
Abstract
This study aimed to assess the impact of a nationwide German diabetes mellitus disease management program (DMP) on survival time and costs in comparison to routine care. The authors conducted a retrospective observational cohort study using routine administration data from Germany's largest sickness fund to identify insured suffering from diabetes in 2002. A total of 95,443 insured with type 2 diabetes mellitus who were born before January 1, 1962 met the defined inclusion criteria, resulting in 19,888 pairs of DMP participants and nonparticipants matched for socioeconomic and health status using propensity score matching methods. This is the first time propensity score matching has been used to evaluate a survival benefit of DMPs. In the time frame analyzed (3 years), mean survival time for the DMP group was 1045 days vs. 985 days for the routine care group (P<0.001). Mean daily hospital and total costs (including DMP administration and medical costs) were lower for the DMP group in the case of deceased insureds (92€ vs. 139€ and 122€ vs. 169€, respectively) as well as for censored observations (6€ vs. 7€ and 12.9€ vs. 13.4€, respectively). Mean daily drug costs were slightly lower for deceased insured in the DMP group (difference 0.6€), while no identifiable difference was found for censored observations. In this study, insured who were enrolled in a DMP for diabetes mellitus in the German Statutory Health Insurance showed a significant benefit in survival time. They also incurred lower costs compared to propensity score matched insured in routine care. (Population Health Management 2012;15:241–247)
Introduction
The present study uses data routinely collected in the German disease management program (DMP) for diabetes mellitus that was offered by the largest sickness fund in the German Statutory Health Insurance (SHI), the BARMER. Quality assured DMPs were implemented in a nationwide rollout in the German SHI in 2002 for 6 diagnoses. In 2010 more than 3 million patients were enrolled in DMPs for diabetes mellitus nationwide. Hallmarks of the programs are treatment according to evidence-based guidelines, implementation of information technology support, the central role of a DMP doctor in ambulatory care, a patient-centered approach that supports patient self-management, and financial incentives for doctors, patients, and sickness funds. Quality assurance measures include reminders, physician feedback and benchmarking reports every 3 months, physician education, compulsory quality improvement circles, and public reporting of results. Feedback and benchmarking reports are individualized for each physician. Routine data collection is standardized on a national reporting sheet. Cross-sectional and longitudinal analyses are risk adjusted and allow subgroup analyses. Programs are operationalized via contracts between the Physician Association for Ambulatory Care (Kassenaerztliche Vereinigung) and sickness funds. The programs must be accredited by the Federal Agency for Insurance (Bundesversicherungsamt). Evaluation of the programs is mandatory. Earlier evaluations of the programs have demonstrated that they are able to impact the provision of care and improve quality of life for patients who suffer from diabetes. 10,11
The aim of the current study is to assess the effectiveness of a nationwide diabetes mellitus DMP in the primary care setting in the German SHI compared to routine care (RC). Comparisons of survival time of patients with different treatment options for diabetes mellitus or its complications are available from various countries, yet most studies center on the comparison of specific treatment regimes, such as peritoneal vs. hemodialysis, or investigate trends in all-cause or complication-specific mortality in patients with diabetes. 7,12 To evaluate a DMP more broadly for patients with diabetes, we performed a survival analysis of patients with type 2 diabetes mellitus who were enrolled in a diabetes DMP (DMP group) compared to patients with type 2 diabetes mellitus in routine care (RC group), using a propensity score matching approach. This is the first time propensity score matching has been used to evaluate a survival benefit of DMPs. Our hypothesis was that patients enrolled in a diabetes mellitus DMP have a longer survival time compared to diabetic patients in RC. We also analyzed the effect of DMP enrollment on hospital costs and drug costs as well as on total costs, including a lump sum for additional administration and medical necessitated by DMPs.
Methods
Disease management program and routine care
The type 2 diabetes mellitus DMP was accredited by the Federal Agency for Insurance to comply with the legal requirements of a quality-assured DMP. It comprises regular consultations at 3-month intervals independent of acute problems, diabetes-specific physical examinations, lab tests, physician and patient education, discussion of patient-specific treatment goals, specialist referrals if required, documentation of all medical findings in a standardized documentation routine, treatment according to evidence-based treatment recommendations, and regular reminders for physicians and patients. Patients enroll into the programs on a voluntary basis. There are financial incentives for physicians and patients for enrollment.
Patients in RC did not receive any specific intervention. RC comprised ambulatory and inpatient care whenever needed or deemed appropriate. It was not detailed in a special protocol.
Study design
Because all SHI insured (∼80% of the population) in Germany are legally entitled to join a DMP, it was not possible to design a randomized controlled trial for this study. To minimize selection bias in the data, the authors designed a retrospective, nonrandomized study using propensity scores to match the data as recommended in the literature for the evaluation of DMPs. 13,14 In this cohort study, more than 200,000 patients were followed over a 3-year period (2005–2007). All patients were insured by the BARMER sickness fund. Insured patients were stratified into either a DMP group (enrolled in the DMP) or an RC group. Inclusion criteria for both groups are presented in Table 1. Additionally, all insured had to be born before January 1, 1962.
DMP, disease management program; RC, routine care.
Data collection
A database of those insured who were identified as having diabetes was constructed using BARMER administrative claims data for the year 2002. The diagnosis of diabetes was defined as having at least 3 prescriptions for antidiabetic drugs in the year 2002. Of the 234,262 insured identified, 53.44% were female (gender was missing in 1.63% of cases). In all, 95,443 insured (40.74%) met the inclusion criteria; 8475 from this sample were eliminated because of missing values in variables used for matching or because they died in 2008 and there was no information on the number of days spent in the DMP. The remaining 86,968 (19,888 DMP group) insured were matched using a propensity score method to yield of 19,888 pairs (Fig. 1).

Data flowchart.
Statistical analysis
Propensity scores were estimated using a stepwise logistic regression with enrollment into the DMP group (yes/no) as the dependent variable. The propensity score is defined as a subject's probability of receiving a specific treatment conditional on his or her observed covariates at baseline. 13 The following independent variables were included to reflect socioeconomic status: age, sex, and insurance status (employed, retired person, unemployed), as well as health status at baseline captured by the inclusion of drug costs in 2003, hospital costs in 2003, and 8 International Classification of Diseases (ICD) clusters to represent comorbidity in 2003 (quantitative variables entered the model unmodified). All variables were chosen based on reasonable criteria and expert assessment. Meaningful 2-way interactions were taken into account. Because individual patient clinical predictors such as HbA1c or blood pressure are not available at the sickness fund level in Germany, we could not include these variables to adjust for morbidity.
The propensity score attributed to an insured is the individual probability of being in the DMP group considering the initial covariates measured. The propensity score can be used as a matching variable that replaces all covariates with a single scalar. Matching was conducted using Parson's 5→1 method. 15 To assure that the propensity score model is adequate, the balance between the groups was assessed. Standardized differences were computed to examine the degree of imbalance within the matched pairs as well as between the unmatched pairs. A standardized difference of <10% is considered an acceptable degree of balance between groups for a given variable. 16
Hypotheses were formulated before the data were inspected. The testing hypothesis was that there is no difference in survival time between the DMP and RC groups. To test the hypothesis, differences between groups in survival time were compared using a test proposed by Austin. 17 If an insured died, this was considered to be the “event” of interest. An observation was “censored” if the insured was still alive on December 31, 2007, or switched sickness fund, or opted out of the DMP.
Mean daily hospital, drug, and total costs during survival time were considered separately for insured who died and insured whose data were censored because patients who die will accumulate higher costs on average during the last months before death compared to patients who survive. 18,19 Costs were taken from sickness funds claims data. Total costs included hospital and drug costs as well as a lump sum of 180€ per enrolled insured per year to cover administration and medical costs. During the observed time frame, sickness funds received this lump sum payment from the German risk compensation scheme to cover additional medical expenses and administrative activities necessitated by the DMPs. It was calculated as the average amount per insured based on data from several sickness funds.
Matching and statistical analysis was performed using SAS version 9.2 (SAS Institute, Cary, NC) and R Version 2.10.1 (Matching package). 20
Results
Propensity score analysis
After matching, all standardized differences were below 10%, indicating that the propensity score approach matched the data appropriately (Table 2). In addition, all standardized differences of included 2-way interactions were well below 10% (data not shown).
Independent variables that had a significant influence in the stepwise logistic regression and were not dismissed from the model.; **ICD codes are based on hospital diagnosis only.
DMP, disease management program; ICD, International Classification of Diseases; RC, routine care.
Survival analysis
Table 3 provides a summary of the survival data. A proportion of 89.06% of the data were censored. The number of events (deaths) was higher in the RC group than in the DMP group.
DMP, disease management program; RC, routine care.
Figure 2 shows the estimated Kaplan-Meier survival curves. Because the intervention period covered 3 years, the maximum survival time was 1095 days. For the total observation period the survival curve of the DMP group is above the curve of the RC group, indicating that patients in the DMP group have a prolonged survival. Mean 3-year survival time in the DMP group was 1,044.94 (±189.87) days while the mean 3-year survival time in the RC group was 985.02 (±264.68) days. The difference in survival curves is significant at P<0.001.
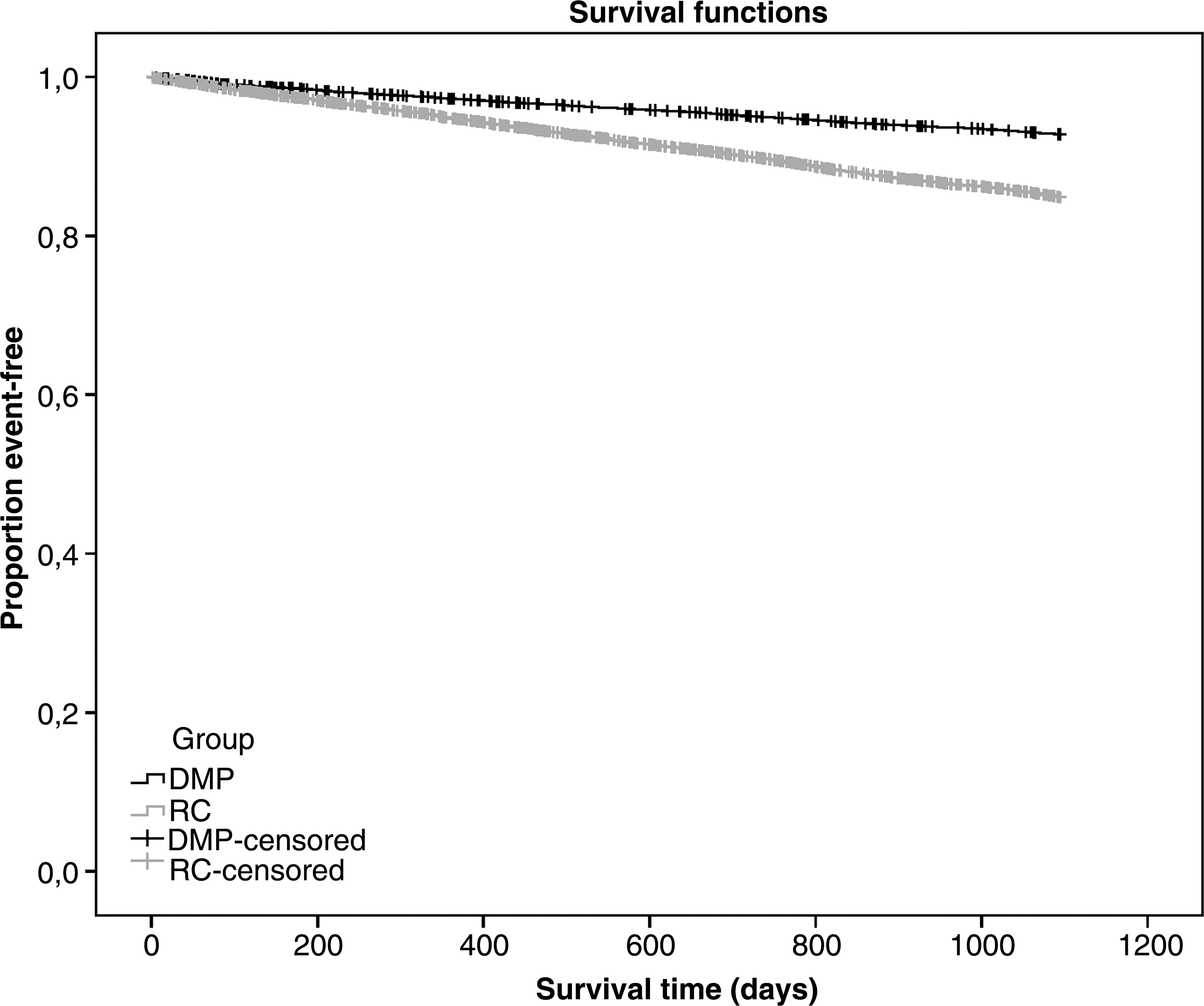
Survival curves.
Cost outcome
Table 4 displays the results for the comparison of mean daily costs for patients in the DMP group to those in the RC group. Mean daily hospital costs were lower for the DMP group for those who died (difference: 47.77€) as well as for censored observations (difference: 1.13€). Mean daily drug costs were slightly lower for deceased insured in the DMP group (difference 0.6€) while no identifiable difference was found for censored observations. Total costs, including the lump sum for administration and medical costs, were lower in the DMP group for deceased insured as well as censored observations (difference: 46.52€ and 0.56€, respectively).
DMP, disease management program; RC, routine care.
Discussion
This study describes the effect of a type 2 diabetes mellitus DMP on the survival time of insured enrolled in the DMP compared to survival times of patients in RC. With a follow-up of at most 3 years we found that—after adjusting for various socioeconomic and health status factors via propensity score matching—patients enrolled in a diabetes mellitus DMP have a significantly longer survival time compared to those in RC. A total of 1,425 (7.17%) insured enrolled in the DMP died; 2,928 (14.72%) insured in the RC group died (P<0.001). This is a reduction of 7.55% in the mortality rate between RC and DMP group in favor of the DMP group. Analyzing survival time, patients in the DMP group lived 59.92 days longer on average compared to those in RC.
There are 2 possible explanations for this difference: (1) patients enrolled in DMP have a lower degree of morbidity and a higher degree of motivation to adhere to treatment regimes compared to individuals who do not enroll in such programs. 21 This so-called selection bias is a common problem with observational cohort studies. To adjust for this bias, we included drug and hospital costs as well as comorbidities as matching criteria to capture differences in severity of morbidity and socioeconomic variables. Matching with respect to patient motivation was not possible because those data were not available. (2) Patients enrolled in DMP received treatment of higher quality compared to RC patients; thus, they had fewer exacerbations, developed fewer complications, and were able to manage their own disease better compared to insured in RC. Therefore, the survival benefit would be related to the high-quality care in the programs. There are a few evaluations that have shown that patients enrolled in diabetes mellitus DMPs in Germany have consistently lower blood pressure and blood sugar levels compared to RC. 22 Additionally, other key parameters such as blood cholesterol levels and smoking cessation rates improve markedly in DMP compared to RC. Evidence from the United States is mixed. However, Thiebaud et al could show that a DMP improved adherence to oral hypoglycemic agents and diagnostic tests in a Medicare population. 23 Two evaluations also suggested an improvement in mortality for patients enrolled in DMP compared to RC. Miksch et al found a significant difference in survival of 3.1% but did not adjust for comorbidities and made no use of propensity score matching. 9 Stock et al used the propensity score matching approach and found a significantly lower mortality rate for patients enrolled in DMP (2.3% vs. 4.7%) but they required the DMP group to be in the program for at least 3 years so that people dying earlier, or switching sickness fund, or opting out the program were not included. 24 The current evaluation is an extrapolation of the analysis by Stock et al, including all patients who died earlier or switched sickness fund.
Despite including all patients, it is not possible with the available data to adequately identify the main reason for the survival benefit. Hence, the survival benefit might be a result of a combination of all factors mentioned.
The economic analysis revealed that insured in the DMP group had consistently lower hospital and total costs (including a lump sum for administrative and medical expenses for DMP participation) per day for both those who died and those who survived. Mean daily drug costs were slightly lower for deceased patients in the DMP group (difference 0.6€) but we found no difference for censored patients. This is remarkable as it is known from economic evaluations of DMPs that hospitalization rates drop within the programs while drug costs rise as a result of better adherence to medications. 25,26 This effect is attributed mostly to the initiation of treatment according to evidence-based treatment guidelines and self-management support. However, overall costs are often lower for patients enrolled in the programs. 27 The reason for the lower drug costs in our evaluation is unclear. Insured with diabetes in RC in Germany tend to be switched to insulin early. Additionally, they may have multiple prescriptions from different doctors. Patients in a DMP, however, may have lower drug costs as a result of frequent revisions to the medical prescription, which is considered to be a key to preventing treatment-related complications in diabetes. 28 Costs for drugs are included in hospital costs in Germany if a patient is treated as an inpatient. We found slightly lower drug costs for deceased patients who, in general, are treated as inpatients before death, which may explain this finding.
Although we used a good statistical tool to minimize bias, this study has a number of limitations that must be addressed. The most important limitation is that of possible selection bias. Because enrollment in a DMP is voluntary, it may be affected by personal characteristics such as motivation for self-management. Analyses hint at differences between DMP and RC insured with diabetes with respect to disease severity, comorbidities, risk factors, and motivation 21,29 ; however, the direction of these differences remains unclear. We used propensity score matching to minimize treatment selection bias from socioeconomic variables and health status. This allows the replication of the characteristics of a randomized controlled trial with regard to these variables. 30 Because the propensity score is a balancing score, the distribution of measured baseline variables will be similar between matched treated and untreated subjects. Moreover, if treatment selection is strongly ignorable, then conditioning on the propensity score can produce unbiased estimates of the treatment effect. 13 However, although randomization will balance, in expectation, both measured and unmeasured variables between treated and untreated subjects, conditioning on the propensity score balances only measured baseline variables between treated and untreated subjects. Therefore, for subjects matched on the propensity score, treated and untreated subjects still may be imbalanced on unmeasured characteristics. 30 This imbalance in unmeasured baseline characteristics can result in a biased estimation of the true treatment effect.
In this analysis, matching with the propensity score approach achieved an accurate balance on the characteristics considered in the model, with all standardized differences being negligible (<10%) after matching. Although matching criteria also were adjusted for comorbidity, we could only rely on the hospital diagnosis. This may lead to an underestimation of morbidity in patients who were not hospitalized. The degree of self-selection that arises with voluntary enrollment has already been discussed. Although health conscious insured may enroll in the programs in higher numbers, insured with low literacy may not be attracted to the programs. Thus, insured with a per se better chance of self-management behavior might be included in the programs, while others with the same comorbidities but less ability to cope with the disease will not opt into the program or drop out. This bias could not be accounted for as no data are available on this issue. This kind of bias might be minimized, however, by the high enrollment rates in some parts of the country. In the North Rhine region, for example, almost 80% of all insured with diabetes are enrolled in the programs. 22
An additional limitation in the analyses of voluntary nationwide opt-in programs is its representativeness for Germany. The BARMER is the single largest fund in the SHI. It operates nationally but has a slightly higher percentage of women compared to the average population. Women often are known to be more active and tend to be more health conscious, which might affect results in favor of the DMP. Another possible bias that could not be accounted for is a difference in physician practices and patient self-care patterns. It would be necessary to address the former cluster randomization at the physician level, which was not possible in this “real-world” study.
Regarding possible regression to the mean, Linden described this effect as a serious problem in the evaluation of US DMPs. 31 As most US DMPs enroll only high-risk patients with high costs, those results are likely to be biased by the regression to the mean effect. But in Germany all insured are legally entitled to join a DMP and there is no selection of high-risk patients. Because of this, we think our propensity score matching was able to remove a possible regression to the mean effect.
If the larger part of the effect on survival is, however, a result of higher quality of care in the programs—which might be caused by better self-management skills of the patients, closer adherence to evidence-based guidelines, or improved secondary prevention—then an even larger effect can be expected within the next years. This applies to diabetes-specific mortality as well as mortality related to diseases for which diabetes or blood sugar level is an important factor that affects prognosis (eg, cardiovascular disease). It is not possible to estimate diabetes-specific mortality with the present data, as we cannot correlate our data with diagnoses from death certificates. Further research is needed to answer this question.
Footnotes
Author Disclosure Statement
Aside from their employment, Ms. Drabik, Mr. Büscher, Mr. Thomas, and Drs. Graf, Müller, and Stock disclosed no potential or actual conflicts of interest.