patient diagnosis. Improved COPD treatment access may help to partially offset some of the direct and indirect costs of COPD reported here. By understanding the economic burden of COPD, employers can make decisions about investments in treatment options, disease management, and prevention programs for COPD.
Footnotes
Author Disclosure Statement
Mr. Doyle and Dr. Frech-Tamas are employees of Novartis Pharmaceuticals Corporation, and both own stock and stock options in Novartis. Ms. Van Den Bos, Mr. Halford, and Mr. Tan are consultants with Milliman, whose work on this study was funded by Novartis Pharmaceuticals Corporation. Dr. Nair and Dr. Ghushchyan report no conflicts of interest. This study was funded by a grant from Novartis Pharmaceuticals.
Acknowledgments
The authors wish to acknowledge Jenifer Wogen, M.S., of MedMentis Consulting LLC, who provided medical writing services and assistance with manuscript preparation. Ms. Wogen was compensated by Novartis Pharmaceuticals Corporation.