
Abstract
This economic evaluation takes the perspective of a health plan provider. The primary objective was to determine if medical expenses of members enrolled in the not-for-profit, US-based Union Pacific Railroad Employes Health Systems (UPREHS) health plan were reduced after implementing a low-cost, patient-focused education campaign on sleep-disordered breathing (SDB). The authors reviewed medical claims records of all members (N=22,275) from 2 years before (2005–2006) and 2 years after (2007–2008) the campaign. Members were assigned to a non-SDB (did not seek diagnosis or not diagnosed with SDB), an SDB-NT (diagnosed with SDB but not on therapy), or an SDB-PAP (diagnosed with SDB and on positive airway pressure [PAP] therapy) group. The authors assessed overall medical and inpatient hospital costs (calculated as annual per member per month [PMPM] costs), and number of hospital admissions. The percentage of members with SDB was 11.1% (2350/21,185) in 2005 and 10.5% (2385/22,639) in 2008. During the study, the percentage of members with SDB receiving PAP increased 145% (2005: 23%, 517/2350; 2008: 54.3%, 1265/2385). After the campaign was initiated, overall medical PMPM costs were significantly lower for the SDB-PAP than the SDB-NT group (2007: $572.10 vs. $720.27, P=0.0006; 2008: $645.66 vs. $846.58, P=0.0009), resulting in a differential cost savings of $4.9 million for the study period. In addition, inpatient hospital PMPM costs and the number of hospital admissions also were lower for the SDB-PAP group than for the SDB-NT group. These findings suggest that an SDB education campaign can improve health care outcomes and reduce medical expenses. (Population Health Management 2013:16:7–13)
Introduction
Disease management plans should ensure that SDB is given appropriate attention. Because of its chronic nature, effects on physical and cognitive function, and associated comorbidities, SDB has significant direct and indirect economic consequences. 5 SDB is associated with higher rates of hospitalization, contact with health care specialists, and medication use, 1 all of which contribute to direct costs. Productivity losses and the increased risk of workplace and motor vehicle accidents caused by the tiredness, lethargy, and inattention resulting from SDB contribute to the indirect costs. 5,14 In the United States, the economic cost of unmanaged SDB (moderate-to-severe obstructive sleep apnea) is estimated to be between $65 and $165 billion. 3 The costs of diagnosing and treating SDB are small relative to the costs associated with its consequences, 5 and the benefits associated with the treatment of SDB (eg, decreased number of days off work) may be realized within the first year of treatment. 15 Studies assessing management strategies for SDB have shown that continuous positive airway pressure (PAP) therapy is more cost-effective and efficacious than other strategies (eg, dental devices, lifestyle advice, no treatment). 16 –18 In particular, patients with severe SDB (obstructive sleep apnea/hypopnea syndrome) can benefit from PAP; continuous PAP therapy was considered more effective clinically than no treatment and, after a minimum of 2 years of treatment, was deemed to be cost-effective. 19
Hence, apart from humane considerations relating to individual well-being, the incentive to treat SDB is economically rational. However, information on the cost savings that might be achieved by implementing an SDB education campaign in a US workplace setting is limited. In this study, the not-for-profit, US-based Union Pacific Railroad Employes Health Systems (UPREHS) initiated a low-cost, patient-focused education campaign designed to increase awareness of SDB for those employees at high risk, and to encourage high-risk employees to seek provider assistance for the diagnosis and treatment of SDB. The primary objective of this retrospective claims-based study was to determine if medical expenses of members enrolled in the UPREHS health plan were reduced after implementation of an SDB education campaign. The authors compared the overall medical costs, inpatient hospital costs, and the number of hospital admissions for members without SDB, members with SDB not on PAP therapy, and members with SDB on PAP therapy.
Methods
Study design
This was a 4-year retrospective review of medical claims data from the UPREHS member self-funded health plan. Medical claims data were collected from the 2 years before (2005–2006) and the 2 years after (2007–2008) UPREHS introduced an SDB education campaign for its members. All medical claims data were de-identified before analysis in accordance with the requirements of the Health Insurance Portability and Accountability Act. Although the Chesapeake Research Review, Inc. Institutional Review Board reviewed our study, it was considered exempt from review under Department of Health and Human Services regulations.
Samples
Medical and pharmacy claim records from 2005 to 2008 of all members (N=22,275) enrolled in the UPREHS health plan were reviewed to determine which members had been diagnosed with an SDB syndrome. The SDB syndromes, diagnosed by polysomnography (PSG), were obstructive sleep apnea, central sleep apnea, Cheyne-Stokes respiration, hypoventilation, and hypersomnia. Members were assigned to 1 of 3 groups: the non-SDB group, the SDB not on therapy (SDB-NT) group, or the SDB on PAP therapy (SDB-PAP) group. The non-SDB group comprised members who underwent PSG but were not diagnosed with SDB and those who did not seek a diagnosis. The SDB-NT group comprised members who were diagnosed with SDB before or during the study and who did not receive, or were yet to start, PAP therapy. The SDB-PAP group comprised members diagnosed with SDB who were receiving PAP therapy. Members diagnosed with SDB during the study but not treated with PAP were assigned to the SDB-NT group for the entire study (ie, from 2005 to 2008), regardless of when their SDB was diagnosed. This conservative assignment was made because we assumed that members with SDB would have had SDB for the entire study owing to the chronic nature of SDB. Members with SDB who began PAP therapy during the study were assigned to the SDB-PAP group (ie, switched from the SDB-NT group) when they started treatment.
The SDB education campaign
An SDB education campaign was initiated by UPREHS to guide members through the diagnosis and treatment of SDB. Specifically, UPREHS developed a 3-set series of oversized, educational postcards that were mailed to UPREHS members in 6-week increments. The postcards were mailed initially to UPREHS members residing in North Platte, NE, as this was where most members resided. The postcards were mailed to the remaining UPREHS members (located in more than 30 states) 4 months after the initial mailing of postcards to members residing in North Platte. The postcards were designed to help UPREHS members identify the risk factors for SDB. UPREHS promoted the mailing of these postcards in its employee newsletter and on its Web site. A toll-free number was included on the postcards to help interested members contact UPREHS medical services staff and discuss the steps necessary to test for SDB and, if diagnosed with SDB, to receive a PAP device (ResMed Corp., San Diego, CA). UPREHS would direct members to pre-certified sleep centers that could perform PSG.
Members who were prescribed a PAP device underwent nocturnal PSG with continuous PAP titration or a trial on auto-titrating PAP for 2 weeks, based on their treating physician's recommendation, to determine the optimal pressure of their PAP device. Throughout the program, a registered sleep technologist coordinated and monitored the care of each patient (with the prescribing physician), and educated patients on the proper use of the PAP device. Follow-up occurred after the delivery of the PAP device, at 2 and 6 weeks, at 6 months, and then annually. Objective data from the PAP device were collected on a fixed schedule to determine if adjustments to the PAP device were necessary. For the purposes of this education campaign, the symptoms of SDB, the steps for diagnosis of SDB, and the use of PAP therapy were discussed by UPREHS medical services staff with members diagnosed with SDB.
Data analysis
The outcome measures were overall medical costs, inpatient hospital costs, and hospital admissions for the non-SDB group, the SDB-PAP group, and the SDB-NT group.
Overall medical costs and inpatient hospital costs (reported in US dollars) were calculated as an annual per member per month (PMPM) cost. A PMPM cost is a calculation commonly used by health plans to determine the average costs for total membership or for subcategories of patients or conditions. The annual PMPM cost was calculated by aggregating the medical expenses incurred in a given year and dividing that amount by the total number of member months for that year. Plan members could have had 1 to 12 member months per year, depending on their participation status (eg, new enrollees, early terminations, or deaths). Ambulatory or retail pharmacy benefit costs were not included in the calculation of overall medical costs. However, the costs of drugs, vaccinations, intravenous medications, or nutritional supplements administered during the course of treatment at a hospital, an ambulatory surgical facility, a physician's office, or at home were included. To normalize the data analysis, members with SDB who began PAP therapy (as defined by the PAP claim or delivery date) during the first half of the month (days 1–15) had their non-sleep-related claims costs included in the SDB-PAP group calculations for that month. Members with SDB who began PAP therapy during the second half of the month (day 16 onward) had their non-sleep-related claims costs included in the SDB-NT group calculations. The costs associated with SDB diagnosis were included in the SDB-NT group calculations whereas the costs associated with PAP therapy were included in the SDB-PAP group calculations. All PAP devices were purchased by the health plan. The formula used to calculate the differential savings between the SDB-PAP and SDB-NT groups was ((PMPMSDB-NT – PMPMSDB-PAP) × 12) × N membersSDB-PAP.
Statistical analysis
Descriptive statistics were used to calculate the mean and standard deviation or the median, minimum, and maximum for continuous variables, or the counts and percentages for categorical variables. Comparisons between groups were done using Student t tests. Statistical significance was prespecified at a 2-sided P<0.05. SAS version 9.1.3 (SAS Institute Inc., Cary, NC) was used for all statistical analyses.
Results
Member disposition and demographics
The number of members in the UPREHS health plan and number of member months are displayed in Table 1. From 2005 to 2008, 89.5% of those members diagnosed with SDB had been enrolled continually in the health plan. Although there was a 30% increase in titration studies by PSG from 2005–2006 (n=621) to 2007–2008 (n=804), the incidence of diagnosed SDB remained stable. There was a 145% improvement in members with SDB being treated with PAP therapy: 23% (517/2350) were treated with PAP in 2005 compared with 54.3% (1265/2385) in 2008.
Non-SDB group, members not diagnosed with SDB and those who did not seek a diagnosis; SDB-NT group, members diagnosed with SDB who did not receive, or were yet to start, PAP therapy; SDB-PAP group, members diagnosed with SDB who were receiving PAP therapy. NT, not on therapy; PAP, positive airway pressure; SDB, sleep-disordered breathing.
Most members in the UPREHS health plan were male and more than 50% of members with SDB were older than 50 years of age (Table 2). Members with SDB and those who were subsequently treated with PAP were generally in poorer health than those without SDB or those not treated with PAP. At the start and during the study, members with SDB were more likely to have 1 of the 5 comorbidities commonly associated with SDB (type 2 diabetes mellitus, chronic obstructive pulmonary disorder, congestive heart failure, hypertension, and obesity) than members without SDB (Table 2). Similarly, at the start and during the study, members with SDB who were treated with PAP had a higher incidence of these comorbidities than those not treated with PAP.
Member demographic information for those in the non-SDB group was not available for 2005.
Non-SDB group, members not diagnosed with SDB and those who did not seek a diagnosis; SDB-NT group, members diagnosed with SDB who did not receive, or were yet to start, PAP therapy; SDB-PAP group, members diagnosed with SDB who were receiving PAP therapy. Abbreviations: COPD, chronic obstructive pulmonary disease; NR, not reported; NT, not on therapy; PAP, positive airway pressure; SD, standard deviation; SDB, sleep-disordered breathing.
Indicates P>0.01 as tested by Student t tests between the non-SDB and SDB populations. **indicates P<0.05 and ***indicates P>0.01 as tested by Student t tests between the SDB-PAP and SDB-NT populations.
Cost of the SDB education campaign
The SDB education campaign had a low PMPM cost. The cost of the postcards and the cost of mailing the postcards to all UPREHS members was $0.08–$0.11 PMPM. For all UPREHS members, the cost of the SDB education program and follow-up was $0.008 PMPM. For UPREHS members enrolled in the SDB education program and follow-up, the cost of the program and follow-up was $4.00–$6.83 PMPM.
Medical claims costs
Overall Medical Costs
The UPREHS overall annual medical claims costs increased 22.1% from 2005 ($79.1 million) to 2008 ($96.5 million). On a PMPM basis, overall medical claims costs increased 14.3% from $310.97 PMPM in 2005 to $355.41 PMPM in 2008.
Overall medical costs varied depending on whether members were diagnosed with SDB and whether members with SDB were treated with PAP therapy (Fig. 1). Throughout the study, overall medical costs were lowest for the non-SDB group and remained stable. Before the education campaign, overall medical PMPM costs were significantly higher for the SDB-PAP group than the SDB-NT group in 2005 (P=0.04), but were similar between groups in 2006 (P=0.2663). Thus, the use of PAP was associated with a differential cost of $579,730 in 2005, but a differential savings of $422,652 in 2006. After the education campaign, overall medical PMPM costs were significantly lower each year for the SDB-PAP group than the SDB-NT group (2007: P=0.0006; 2008: P=0.0009). Thus, the use of PAP was associated with a differential savings of $1,722,180 in 2007 and a differential savings of $3,049,564 in 2008. Overall, the effect of the education program on the use of PAP was associated with a differential savings of $4,928,822: A differential cost of $157,078 before the education program and a differential savings of $4,771,744 after the education program. Similar results were obtained when the costs for the diagnosis of SDB and the PAP device and supplies were excluded from the post hoc analysis of overall medical PMPM costs (data not shown).
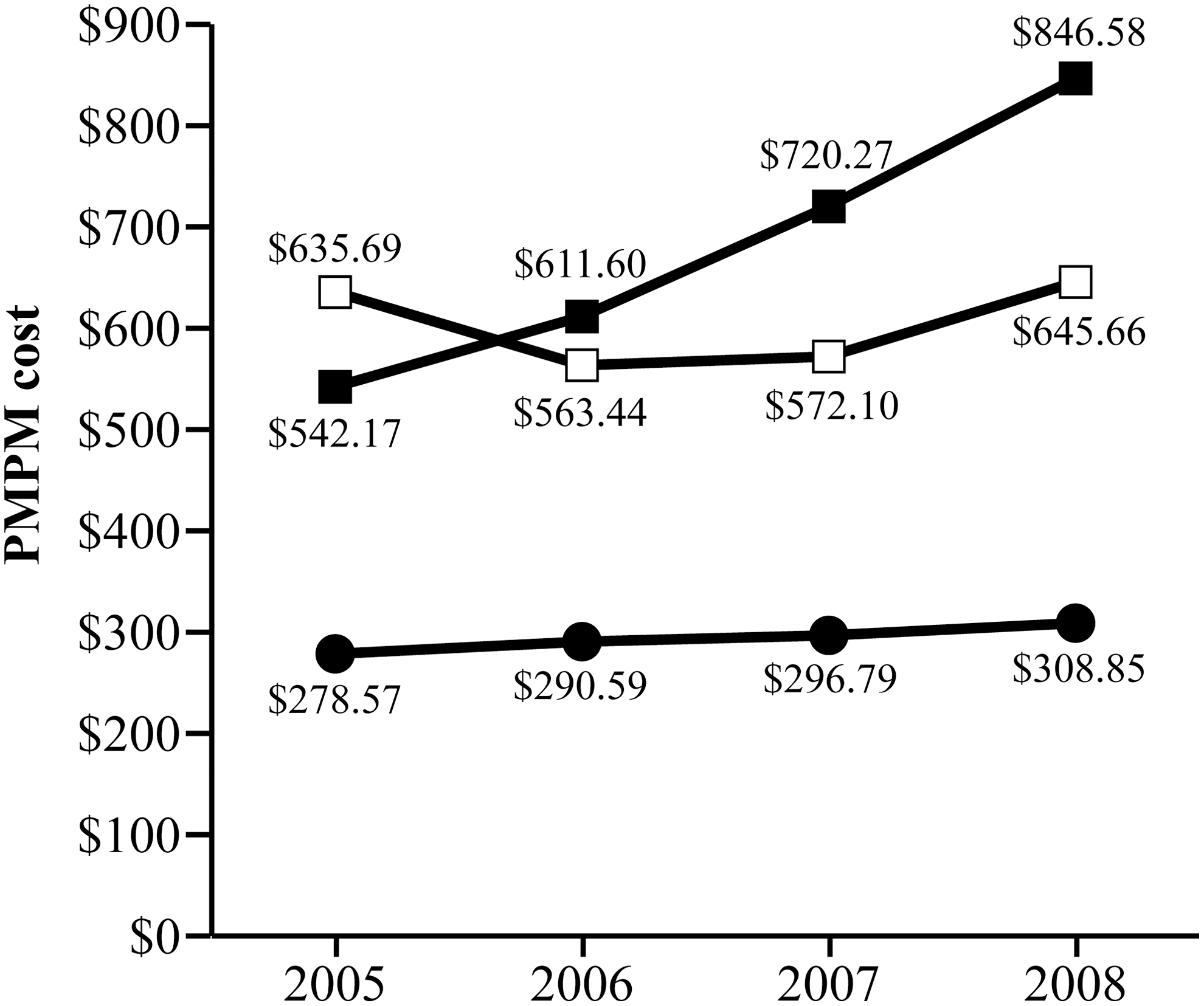
Overall medical per member per month (PMPM) costs. Non-SDB group (—●—), members not diagnosed with SDB and those who did not seek a diagnosis; SDB-NT group (—■—), members diagnosed with SDB who did not receive, or were yet to start, PAP therapy; SDB-PAP group (—□—), members diagnosed with SDB who were receiving PAP therapy. Abbreviations: NT, not on therapy; PAP, positive airway pressure; SDB, sleep-disordered breathing. Student t test between the SDB-NT and SDB-PAP groups: P<0.05 for 2005, P>0.05 for 2006, and P>0.001 for 2007 and 2008.
A comparison of overall medical PMPM costs in the 12 months before and the 12 months after initiation of PAP therapy for members with SDB (n=654) showed a post-therapy savings of $20.04 PMPM (2.5% reduction in medical costs after initiation of PAP). A post hoc subanalysis of members diagnosed with obstructive sleep apnea and excluding members exceeding $200,000 in claims during the 24 months (n=645) showed a post-therapy savings in overall medical PMPM costs of $87.52 (11.1% reduction in medical costs after initiation of PAP).
Sleep apnea-related claims
From 2005 to 2008, the PMPM costs for all claims for members with a primary diagnosis of sleep apnea (International Classification of Diseases, Ninth Revision codes 327.23, 780.53, and 780.57) decreased from $70.70 to $54.09 in the SDB-PAP group, but increased from $32.39 to $85.38 in the SDB-NT group. After the education campaign, treatment of SDB with PAP resulted in a differential savings for sleep apnea-related claims of $89,361 in 2007 and $461,869 in 2008.
Inpatient hospital costs
Inpatient hospital costs varied depending on whether members were diagnosed with SDB and whether members with SDB were treated with PAP therapy (Fig. 2). Throughout the study, inpatient hospital PMPM costs were lowest for the non-SDB group and remained stable. Before the education campaign, inpatient hospital PMPM costs for the SDB-PAP and the SDB-NT groups were similar (2005: P=0.6173) or significantly lower for the SDB-PAP group (2006: difference=$73.11, P=0.0239). After the education campaign, the inpatient hospitals costs were significantly lower each year for the SDB-PAP group than the SDB-NT group (2007: difference=$85.67, P=0.0211; 2008: difference=$141.85, P=0.0086).
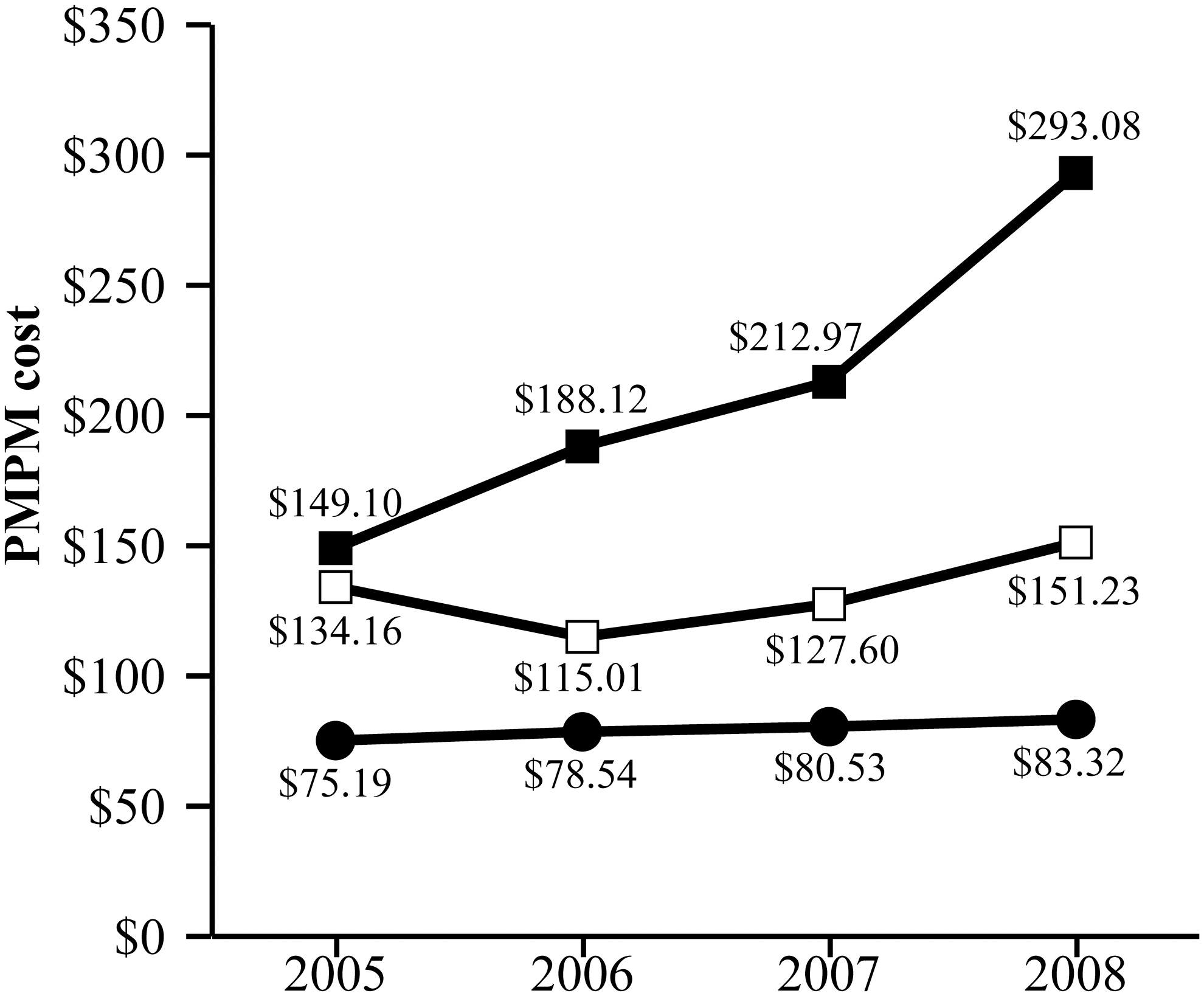
In-patient hospital per member per month (PMPM) costs. Non-SDB group (—●—), members not diagnosed with SDB and those who did not seek a diagnosis; SDB-NT group (—■—), members diagnosed with SDB who did not receive, or were yet to start, PAP therapy; SDB-PAP group (—□—), members diagnosed with SDB who were receiving PAP therapy. Abbreviations: NT, not on therapy; PAP, positive airway pressure; SDB, sleep-disordered breathing. Student t test between the SDB-NT and SDB-PAP groups: P>0.05 for 2005, P<0.05 for 2006 and 2007, and P<0.01 for 2008.
Hospital admissions
The number of hospital admissions varied depending on whether members were diagnosed with SDB and whether members with SDB were treated with PAP therapy (Fig. 3). Throughout the study, the number of hospital admissions was lowest for the non-SDB group and remained stable. Before the education campaign, the number of hospital admissions for the SDB-PAP and the SDB-NT groups was the same or lower for the SDB-PAP group (P=0.0805). After the education campaign, the number of hospital admissions was lower each year for the SDB-PAP group than the SDB-NT group.
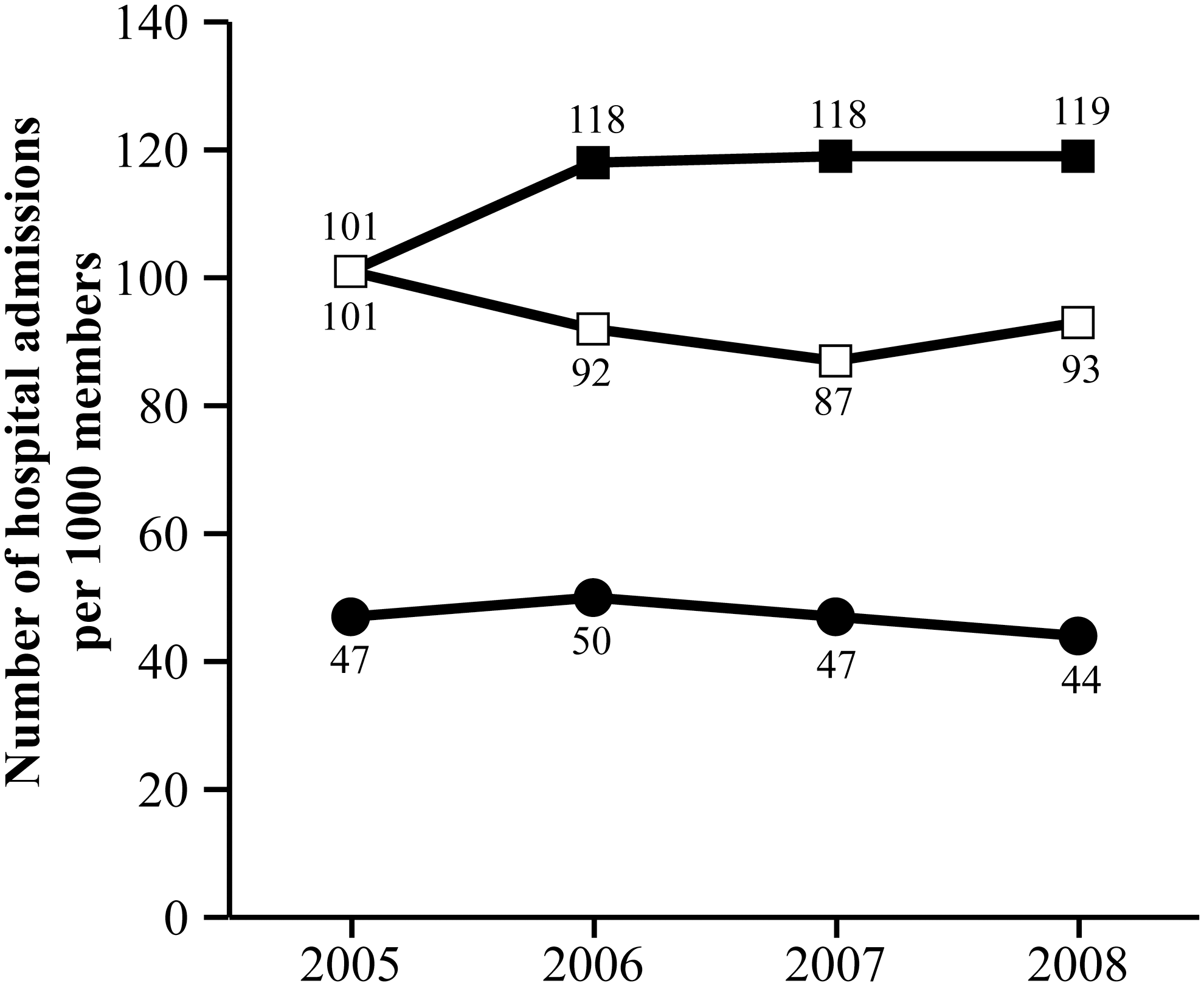
Number of hospital admissions per 1000 members. Non-SDB group (—●—), members not diagnosed with SDB and those who did not seek a diagnosis; SDB-NT group (—■—), members diagnosed with SDB who did not receive, or were yet to start, PAP therapy; SDB-PAP group (—□—), members diagnosed with SDB who were receiving PAP therapy. Abbreviations: NT, not on therapy; PAP, positive airway pressure; SDB, sleep-disordered breathing. Student t test between the SDB-NT and SDB-PAP groups: P>0.05 for 2005 and 2006, P<0.05 for 2007, and P>0.05 for 2008.
Discussion
To our knowledge, this is the first study to investigate the effects of an SDB education campaign in a US workplace setting on medical expenses and health outcomes. Based on our retrospective analysis of medical claims data, a low-cost, patient-focused SDB education campaign was associated with a 145% increase in the uptake of PAP therapy by members with SDB and, within 2 years after initiating the campaign, the use of PAP therapy was associated with a $4.9 million differential savings in overall medical costs. In addition, members with SDB who were treated with PAP had lower inpatient hospital costs and fewer hospital admissions than members with SDB who did not receive PAP therapy. Our findings suggest that an SDB education campaign can result in substantial savings for a health care plan by encouraging members to seek and use appropriate treatment for SDB.
Although cost of illness analyses provide a framework for cost estimation in cost-effectiveness and cost-benefit analyses, results from our study have a real-world use. We exposed all UPREHS health plan members, a population that had key risk factors for SDB (eg, older age, mostly male), 20 to the SDB education campaign. The 145% increase in the use of PAP therapy suggests that our SDB education campaign provided the guidance and support necessary to help members navigate the SDB treatment pathway successfully. This guidance and support included a registered sleep technologist who coordinated and monitored the care of each patient, educated patients on the proper use of the PAP device, and encouraged compliance. We propose that, in this real-world setting, our education campaign served as a catalyst for change for members who could have become complacent or confused about SDB. The education campaign may have encouraged and enabled these members to understand why they should treat SDB and how to access appropriate treatment. We acknowledge that members may have changed their behavior because of other factors (eg, poor health, encouragement from a sleeping partner or primary care physician). Given the chronic nature of SDB, however, the temporal association between the education campaign and the uptake of PAP therapy supports our proposition.
Our results suggest that treatment of SDB can result in substantial savings for a health care plan. In the 2 years after the education campaign was initiated, the health care plan realized a differential saving of about $4.9 million for members with SDB who were treated with PAP therapy compared with those who were not treated with PAP therapy. The estimated return on investment was $200 PMPM for members enrolled in the SDB education campaign. People with SDB have higher health care costs than age- and sex-matched controls 1 ; in our study, both SDB groups had higher overall medical and inpatient hospital costs, and more hospital admissions than the non-SDB group. However, health care plans may realize cost savings if members with SDB are treated with PAP therapy. These savings are particularly substantial when members with obstructive sleep apnea are treated. In our study, the overall medical PMPM costs of members with obstructive sleep apnea were reduced 11.1% in the 12 months after starting PAP therapy. In cost-effective analyses of sleep clinic populations, the treatment of moderate-to-severe obstructive sleep apnea provides value to health care payers, with costs ranging from $2,000 to $11,000 per quality-adjusted life year. 16,21,22 In addition, health care plans may secure further savings as treatment of obstructive sleep apnea may diminish the risks of associated comorbidities, such as hypertension and cardiovascular events. 23
Interestingly, the SDB-PAP group had a higher prevalence of potentially costly comorbidities associated with SDB (eg, type 2 diabetes, hypertension) than the SDB-NT group. Health care costs of these comorbidities can be 2.5 times the health care costs of SDB, 5 and treatment of SDB is correlated with reduced medical claims for associated comorbidities and improved quality of life. 15,18,24 –27 Despite the higher prevalence of comorbidities in the SDB-PAP group, overall medical cost savings were generally lower in the SDB-PAP group than the SDB-NT group. The benefit of PAP therapy in terms of overall medical costs was more evident after, than before, the education campaign was initiated and, as such, the education campaign may have motivated increased adherence to PAP therapy among users. We did not directly address whether PAP therapy led to improvement in associated comorbidities. Nevertheless, it is possible that enhanced adherence to PAP therapy could have alleviated the symptoms and need for treatment of some of the comorbidities associated with SDB (eg, hypertension) 10 and, in this regard, helped reduce overall medical costs.
This study has some limitations. As we conducted a retrospective review of aggregated data, rather than a prospective analysis, we do not know if members in the SDB-NT group had been on PAP therapy before 2005, but opted to discontinue. In addition, as medical claims data do not account for therapies not covered by the health plan, we do not know if members were using different therapies or lifestyle modifications (eg, weight loss), successfully or otherwise, to alleviate their SDB symptoms. However, it is likely that most members in the SDB-NT group had been unsuccessful (to date) in their use of other therapies or lifestyle modifications as both hospital admissions and overall medical and inpatient hospital costs continued to rise for this group during the analysis period. We also recognize that the education campaign did not appear to affect the rate of diagnosis of SDB and may have targeted only those members motivated to improve their health. From the study, we cannot tell whether members with SDB remained undiagnosed, but we would expect that the increase in PSG testing would have helped identify suspected but undiagnosed SDB. The results of this study's population (ie, mostly males older than 50 years of age) may not be applicable to the general population. However, our results are applicable to health care plan providers of similar populations that have higher rates of SDB (eg, commercial vehicle drivers) 28 than the general population.
Conclusion
Our findings suggest that a low-cost, patient-focused SDB education campaign can improve health care outcomes and reduce medical expenses. In our study, members with SDB had higher medical expenses than members without SDB, but treatment with PAP therapy reduced medical expenses of members with SDB. Health care plans may realize considerable cost savings if their members with SDB are treated with PAP therapy. Implementing education campaigns that encourage health plan members to seek treatment for specific diseases may have merit and further study on the direct role these campaigns play on the overall medical expenses of health care plans is warranted.
Footnotes
Acknowledgments
This study was sponsored by ResMed Corp. (San Diego, CA). ResMed Corp. was involved with the authors in the study design, data collection, data analysis, and preparation of the manuscript. In compliance with the Uniform Requirements for Manuscripts, established by the International Committee of Medical Journal Editors, the sponsor of this study did not impose any impediment, directly or indirectly, on the publication of the study's results.
The authors acknowledge statistical analysis assistance provided by Olivia Parr-Rudd, M.S. and James Allen, M.B.A. The authors acknowledge the independent medical writing assistance provided by Julie Monk, Ph.D. and Karen Woolley, Ph.D. of ProScribe Medical Communications (
Disclosure Statement
Mr. Potts, Mr. Butterfield, Ms. Sims, and Mr. Henderson are employees of Union Pacific Railroad Employes Health Systems. Dr. Shames is an employee of and a shareholder in ResMed Corp.