
Abstract
Virtual wards are a model for delivering multidisciplinary case management to people who are at high predicted risk of unplanned acute care hospitalization. First introduced in Croydon, England, in 2006, this concept has since been adopted and adapted by health care organizations in other parts of the United Kingdom and internationally. In this article, the authors review the model of virtual wards as originally described—with its twin pillars of (1) using a predictive model to identify people who are at high risk of future emergency hospitalization, and (2) offering these individuals a period of intensive, multidisciplinary preventive care at home using the systems, staffing, and daily routines of a hospital ward. The authors then describe how virtual wards have been modified and implemented in 6 sites in the United Kingdom, United States, and Canada where they are subject to formal evaluation. Like hospital wards, virtual wards vary in terms of patient selection, ward configuration, staff composition, and ward processes. Policy makers and researchers should be aware of these differences when considering the evaluation results of studies investigating the cost-effectiveness of virtual wards. (Population Health Management 2012;15:315–321)
Introduction
An important element of any hospital avoidance program is the ability to identify patients at high risk of future unplanned admission to an acute care facility. Unfortunately, doctors, nurses, and case managers do not appear to be able to predict hospital admissions reliably. 11 Furthermore, patients who have multiple emergency admissions in a given year tend to have fewer admissions in subsequent years, even without any intervention—a phenomenon known as “regression to the mean.” 12 Therefore, tools that identify patients who currently are experiencing multiple hospital admissions also are unsatisfactory. 13,14 A more reliable way to identify individuals at risk of future unplanned hospital admissions is to use a predictive risk model. 15,16
In many health care systems, predictive models are currently being used to identify which patients should be offered hospital avoidance interventions. Given that the accuracy of predictive models can be quantified, the crucial questions now are whether these interventions are efficacious, equitable, and cost-effective. 17 One such intervention is the virtual ward (VW) (Fig. 1). 18,19 In 2010, Carlisle reported that over 30 sites had established VWs or were in the process of doing so. 20 Formal evaluation studies are currently being conducted in 6 of these sites: 4 sites in the United Kingdom, and 1 each in Canada and the United States. 21 –24 However, each of the 6 VW study sites has adapted and implemented the intervention somewhat differently.
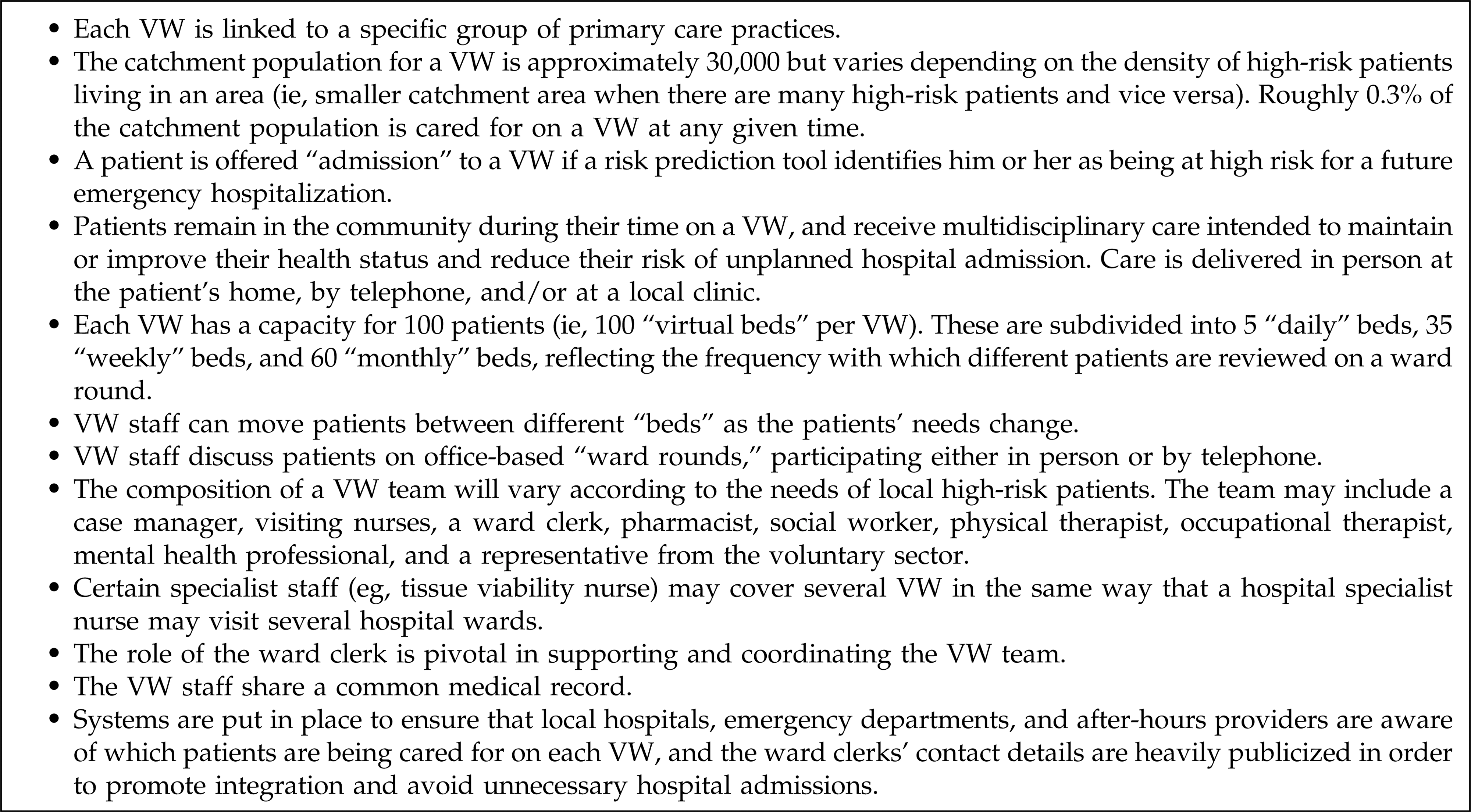
Original Virtual Wards (VW) model. 18
In this article, the authors first review the VW model as it was originally described, and then outline the ways in which VWs are currently operating in 6 study sites. The authors conclude by exploring a wider range of variations to the VW model that researchers and policy makers should bear in mind when considering this type of population health management.
Description of Care Practice
Virtual wards: Original model
VWs are a model for organizing care in the community for individuals in a population who are predicted to be at very high risk of a future emergency hospitalization. 18,19 They build on a long tradition of hospital-at-home schemes, which may be defined as services that provide, “active treatment by health care professionals, in the patient's home, of a condition that otherwise would require acute hospital in-patient care, always for a limited period.” 25
In 2005, a Cochrane review concluded that there was insufficient evidence of so-called “early discharge hospital-at-home” services being cheaper than inpatient care, and recommended that future research should focus on “admission avoidance” hospital-at-home schemes. 26 VWs are an example of this second type of hospital-at-home scheme. Rather than waiting for high-risk people to be admitted to an acute care hospital as an emergency, VWs instead bring the coordination of a multidisciplinary team to the patient in advance in order to deliver intensive preventive care in the community.
How are Virtual Wards being implemented in practice?
Following its implementation in Croydon, England, clinicians and health care managers working in other parts of the United Kingdom and overseas began to adopt and modify the VW model in their local areas. Formal evaluations are currently under way in at least 6 of these sites: Croydon, Devon, Wandsworth, and North Somerset in England, as well as in New York City, New York, and Toronto, Ontario. The authors conducted an online survey in April 2011 to ascertain how VWs are currently operating in these 6 study sites. Table 1 presents the findings, organized according to the taxonomy described by Boaden and colleagues, namely: (1) target population; (2) assessment, care planning, and monitoring of patients; and (3) exit. 30
Information was collected in April 2011 using an online survey tool.
Members of the “core team” spend most or all of their time working with VW patients.
Members of the “wider team” spend less than half of their time working with VW patients.
GP, general practitioner; VW, virtual ward.
As can be seen in Table 1, the original VW model has been modified in a number of ways by the different study sites. For example, in Wandsworth, England, 4 VWs have been established, each led by a general practitioner, known as a “VWGP,” who works full time exclusively with VW patients (Fig. 2). 33 In New York City, the “Hospital2Home” project shares many common features with VWs but, to reflect the high prevalence of homelessness among high-risk patients, the multidisciplinary team includes housing officers, and patients are issued pre-programmed mobile phones to ensure that they can contact the team. 34 Finally, in the Toronto VW project, patients are identified using a predictive model called LACE, which forecasts risk of readmission within 30 days of discharge from hospital. 31 High-risk patients are offered care by a VW team that is led by a hospital physician and includes a range of community-based professionals, which may help improve integration between hospital and community services. 35
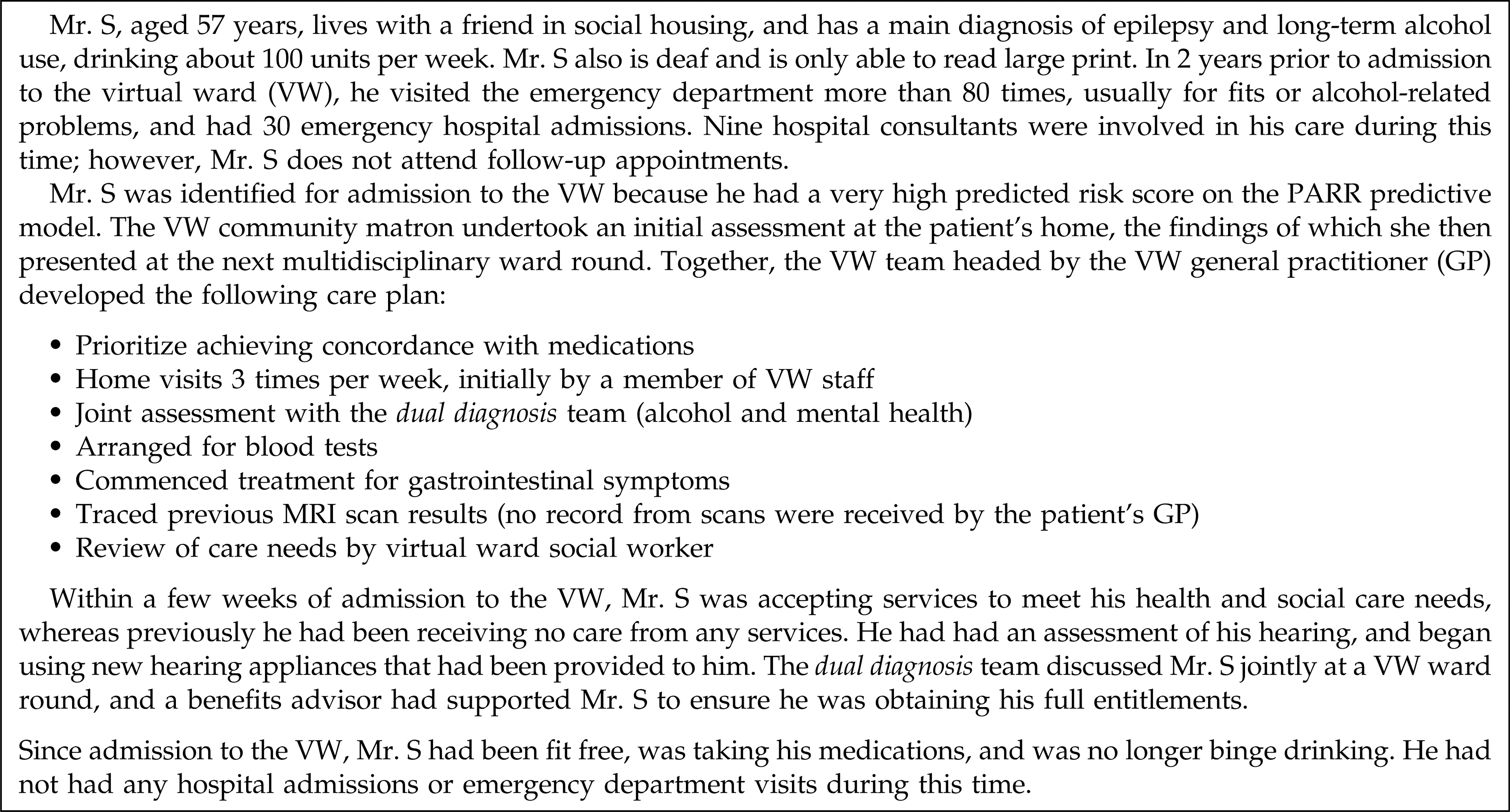
Example case history (certain details have been changed to protect anonymity).
Variations of the Virtual Ward model
Our survey and visits to the study sites have revealed a range of factors that determine how VWs have been implemented in practice. Table 2 provides an outline of a more detailed framework that researchers and policy makers might wish to consider when interpreting the various forthcoming VW evaluation findings.
GP, general practitioner; VW, virtual ward.
Discussion
VWs bring together predictive modeling and a hospital-at-home approach with the aim of improving the quality and integration of preventive care in the community for patients at high risk for unplanned hospital admission. This model of preventive, integrated care may have a number of theoretical advantages over “traditional” one-to-one case management. Potential advantages include the ability to provide continuity of care when a member of the team is away sick or on annual leave, and to reduce fragmentation between the primary, community, and social care sectors by bringing together professionals from different organizations to participate in a joint “ward round.” However, the efficacy and cost-effectiveness of VWs are currently unknown. Several evaluations of VWs are under way and their results are awaited; this article highlights the considerable variation that exists between different VW study sites in practice.
In our survey, some study sites reported that they are using the term “virtual ward” or similar, but currently are delivering care that differs from the core definition of a virtual ward—either because they are not using a predictive model to identify patients (eg, North Somerset) or because they are not holding regular multidisciplinary “ward rounds” (eg, Croydon). Equally, another site (the Hospital2Home project in New York City) appears to be providing the core elements of the VW model of care without using the term “virtual ward.” Therefore, it will be important for researchers and policy makers to bear these differences in mind when the findings of the evaluations are published.
Finally, it is important to remember that even if the evaluations do show a comparative reduction in unplanned hospital admissions for VW patients, any savings generated by the intervention could be undermined by Roemer's law, which states that “a hospital bed built is a hospital bed filled.” 38 In other words, local hospitals may be expected to respond to any reduction in risk for those patients receiving the VW intervention by admitting other, lower risk patients and/or by increasing the average length of stay for hospital inpatients. It will be important for researchers and commissioners to monitor carefully for this phenomenon. One rational way to counter Roemer's law is to close hospital beds or hospital wards. However, politicians and the general public tend to have strong emotional attachments to hospitals, partly because issues of access are more observable than quality or cost-effectiveness concerns. As a result, ward closures are notoriously difficult to achieve in practice, even where they are preferable, all things considered. 39 One unintended benefit of VWs, therefore, is that they could conceivably make the closing of a hospital ward slightly less unpalatable to the public if the closure of each hospital ward was coupled with the opening of 1 or more VWs.
Conclusion
VWs are a model of multidisciplinary case management that is being adopted and adapted in many areas, and which is currently being evaluated in several studies. However, in the same way that different hospital wards vary from each other in terms of their staffing, configuration, and daily routines, so too a number of different variants of VWs are emerging. Researchers should be mindful of these differences when interpreting the results of evaluation studies of VWs.
Footnotes
Acknowledgment
The authors are grateful to Martin Bardsley, Ph.D., who provided helpful comments on an earlier draft; to Heather Watson, M.D., who provided the case history; and to the representatives from the 6 study sites who completed the online questionnaire.
Disclosure Statement
Dr. Lewis, Mrs. Wright, and Dr. Vaithianathan disclosed no conflicts of interest.
This work was funded by the National Institute for Health Research (NIHR) Service Delivery and Organization (SDO) program (Project number 09/1816/1021). The views and opinions expressed here are those of the authors and do not necessarily reflect those of the NIHR SDO program or the Department of Health.