
Abstract
The Patient Protection and Affordable Care Act of 2010 proposed sweeping changes to health insurance and health care delivery systems. As a result, local health departments, community health centers, and other safety net providers are expected to play a role in providing access to care for millions of individuals. This study examines the availability of population-based services by local health departments and community health centers in the Midwest/Great Lakes region. For this study, the authors used secondary data on location of community health centers collected by the Health Resources and Services Administration and local health department services delivery from the 2008 National Profile of Local Health Departments. To simultaneously examine the geospatial patterns of service delivery and location of community health centers, the geographic information system shape files of local health department jurisdictions were used to examine prenatal care services. Additionally, the effect of service availability was examined by analyzing the rate of low birth weight births within the service areas of these facilities. Results show large variation in the distribution of community health centers. Additionally, the analysis of local health department services shows that prenatal care services are not available in every jurisdiction. Furthermore, the rates of low birth weight births in these areas are significantly higher than in areas where prenatal care is available. Future studies are needed to examine the relationship between safety net providers as well as their role in improving population health. (Population Health Management 2013;16:270–275)
Introduction
The Public Safety Net
The public safety net is defined as those organizations and programs, in both public and private sectors, with a legal obligation or a commitment to provide direct health care services to uninsured or underinsured populations. 4 These providers include federally qualified health centers (FQHCs) and FQHC look-alikes, rural health centers, free clinics, and, in many areas, the local health department. The health care safety net can also include payment sources such as Medicaid and locally provided health plans for low-income and uninsured individuals. In 2000, the Institute of Medicine released a report that examined the effect of Medicaid managed care and welfare reform on the future integrity of the safety net. 5 Since that time, there has been a concern among policy makers that organizations that provide services to the uninsured or underinsured may not survive the declining resources and increasing demand for services. The Institute of Medicine report gained popularity again after the authors of this report reconvened in 2006 to take another look at the issue. Interest continued as the topic was hotly debated by presidential candidates in 2008. In response to a report issued by the Government Accountability Office, 7 Congress doubled the appropriations for community health centers to $2.1 billion. In addition, the American Recovery and Reinvestment Act of 2009 directed an additional 1-time appropriation of $2 billion. 6 The safety net continues to be an issue of concern as a growing body of evidence suggests that gaps in the availability and quality of services may put some communities at risk for health threats. 7,8 According to Mays et al, 8 a review of empirical studies published between 1990 and 2007 uncovered numerous gaps and uncertainties that influence the efficiency and effectiveness of public health delivery systems. These studies analyzed areas such as community health threats, healthy lifestyles, injury prevention, emergency preparedness, and resources available for good health. None of these studies specifically addressed gaps in the delivery of prenatal care and related health outcomes at a population level.
Community health centers
Community health centers are nonprofit, community-owned organizations that provide affordable primary and preventive care. Along with public hospitals and other providers, community health centers form the backbone of the health care safety net in the United States. 9,10 Community health centers are called by many names, including neighborhood health centers, family health centers, migrant health centers, and rural health initiatives. All community health centers meet the following 4 criteria: (1) Provide health care to medically underserved populations, (2) Provide a comprehensive range of primary care services, (3) Adjust charges for services based on patient income, (4) Governed by a community board, the majority of whom are patients. 10 These organizations operate using a combination of federal funding, grants, revenues, and private donations. According to a recent report, 7500 community health center locations served over 17.1 million people in 2008. 3
Community health centers provide comprehensive primary care that is culturally and linguistically appropriate, behavioral health care, case management, and use a whole-person approach to health. 10
Local health departments
Local health departments are responsible for creating and maintaining conditions that keep people healthy. Approximately 2800 health departments in the United States provide a wide array of services to diverse local communities. 11 Most local health departments are required by law to provide services to vulnerable populations within their jurisdiction and, as such, are called “providers of last resort.” 12 As part of the safety net, they strive to be effective in providing care for the uninsured and underinsured. In addition, local health departments are sometimes used as resources after community health centers turn away patients because of operational deficits. Often under-recognized, local health departments are major providers of maternity services in the United States. 13
Historically, local health departments serve women at the greatest risk for low birth weight and premature births, including the poor, uninsured, and adolescents. Studies show that women who receive publicly funded prenatal care received more health education than women in private practice, and were more satisfied with the information they received. 13,14 The percent of women who receive prenatal care directly from local health departments varies by state and within states by the availability of resources.
Dwindling public health budgets resulting from persistent economic recession have significantly hampered the ability of the safety net providers to operate successfully. 15 –17 Their ability to continue functioning within the current funding environment will hinge on how efficiently resources are used to produce the desired services and outcomes. Therefore, it is imperative to assess the gaps in service provision to build essential evidence for policy and practice. The objectives of this study are: (1) to examine the distribution of community health centers and local health department jurisdictions within the Great Lakes region, (2) to examine the distribution of maternal and child health services provided by community health centers and local health departments and identify spatial gaps in these services, and (3) to analyze the effect of the availability of services on population health outcomes. Although the authors' approach to mapping the gaps can be used for many other primary care services, prenatal care was selected because of its direct effect on infant mortality. Low infant mortality is an indicator of good population health status and access to primary care. 18 The authors selected low birth weight births for the population health indicator. Low birth weight is a primary factor affecting infant mortality. 13
Methods
Study population
This study focuses on 5 states in the Great Lakes region of the Midwest United States: Illinois, Indiana, Ohio, Michigan, and Wisconsin. Within this region, there are 432 local health departments and 1132 community health center locations. 19
Data and analytical methods
For this study, the authors used secondary data from 3 different sources. Data about services delivery of local health departments came from the 2008 National Profile of Local Health Departments, collected by the National Association of County and City Health Officials (NACCHO). The Profile study consisted of data from all 2794 local health departments in the United States at the time of administration of the survey in 2008. The complete survey technical documentation, including the instruments and code book, is available on the NACCHO Web site. 20 The Health Care Service Delivery Site data set was obtained from the Health Resources and Services Administration (HRSA) Web site. 21 This data set contained the locations of all FQHCs and FQHC look-alike health centers in the United States. From the larger data set, the authors extracted information for the 5 states that were of interest in this study. They also obtained geographic information system (GIS) shape files of local health department jurisdictions from the NACCHO. The GIS shape files of local health department jurisdictions were used to create maps of the Great Lakes region. Addresses of the community health centers were extracted from the HRSA data set and geocoded. ArcGIS (Esri, Redlands, CA) was used to map the distribution of community health centers throughout the Great Lakes region. Additional maps were created using the 2008 NACCHO National Profile Study 22 to examine the provision of prenatal care services and maternal and child health home visits as reported by local health departments. To examine the effect of service availability, information on low birth weight birth rates was collected from the Population Health Institute at the University of Wisconsin. More information on low birth weight data sources and measures can be found on their Web site. 23
Results
Table 1 shows the number of service areas of local health departments and community health centers within the 5 states used for the study. In addition, the table provides the average percentage of low birth weight births within the service area for all local health departments, including those with a community health center within the same jurisdiction, as well as the average for local health departments without a community health center. The table also shows the average low birth weight percentage for all community health centers, including those within a local health department jurisdiction and those that are outside the jurisdiction of a local health department.
SD, standard deviation.
Figure 1 shows the distribution of community health centers within local health department jurisdictional areas. The greatest concentrations of community health centers are within urban areas. Figure 1 also shows an absence of community health centers in many rural jurisdictions.
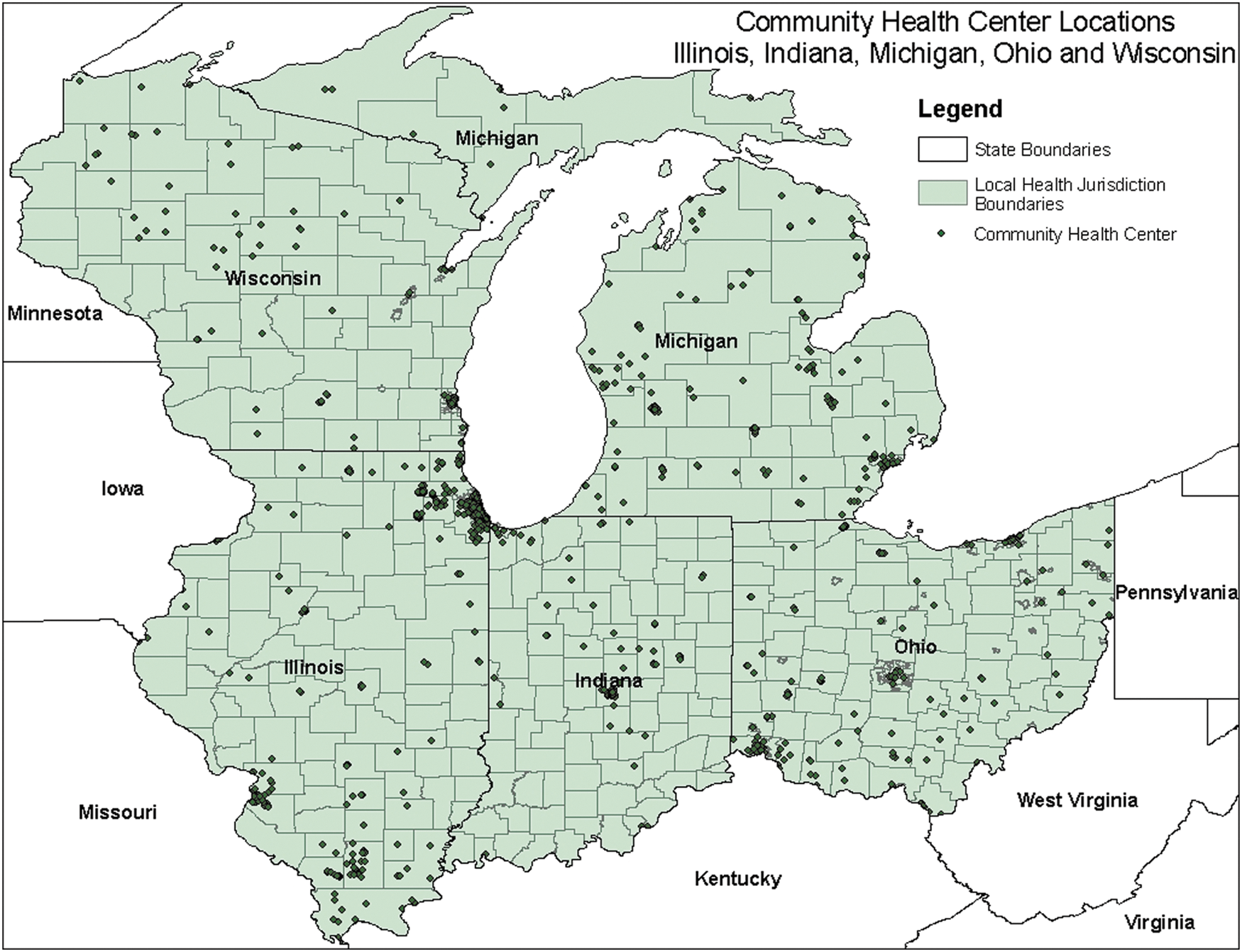
Community health center locations. A color version of this figure is available in the online article at
To account for variation in population density across local health department jurisdiction, the number of community health centers per 100,000 individuals within each area was computed, as shown in Figure 2. Of the 5 states, the state of Michigan shows the largest concentration of community health clinics per 100,000 individuals within local health department jurisdictions, while the state of Indiana shows the fewest community health centers.

Community health centers in local health department jurisdiction by population. A color version of this figure is available in the online article at
Figure 3 shows the availability of prenatal care services provided by local health departments in relation to the community health center locations. Most importantly, the map shows potential gaps in service where local health departments do not provide prenatal care services and a community health center is not present.
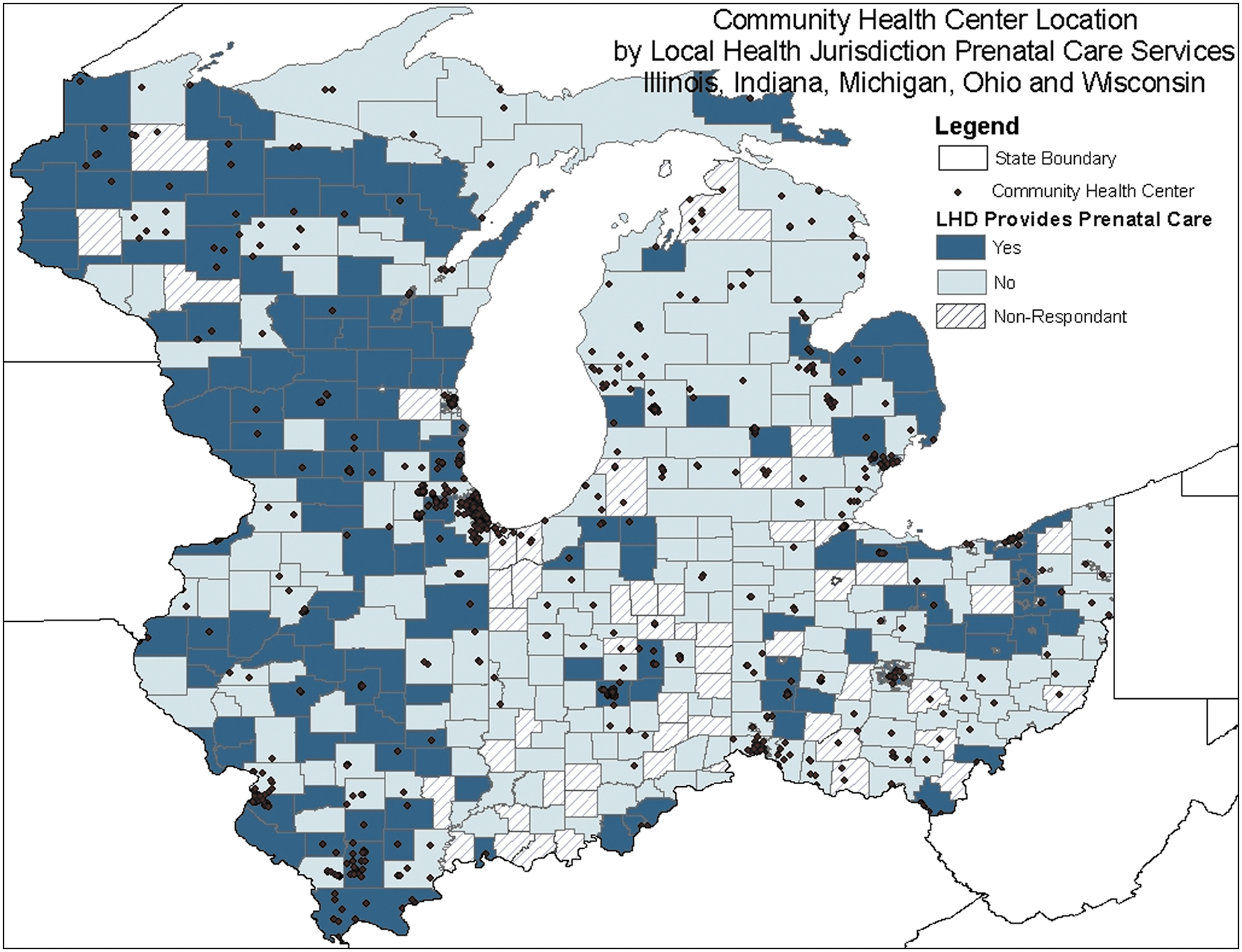
Local health department provision of prenatal care services and community health center locations. A color version of this figure is available in the online article at
Using low birth weight as a population-based indicator, the authors analyzed the relationship between the provision of prenatal care services within health department jurisdictions and the percentage of low birth weight births. Of the 319 local health departments in this analysis, 43% provided prenatal care services. The mean percentage of low birth weight births within the service area for this group was 6.96. In the service area for local health departments that did not provide prenatal care, the mean percentage of low birth weight births was 7.32. The data show a significant difference in the mean percentage of low birth weight births (F=7.30, P=0.007) in local health department service areas that provided prenatal care services when compared to areas that did not provide this service (Table 2).
Mean percentages are statistically significant (P=0.007). SD, standard deviation.
Discussion
Assessing gaps in service provision is an essential first step to assuring access to population health services. This study demonstrates that geospatial analysis can be used effectively for this purpose. This study focuses primarily on community health centers and local health departments within the safety net because of the leading roles these governmental agencies play in providing health services to the poor and uninsured. According to the Kaiser Commission on Medicaid and the Uninsured, these patients account for almost 75% of health center caseloads. 3 Likewise, a recent study of local health departments reported that 27% of patients were poor and 63% were nonwhite or Hispanic. 24 According to the HRSA Uniform Data System, 7.6% of Illinois residents, 4.7% of Michigan residents, 3.5% of Wisconsin residents, 3.4% of Indiana residents, and 3.3% of Ohio residents received health care from community health centers in 2008. 6
The study also highlights that there are significant gaps in the public safety net in maternal and infant health services by GIS mapping the distribution of safety net facilities and linking the availability of prenatal care services to the percentage of low birth weight infants within local health department service areas. The availability of prenatal care services from a safety net provider is related to a lower percentage of low birth weight deliveries within the population. Such empirical evidence can help improve efficiencies in public health by identifying areas of greatest need and targeting the delivery of services to these areas. Local health departments are major providers of maternity services to low-income and uninsured women. 13 However, with reduced financial and workforce capacities, local health departments are expected to do more with fewer resources. 15 Local health departments attempt to reduce the impact on the population by working closely with alternative providers in the area. 25 This elevates the importance of studies that examine the coexistence of various safety net providers in communities across the United States. Research designs and measurement strategies used in the field of network analysis may provide direction for future studies to examine coordination among safety net providers.
This study is limited by the following issues: the health indicators currently available are restricted because of the small unit of analysis used in this study. The unit of analysis used in this study is county (recognized by county Federal Information Processing Standard code). Health indicators commonly used to assess maternal and infant health on a population level include education and age of the mother, insurance status, prenatal care origination, maternal and infant mortality, and behavioral risk factors such as tobacco use and obesity. 26 –28 Other indicators of infant health include gestation period, Apgar score, abnormal conditions, and congenital abnormalities. 28 –30 Including these types of measures (if available) would strengthen the study. However, data from smaller counties were unavailable because of the low numbers and the potential for identification of subjects.
Another limitation is incomplete information from community health centers. Services vary widely by community, and the availability and quality of services in a given jurisdiction is difficult to describe across a wide range of counties and states. Furthermore, a community health center within an area may not have sufficient capacity to meet the needs of the population. Conversely, residents of a certain local health department jurisdiction may find it more convenient to obtain services across the administrative boundary of their local health department. Future studies are needed to examine the relationship between safety net providers, as well as the contributions of other organizations to improving population health. Other contributors include community and faith-based organizations, health care providers and insurers, social service agencies, and private businesses. 8 Additional indicators should be identified and made available to study the relationship between access to services and population health outcomes.
Like other sectors of the economy, safety net providers have experienced financial and workforce reductions since 2008. 15 However, during this same period, demand for services increased. The PPACA provides $11 billion to FQHCs over the next 4 years. In addition to the $1.5 billion set aside for capital improvements, funds also are provided to support primary care residency programs that support the goal of providing high-quality, low-cost primary care. Moving ahead, the PPACA is expected to reduce some of the challenges previously faced by safety net providers by reducing the rolls of the uninsured, enhancing compensation for primary care providers, and expanding the community health center infrastructure.
Footnotes
Acknowledgments
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was support by a grant from the Robert Wood Johnson New Connections Program. The authors would like to thank Fatema Mamou, M.P.H., lecturer (University of Michigan-Flint) and epidemiologist, who served as the GIS consultant on this project.
Disclosure Statement
Drs. Mathis, Barnes, and Shah declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.