
Abstract
Despite being a screening-amenable cancer, cervical cancer is the third most common genital cancer among white women and the most common among African American women. The study objective was to use administrative claims data for CC disease surveillance among recipients enrolled in a state Medicaid fee-for-service (FFS) program. West Virginia (WV) Medicaid FFS administrative claims data for female recipients aged 21–64 years from 2003 to 2008 were used for this study. All medical and prescription claims were aggregated to reflect each recipient's medical care and prescription drug utilization. The yearly prevalence of Pap smear testing declined from 23.9% in 2003 to 15.8% in 2008 in the Medicaid FFS population. During the 6-year study period, persistence with Pap smear testing was low; 41.8% of recipients received no Pap smear testing. Only 73.1% of recipients received Pap smear testing during the year prior to their CC or precancerous cervical lesions (PCL) diagnosis. The likelihood of a CC diagnosis increased with a decrease in Pap smear testing persistence. Only 10.1% of recipients received appropriate follow-up care following a diagnosis of high-grade PCL; only 31.5% of the recipients received appropriate follow-up care for low-grade PCL diagnosis. Although CC preventive services such as screening and PCL follow-up care are covered under Medicaid programs, underutilization of these services by recipients in the Medicaid FFS population is a concern. Results of this study emphasize the need to address disparities in screening and appropriate PCL follow-up care among recipients in the Medicaid FFS population. (Population Health Management 2012;15:362–371)
Introduction
Various public health organizations, such as the American Cancer Society (ACS) 4 and the United States Preventive Services Task Force (USPSTF), 5 have issued recommendations for screening among women at risk for cervical cancer. Current ACS guidelines recommend screening with Pap smear in all women about 3 years after they begin having vaginal intercourse, but no later than 21 years of age. 4 Screening should then be done every year with the regular Pap smear test or every 2 years using the newer liquid-based Pap smear test. 4 Beginning at age 30, women who have had 3 normal Pap smear test results in a row may be screened every 2 to 3 years. Women older than age 30 also may be screened every 3 years with either the conventional or liquid-based Pap smear test, plus the human papilloma virus (HPV) test. 4 Women 70 years of age or older who have had 3 or more normal Pap tests in a row and no abnormal Pap test results in the last 10 years may choose to stop having Pap tests. 4 However, the USPSTF recommends discontinuing routine Pap smear screening for women who are older than age 65. 5 Women who have had a total hysterectomy (removal of the uterus and cervix) may choose to stop having Pap tests unless the surgery was done as a treatment for cervical cancer or pre-cancer. 4 However, it is recommended that women who have had a hysterectomy without removal of the cervix continue to have Pap smear tests. 4 Besides screening, cervical cancer prevention also requires the eradication of PCL, also referred to as CIN, once they have been identified by screening. Evidence-based consensus guidelines developed by the American Society of Cytology and Cervical Pathology (ASCCP) provide detailed recommendations for the management of women with CIN. 6 Options available for the management of women with CIN include continued screening with or without an excisional procedure such as cryotherapy, laser abalation, electrofulguration, and cold coagulation.
Despite consensus regarding the importance of cervical cancer screening, many women still do not receive guideline-based recommended screening. The failure to be screened has been associated with age, race, low income, inner-city residence, lack of health insurance coverage, and low educational status. 7,8 Health disparities in cervical cancer incidence and survival also exist and are associated with reduced access to care, 9 lack of screening, 10 non-white race, 9,11 –13 contraceptive use, 14 and low socioeconomic status (SES). 15 One of the goals of Healthy People 2020, a national initiative to improve the health of the population and reduce health disparities, is to reduce the death rate from cervical cancer by increasing the proportion of women aged 18 and older who have had Pap smear testing within the preceding 1–3 years. 16 To this end, free cervical cancer screening and diagnostic tests are being provided to low-income and uninsured/underinsured women through the federally funded National Breast and Cervical Cancer Early Detection Program (NBCCEDP). 17 As of 2001, women diagnosed with cervical cancer or PCL through the NBCCEDP program also qualify automatically for Medicaid coverage for the duration of their treatment. 18 Given the high risk of cervical cancer among low-SES women, publicly funded health care programs such as Medicaid play an important role in early detection and prevention. Therefore, it is necessary to monitor cervical cancer incidence and detection over time in this low-income, Medicaid insured population.
The use of administrative claims data for surveillance has been evaluated for a variety of diseases, including cancer. 19 –28 Although these data are inherently limited because their primary function is administrative, they are potentially useful for epidemiologic purposes. 20,23 Most commonly, these administrative data are insurance claims databases, such as Medicare, Medicaid, or Blue Cross, 19,22,23 or statewide hospital discharge files. 21 Administrative claims data also have been used in the past as a rich source of information about cervical cancer disease surveillance among Medicaid recipients. Using claims data, cervical cancer screening rates were found to be lower than the Healthy People 2010 goal rates in North Carolina Medicaid recipients aged 50 years and older. 29 Cervical cancer screening rates improved with referral to a primary care physician among Delaware Medicaid recipients. 30 Cervical cancer risk was found to be higher among those residing in metropolitan areas among Georgia Medicaid recipients. 31 State cancer registry data linked with Medicaid administrative claims data also have identified poor survival associated with cervical cancer diagnosis among Medicaid recipients. 10,32 Recipients who are enrolled in Medicaid intermittently also are at increased risk for late-stage diagnosis, suggesting the need for outreach efforts and access to screening services. 33 Disparities in follow-up care also exist, and were identified among Georgia Medicaid recipients with invasive cervical cancer, with 18% receiving no cancer treatment. 34 Effective communication of test results was identified as the most important barrier to follow-up of abnormal Pap smear testing results among a small group of Medicaid recipients. 35 To date, no study has been performed that provides comprehensive information on the patterns of cervical cancer screening and diagnosis in Medicaid recipients aged 21–64 years. Specifically, the proportion of Medicaid recipients who do receive cervical cancer screening on a timely basis or prior to their diagnosis of cervical cancer/PCL remains unknown. Because a much higher percentage of women develop PCL, it is more important than ever to determine the appropriateness of follow-up care in Medicaid recipients diagnosed with PCL.
In the current study, West Virginia (WV) Medicaid administrative data were used to study the patterns of cervical cancer screening, diagnosis, and PCL follow-up care among Medicaid recipients. The state, all of which is in Appalachia, generally is characterized as being white, rural, poor, and undereducated. 36 Medicaid covers approximately 22% of the total state population. 37 Approximately 46% of Medicaid beneficiaries are enrolled in the managed care plan. 38 Although cervical cancer incidence and death rates (9.2 and 3.3 per 100,000) in the general population are higher in the state than in the United States as a whole (7.9 and 2.4 per 100,000), Pap smear-based screening rates are lower in the state (80.8%) compared to the United States (82.8%). 39,40 The objectives for this study include: (1) to determine Pap smear testing prevalence rates and trends; (2) to determine cervical cancer/PCL diagnosis prevalence trends; (3) to determine Pap smear testing persistence; (4) to determine predictors of Pap smear testing persistence; (5) to determine rates of Pap smear testing prior to cervical cancer/PCL diagnosis; (6) to determine predictors of cervical cancer/PCL diagnosis; and (7) to determine appropriateness of follow-up care following PCL diagnosis.
Methods
The study used WV Medicaid fee-for-service (FFS) administrative claims data, which include medical claim files, prescription claim files, and recipient files from 2003 through 2008. Health care encounter data for recipients enrolled in the Medicaid managed care plan were not available for this study. Managed care enrollment was 46% on average among Medicaid beneficiaries during the study years. 38 Recipient files provide demographic and enrollment information for Medicaid recipients; claim files provide diagnosis, procedure, and prescription drug information using International Classification of Diseases, Ninth Revision (ICD-9)/ Current Procedural Terminology-4 (CPT) codes for reimbursement. 41,42 Records in all files contain recipients' unique identification numbers. These identifiers were used to link recipients across different files. The study protocol was granted exemption from review by the Institutional Review Board at West Virginia University because it involved the use of existing de-identified data. Study cohorts A to F were identified separately for each objective using inclusion and exclusion criteria as listed in Table 1. The initial age of 21 was chosen because guidelines recommend initiation of Pap smears 3 years after the onset of sexual activity (median age of first intercourse for women is 17.4) 43 or age 21. Age 64 was chosen as the upper limit for evaluation because the USPSTF recommends discontinuing routine Pap smear screening once a woman is older than age 655 and because Medicare eligibility begins at age 65.
Cohorts identified separately for each year; +Recipients were continuously enrolled within each year and not necessarily for the 6-year duration.
CIN, cervical intraepithelial neoplasia; n/a, not applicable; PCL, precancerous cervical lesions.
Pap smear testing prevalence rates and trends
Pap smear testing received by recipients in cohort A during a given study year was identified using CPT and ICD-9 codes from medical claims. (A listing of the CPT and ICD-9 codes used is available from the authors upon request.) Cervical cancer screening rate was defined as the percentage of recipients in cohort A who received Pap smear testing and was calculated for each year and reported by age, race, and location of residence. Age was categorized into 3 groups: 21–35 years, 36–45 years, and 45–64 years. Because the state is predominantly white (∼ 95%), race was categorized as white and nonwhite. Location of residence was classified into metro, nonmetro, and rural region based on US Department of Agriculture rural-urban classification codes. 44
Cervical cancer/PCL diagnosis prevalence trends
Cervical cancer/PCL diagnosis among recipients in cohort B during a given year was identified from medical claims using ICD–9 codes: cervical cancer (180.0, 180.1, 180.8, and 180.9); high-grade PCL (233.1 for CIN III, 622.12 for CIN II); and low-grade PCL (622.11 for CIN I). If a recipient had more than 1 type of diagnosis code during the year, the code that represented more advanced disease stage was used for classification. Yearly prevalence rates (per 100,000) were calculated using the total number of recipients in cohort B who had a diagnosis of cervical cancer/PCL in the study year. The rates also were stratified by age, race, and location of residence.
Pap smear testing persistence
Persistence with Pap smear testing among recipients in cohort C was measured by calculating the total number of claims for Pap smear testing, identified using CPT and ICD-9 codes, during the 6-year period. (A listing of the CPT and ICD-9 codes used is available from the authors upon request.) Multiple claims for Pap smear testing during the same day were counted only once. The higher the count, the greater the persistence with Pap smear testing. The number of recipients receiving 0, 1, 2, 3, 4, 5, 6, 7, or more Pap tests during the 6-year time period was calculated.
Predictors of Pap smear testing persistence
Factors associated with Pap smear testing persistence in cohort C was determined using Poisson regression modeling. Independent factors included: recipient's age (as of January 1, 2003), race, location of residence, Charlson comorbidity index, contraceptive use, and access to provider. Charlson comorbidity index score was categorized as 0, 1, 2, or more and was calculated using diagnosis codes from medical claims during the study period. 45 –47 Contraceptive use was assessed by examining prescription claims during the study period. Total number of packs (1 pack=1 month's supply) of contraceptives received by each recipient was determined and used as a continuous independent variable in the model. A proxy measure of access to provider was identified for each recipient based on the type of provider visits they had during the study period. There were 4 categories of access to provider: “No access” if the recipient had no provider visit claim during the analysis window; “Primary care provider” if the recipient had any visit to a general practitioner, internist, family practitioner, or geriatrician during the analysis window; “Ob/Gyn provider” if the recipient had any visit to an obstetrics/gynecology (Ob/Gyn) provider; “Specialist provider” if the recipient had any visits to an oncologist during the analysis window.
Pap smear testing prior to diagnosis
The index date, defined as the date of the first claim containing a diagnosis code for cervical cancer/PCL following January 1, 2004, was identified for each recipient in cohort D. Claims for medical services that occurred during the 365 days prior to the index date were analyzed retrospectively for each recipient in cohort D to identify receipt of Pap smear testing. The proportion of recipients who had a medical services claim for Pap smear testing in the year prior to diagnosis were reported by age, race, location of residence, and type of initial diagnosis.
Predictors of cervical cancer/PCL diagnosis
The index date, defined as the date of the first claim containing a diagnosis code for cervical cancer/PCL following January 1, 2007, was identified for each recipient in cohort E. Claims for medical services that occurred during the 5 years prior to the index date were analyzed retrospectively for each recipient in cohort E to assess Pap smear testing persistence. Factors associated with likelihood of initial diagnosis of cervical cancer, high-grade PCL (CIN III and CIN II), or low-grade PCL (CIN I) were determined using ordinal logistic regression. Independent factors included: recipient's Pap smear testing persistence, age (as of January 1, 2003), race, location of residence, Charlson comorbidity index, contraceptive use, and access to provider. Charlson comorbidity index score and contraceptive use were assessed by examining medical and prescription claims prior to the index date.
Patterns of PCL follow-up care
The index date, defined as the date of the first claim containing a diagnosis code for PCL following January 1, 2003, was identified for each recipient in cohort F. Claims for medical services that occurred during the 14 months following the index date were analyzed prospectively for each recipient to determine appropriate follow-up care based on ASCCP 2001 guidelines. 6
For the purpose of this study, based on the ASCCP 2001 guidelines and taking into consideration normal variance, appropriate follow-up care for CIN I was defined as: (1) a Pap smear test within 5 to 8 months with a second Pap smear test within 11 and 14 months following the index date; or (2) a Pap smear test and colposcopy within 11 and 14 months following the index date; or (3) an HPV DNA test within 11 and 14 months after the index date; or (4) an excisional procedure within 3 months of diagnosis. Similarly, we defined appropriate follow-up care for CIN II and CIN III as having an excisional procedure which is followed by: (1) a Pap smear test at 4 to 6 months; or (2) a Pap smear test and colposcopy at 4 to 6 months; or (3) an HPV DNA test performed within at least 9 months. Individuals having a HPV DNA test or a excisional procedure or a colposcopy were identified using CPT codes (available from the authors upon request).
Frequency and proportions of recipients receiving appropriate versus inappropriate follow-up care for low-grade and high-grade PCL were calculated. The results were stratified by age group, race, and location of residence. Chi-square tests were performed to determine association between type of PCL and appropriateness of follow-up care. All data were analyzed using SAS 9.1 software (SAS Institute Inc., Cary NC).
Results
Pap smear testing prevalence rates and trends
Table 2 displays the number of recipients in Cohort A by year. The yearly prevalence of Pap smear testing among cohort A recipients declined from 23.9% in 2003 to 15.8% in 2008. In most years, the rates were the highest among white females, ages 21-35 years, and those who reside in rural counties.
There were missing values in the geographic region variable.
Cervical cancer/PCL diagnosis yearly prevalence trends
Figure 1 displays the number of recipients in Cohort B by year. During the period 2004 to 2008, the cervical cancer diagnosis yearly prevalence rate (per 100,000) decreased, as did the yearly prevalence rate for CIN III diagnosis. However, the yearly prevalence rate for CIN I and CIN II diagnosis increased between 2004 and 2008 (Fig. 1). In each year, cervical cancer diagnosis prevalence rates were higher among those who were white, ages 46–64 years, and those who resided in nonmetro urban counties (data suppressed due to small cell size).
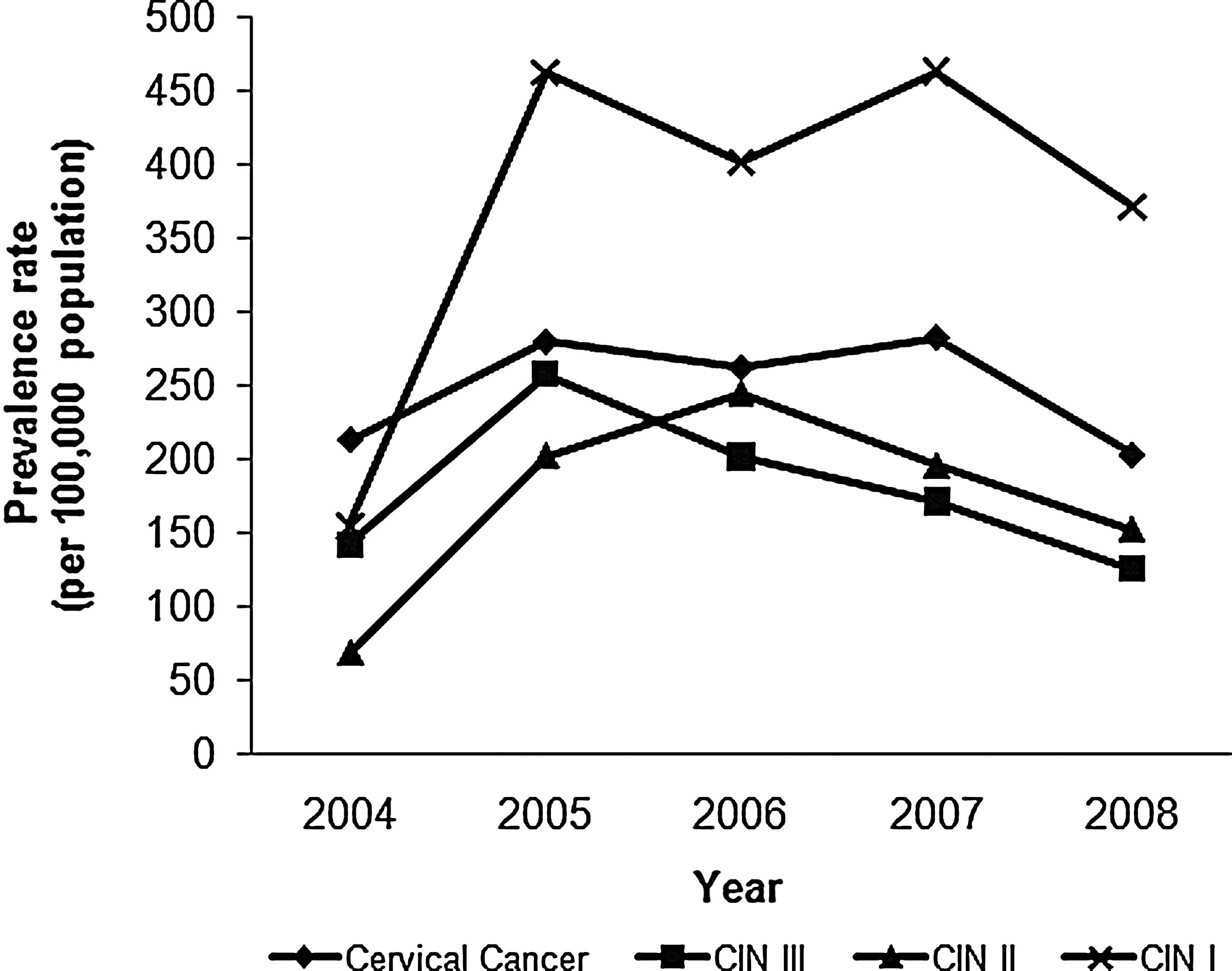
Cervical cancer/precancerous lesion diagnosis yearly prevalence rate (per 100,000) trends among female recipients in the West Virginia Medicaid fee-for-service program, 2004–2008. 2004, N=40,775; 2005, N=41,459; 2006, N=41,563; 2007, N=53,072; 2008, N=55,681. CIN, cervical intraepithelial neoplasia.
Pap smear testing persistence
Overall, Pap smear testing persistence was low among recipients in Cohort C. Approximately 41.8% had no receipt of Pap smear testing during the 6-year study period. Greater persistence (3 or more Pap smear tests) was seen in only 22.7% of recipients during the study period (Fig. 2).
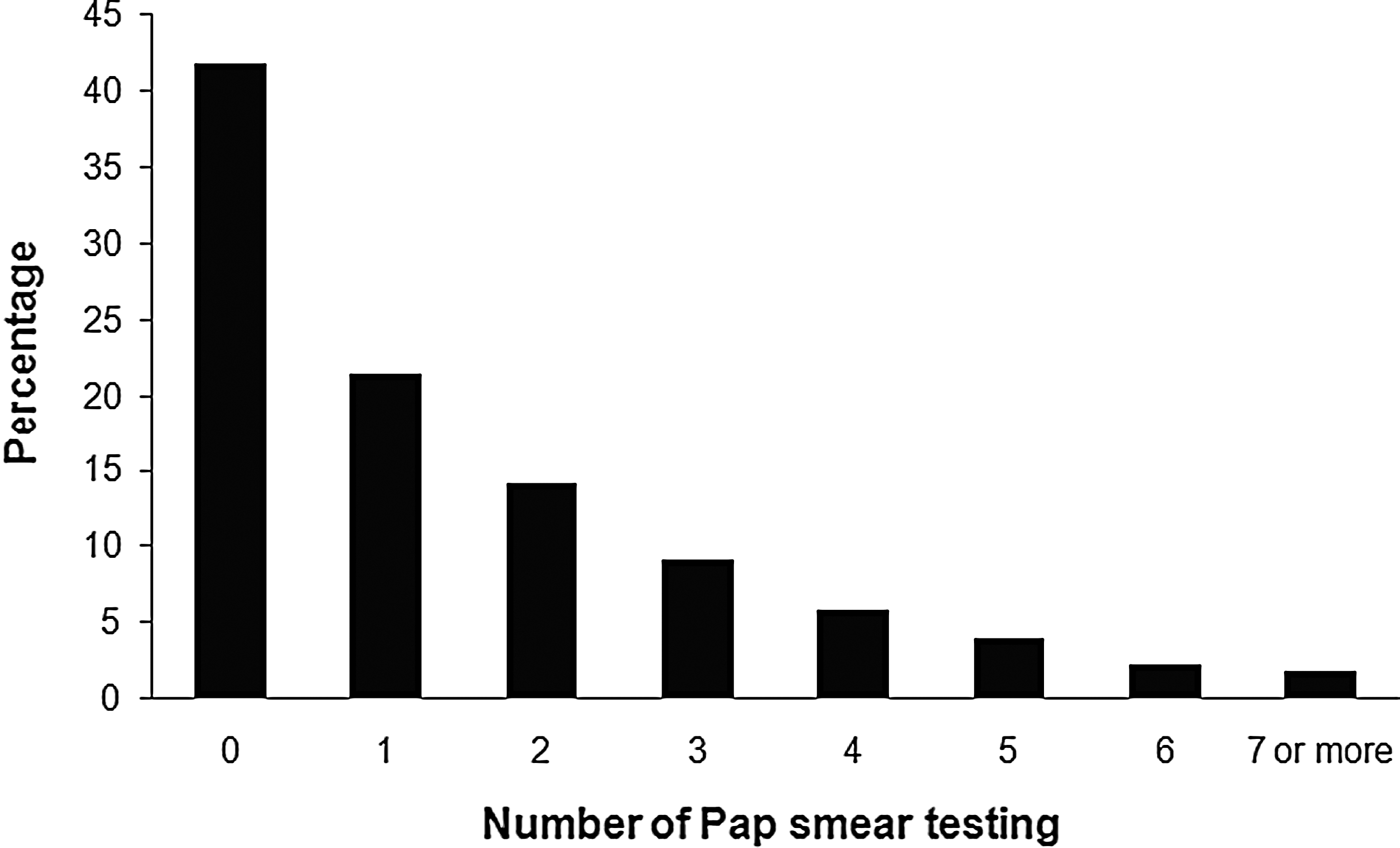
Pap smear testing persistence among female recipients in the West Virginia Medicaid fee-for-service program, 2003–2008 (N=22,295). Each bar represents the proportion of recipients who received a given number of Pap smear tests during the study period; it is assumed that receiving a higher number of Pap smear tests is indicative of high persistence with screening.
Predictors of Pap smear testing persistence
Significant predictors of Pap smear testing persistence in cohort C included age, race, location, Charlson comorbidity status, contraceptive use, and access to provider. Overall Poisson regression model was significant. Pap smear testing persistence was higher among white recipients compared to nonwhite; lower among those who resided in metro and nonmetro counties compared to rural counties; and lower among those with a Charlson comorbidity index score of zero compared to those with an index score of 2 or more. Pap smear testing persistence increased with age, contraceptive use, and with access to specialist provider (Table 3).
P≤0.05; Log Likelihood (Full model)=− 15,125.98, Log Likelihood (Intercept)=−20,150.91, chi-square value=10,049.86, P≤0.05; CI, confidence interval; Ob/Gyn, obstetrics/gynecology provider.
Pap smear testing prior to diagnosis
Overall, 73.1% of recipients in Cohort D received Pap smear testing during the 365-day period prior to their index date of diagnosis. The proportion was higher among recipients with an index diagnosis of CIN II. The proportions were also higher among those who were white, ages 21–35 years, and those who resided in rural counties (Table 4).
There were missing values in the geographic region variable; CIN, cervical intraepithelial neoplasia.
Predictors of cervical cancer/PCL diagnosis
Pap smear testing persistence and access to Ob/Gyn providers were identified as significant predictors of cervical cancer/PCL diagnosis among recipients in cohort E. The overall ordinal logistic regression was significant. The likelihood of a more severe diagnosis (cervical cancer vs. high-grade PCL vs low-grade PCL) increased with a decrease in Pap smear testing persistence and with access to Ob/Gyn and specialty providers (Table 5).
P≤0.05; Probability modeled for likelihood of diagnosis of cervical cancer followed by high-grade lesion, followed by low-grade lesion; Likelihood ratio: chi-square=35.20, P≤0.01; Score test for Proportional Odds assumption: chi-square=18.86, P≤0.09; CI, confidence interval; Ob/Gyn, obstetrics/gynecology provider.
Patterns of PCL follow-up care
The proportion of female recipients who received appropriate follow-up care is displayed in Table 6. Significant association existed between type of lesion and appropriateness of follow-up care. Most of the recipients who received appropriate follow-up care were white and resided in nonmetro urban counties. Most of the recipients with inappropriate follow-up care were white, ages 21–35 years, and those who resided in metro counties (low-grade PCL) and nonmetro counties (high-grade PCL) (Table 7).
p≤0.05; aLow-grade precancerous lesions include cervical intraepithelial neoplasia-I; bHigh-grade precancerous lesions include cervical intraepithelial neoplasia-II and cervical intraepithelial neoplasia-III.
There were missing values in the geographic region variable; aLow-grade precancerous lesions include cervical intraepithelial neoplasia-I; bHigh-grade precancerous lesions include cervical intraepithelial neoplasia-II and cervical intraepithelial neoplasia-III.
Discussion
Cervical cancer incidence and mortality rates among women have declined in the United States since the introduction of Pap smear testing. 2 Still, cervical cancer remains the third most common genital cancer among white women and the most common genital cancer among African American women. 1 Given the high risk of cervical cancer among low-income and uninsured/underinsured women, publicly funded health care programs such as NBCCEDP and Medicaid play an important role in early detection and prevention. Disparities in incidence and mortality still exist between Medicaid and the general population, suggesting underutilization of cervical cancer screening and preventive services among Medicaid recipients.
The current study is the first to examine patterns of cervical cancer screening, diagnosis, and PCL follow-up care in a state Medicaid FFS population. The study adds to the literature by demonstrating that the cervical cancer screening rate is lower among Medicaid FFS recipients than the general population despite the population's access to primary care and full coverage of cancer screening services by Medicaid. This study differs from most published reports of cervical cancer screening rates as data were obtained from Medicaid administrative claims data rather than from patient self-report, the accuracy of which has been reported to be low in epidemiologic studies. The low screening rates also are comparable to the results of studies involving North Carolina and Delaware Medicaid recipients. 29,30 Direct comparison of rates from this study to those of the Behavioral Risk Factor Surveillance System (BRFSS) survey is not advisable because the latter reports screening rates for women aged 18 and older who have had a Pap test within the past 3 years. 39
The screening rates in this study were higher for recipients from rural regions as compared to their urban counterparts. The observed difference in this study may have resulted from exclusion of urban residents who received screening but were enrolled in Medicaid intermittently during the study period, and therefore not captured in our continuously enrolled cohorts. This may happen because recipients from rural regions in WV are likely to be more disadvantaged economically than their urban counterparts, and therefore also more likely to be continuously enrolled in Medicaid. Urban–rural differences in cervical cancer incidence have been observed by other researchers as well. 31,48,49 They found higher incidence of cervical cancer in urban populations than in rural populations and these differences were attributed to differences in lifestyle and in cervical cancer risk in urban and rural populations. A policy brief using BRFSS data did not find any significant difference in cervical cancer screening rates across the urban–rural continuum in the United States. 50
The study also reveals the lack of persistence among Medicaid FFS recipients to get screened, because less than one third of all recipients received 3 or more Pap smear tests during the 6-year study period. Persistence with screening was low among young recipients and was higher among those recipients with access to Ob/Gyn or specialist providers. Recipients with a low Charlson comorbidity index score were found less likely to be persistent in their screening behavior, suggesting a need for targeted educational interventions for this group. Educational interventions promoting adherence to cervical cancer screening guidelines in the Medicaid FFS population also is important because approximately half (48%) of all recipients received Pap smear testing in the year prior to their index date of cervical cancer diagnosis, a much lower rate compared to that observed among recipients with a PCL diagnosis (72%–85%). This difference suggests that regular screening can help with early diagnosis.
Although the trend in yearly cervical cancer prevalence rates and high-grade PCL (CIN II and CIN III) prevalence rates remained flat, an upward trend was found in low-grade PCL (CIN I) prevalence rates. This suggests that more recipients are getting diagnosed earlier than before, which may have resulted from an increased use of screening services. However these results cannot be directly compared with those from screening usage patterns (Pap smear testing prevalence and persistence) because the cohorts for these study objectives differed. However, Pap smear testing persistence and access to Ob/Gyn providers were identified as significant predictors of a higher stage diagnosis, with the likelihood increasing with decreasing Pap smear testing persistence and with access to Ob/Gyn providers.
Lower screening rates in the state Medicaid FFS population highlight the need to promote cervical cancer screening and perhaps other self-care behaviors. It also underscores the importance of programs such as NBCCEDP, which targets low-income women. Educational interventions to improve cervical cancer screening persistence are likely to reduce the risk of late-stage cervical cancer diagnosis in this population. 33 This is specifically true for those recipients who do not have any medical conditions (or are simply healthy) and therefore are less likely to visit a health care provider. They must be educated about the benefits of regular screening and early diagnoses and made aware that these services are covered by Medicaid. Furthermore, outreach efforts also are required for recipients who enroll in Medicaid intermittently, as they are at increased risk of late-stage diagnosis. 33
The most important finding of this study is the lack of appropriate PCL follow-up care among Medicaid FFS recipients. Considering the increasing occurrence of a PCL diagnosis among women, 3 which also was found in this study, eradication of PCL that has been identified by screening is an important preventive step to reduce cervical cancer-related mortality. The lower rates of appropriate follow-up care seen in this study may have resulted from the recipients' lack of involvement in their own health and the resulting underutilization of covered services. Effective communication of test results was identified in a prior Medicaid study as the most important factor related to follow-up after an abnormal Pap smear test. 35 Similar to other studies, we found the lack of appropriate follow-up care higher among younger recipients. 10,32,35 Recipients with abnormal Pap smears may be afraid of cancer and of colposcopy and its side effects. Efforts to better assess whether recipients understand the meaning of their abnormal Pap smear results are needed for this population.
The findings from this study are subject to several limitations. An inherent limitation of using administrative claims data for epidemiologic studies is the lack of clinical detail, resulting in the possibility of misclassification. 20,23 Possibility of misclassification also can occur as a result of coding errors within administrative claims data. However, in the past few years, there has been an increasing interest in analyzing large health claims databases to assess screening, treatment, and outcomes for specific diseases. 20,23,51 Claims data have been evaluated for their utility as a source of epidemiologic or health services information on cancer patients. 19 –28 Increasing the use of these types of data to assess the quality of cancer care also has been identified as a priority by the Institute of Medicine. 51 Studies using claims data are usually population based and have the potential to address a number of priority questions regarding health care disparities and the quality of cancer care. These population-based rates also provide valuable information for future planning and prioritization of health programs.
The results from this study are generalizable only to the Medicaid FFS population aged 21 to 64 years, as encounter data for Medicaid recipients enrolled in the managed care plan were not available for this study. There was a steady increase in the percentage of Medicaid recipients enrolled in managed care during the study years; it was 46% on average. 38 This might have resulted in a sicker Medicaid FFS population, which could explain the poor screening behavior and outcomes observed in this study. Data on any care received by the recipients outside of the Medicaid system or through non-Medicaid providers also were not available in the claims data for our study.
Medicaid eligibility type information was unavailable for this study and, hence, was not used in cohort selection. The cohort selection in this study was limited to those enrolled in Medicaid continuously during the study period. This resulted in the non-inclusion of individuals with noncontinuous enrollment and the loss of individuals who were enrolled intermittently. As each study objective required us to have a distinct cohort, direct comparison of results from each objective is not valid. In defining persistence with screening, we acknowledge that various guidelines have been published, each of which recommends a particular set of screening standards. For the purpose of this study, we assumed that receiving a greater number of Pap smear tests over the 6-year study period was indicative of high persistence with screening. Because of limited data availability, the number of recipients in our study sample who may have had a hysterectomy before January 1, 2003 cannot be determined. This may lead to a slight overestimation of the proportion of recipients who did not receive Pap smear testing during the study period. Finally, our definition of appropriate versus inappropriate initial follow-up is limited to the data recorded in the claims, such as the presence or absence of diagnosis and CPT codes. Clinical-level data and results of screening tests are not available in the claims data, making it difficult to truly assess whether appropriate or inappropriate care was received. Because only 6 years of data were available, we were unable to conduct a long-term follow-up to assess the positive or negative outcomes associated with appropriate versus inappropriate follow-up.
This study is the first of its kind in which state Medicaid administrative data were used to determine disparities in cervical cancer screening, diagnosis rates, and patterns of PCL follow-up care in a Medicaid FFS population. Although cervical cancer preventive services such as screening and PCL follow-up care are covered under Medicaid programs, underutilization of these services by recipients in the Medicaid FFS population is a concern. Results of this study emphasize the need to address disparities in screening and appropriate PCL follow-up care among recipients in the Medicaid FFS population who traditionally are known to be more sick or disabled than Medicaid managed care enrollees.
Footnotes
Disclosure Statement
Mr. Nadpara and Drs. Madhavan, Khanna, Smith, and Miller disclosed no conflicts of interest.
This project was supported by Grant Number P20-HS015930 (SM) from the Agency of Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality. The authors also acknowledge support from the West Virginia Bureau of Medical Services.
This work was performed at the Department of Pharmaceutical Systems and Policy, School of Pharmacy, West Virginia University.