
Abstract
The US health care system is currently heading toward unsustainable health care expenditures and increased dissatisfaction with health outcomes. The objective of this population-based study is to uncover practical insights regarding patients with 1 or more chronic illnesses. A cross-sectional investigation was designed to gather data from health records drawn from diverse US geographic markets. A database of 9.74 million fully-insured, working individuals was used, together with members in the same households. Among nearly 3.43 million patients with claims, 2.22 million had chronic conditions. About 24.3% had 1 chronic condition and 40.4% had multi-morbidity. Health care expenditures for chronic conditions accounted for 92% of all costs (52% for chronic costs and 40% for nonchronic costs). Psychiatry, orthopedics-rheumatology, endocrinology, and cardiology areas accounted for two thirds of these chronic condition costs; nonchronic condition costs were dominated by otolaryngology, gastroenterology, dermatology, orthopedics-rheumatology conditions, and preventive services. About 50.1% of all households had 2 or more members with chronic conditions. In summary, multi-morbidity is prevalent not only among those older than age 65 years but also in younger and working individuals, and commonly occurs among several members of a household. The authors suggest that the disease-focused model of medicine should change to a more holistic illness-wellness model, emphasizing not only the physical but also the mental and social elements that can influence individual health. In that way the chronic care model could be broadened in context and content to improve the health of patients and households. (Population Health Management 2013;16:381–389)
Introduction
A
New evidence indicates that single and multiple chronic conditions are prevalent not only in the US elderly population (≥65 years of age), but also in the working age population (18–64 years). 3 A US survey of 58,408 individuals suggests that 51.8% had single and multiple (ie, multi-morbidity) chronic conditions. 3 However, these findings lack details about their clinical profiles and health care utilization patterns. Knowledge of actual clinical conditions is essential to gain insights into the pattern of multi-morbidities and associated health care utilization. Consequently, to accomplish substantive change, this information must be incorporated into clinical projects intended to improve the quality and affordability of care. This article will discuss practical insights with respect to cohorts of working age individuals with 1 or more chronic illnesses, with the longer term goal of better aligning the US health care system to achieve sustainable healthier lives and health care expenditures.
Methods
Study design and population
A cross-sectional 39-month (January 1, 2008 through March 31, 2011) study was conducted using a population-based health plan administrative database. The database covered 9.74 million consisting of fully-insured working individuals and their dependents. It spanned diverse geographic markets across the continental United States.
Identification of single morbidity and multi-morbidity
Administrative databases were analyzed as a function of single and multiple chronic illnesses, with multi-morbidity signifying the coexistence of 2 or more chronic conditions. Medical conditions were defined using the Episode Treatment Groups® (ETG®) illness classification methodology, which identifies chronic conditions (persisting >1 year) as well as conditions that are not chronic. Single morbidity and multi-morbidity were defined as the unique number of chronic ETG episodes for an individual in a 39-month period. 4
Health care economic outcomes
Health care expenditures were quantified in terms of allowed amounts, defined as the payments made to the provider via the benefit plan plus deductibles, co-payments, and coinsurance paid by the patient, as applicable. The total amounts allowed include those for management (office visits), surgical procedures, facility (room and board), ancillary inpatient and outpatient services, and pharmaceuticals.
Data analyses
To manage analytic complexity, conditions were rolled up in terms of predefined ETG Major Practice Categories (MPCs). For example, diabetes and hypothyroid disease were rolled up into the endocrinology MPC. For an MPC, a proportion was calculated as a ratio of the sum of ETG episodes in a given MPC to the total number of episodes across all respective MPCs in a given time period within a single-morbid or multi-morbid cohort. For a condition, a proportion was computed as a ratio of the number of unique individuals for a given condition to the total number of unique individuals across all types of conditions in a given cohort. The latter calculation was performed to examine the disease frequency in patient cohorts defined by the number of chronic conditions. All calculations were performed using SAS Enterprise software (SAS Institute Inc., Cary, NC).
Results
Patient count, frequency, and health care spending as a function of number of chronic conditions
Among 3.43 million patients with claims in the analysis period, with 2.22 million had 1 or more chronic conditions. Single-morbid chronic patients accounted for 24.3% (830,000) of those with claims, with multi-morbid individuals comprising 40.4% (1.39 million) of the claimants (62.4% of all patients with chronic disease). As depicted in Figure 1, the number of patients decreased as the number of chronic conditions increased. About 91.6% of multi-morbid patients were noted to have between 2 and 6 chronic conditions; patients with 2 or 3 chronic diseases accounted for 61.5% of the multi-morbid population. In this population of fully-insured, working individuals, only 6.7% were older than the age of 65.
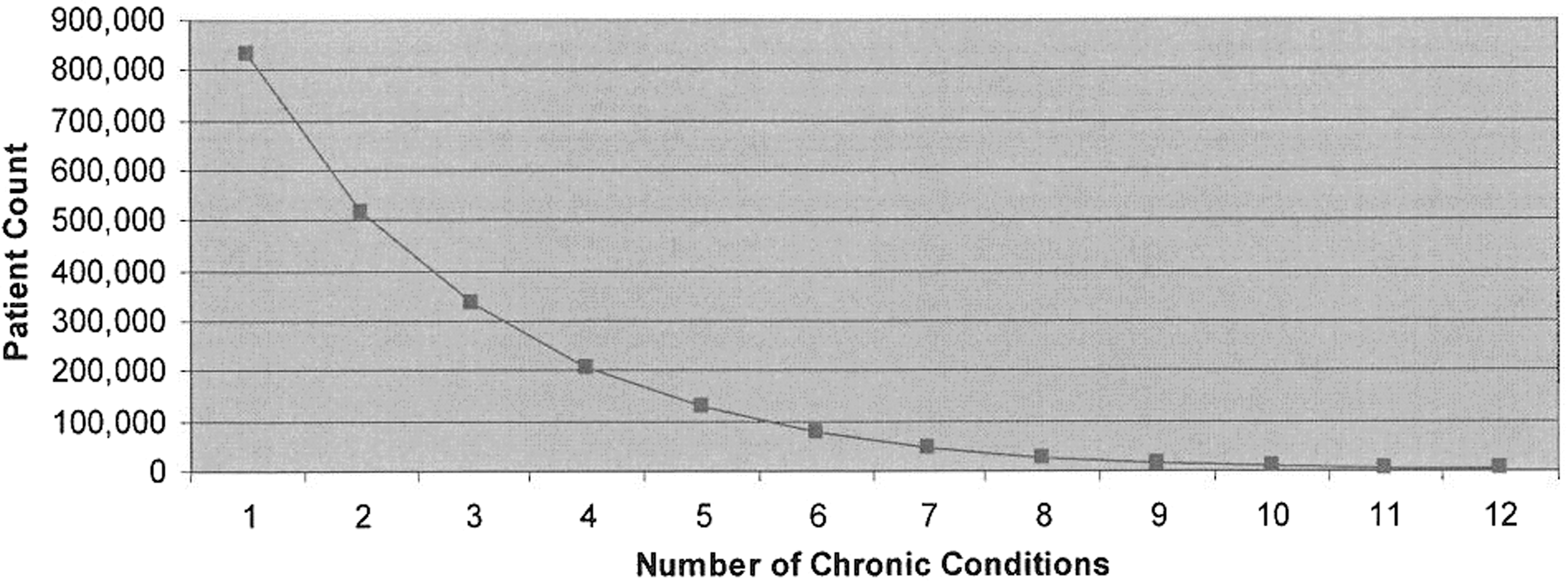
Patient count as a function of the number of chronic conditions.
Patients with chronic conditions accounted for 92% of all health care expenditures over the time period studied. Services related to their chronic conditions were responsible for 56.5% of their health care expenditures (52% of total claim costs) with the services for nonchronic conditions accounting for the remaining 43.5% of their costs (40% of total claim costs). The total allowed amounts are displayed in dollars (Fig. 2a) and relative terms (Fig. 2b) as a function of the number of chronic conditions for both chronic and associated nonchronic conditions. All dollar amounts are annualized across the full 39-month period. The associated nonchronic costs exceeded those of chronic costs for patients with 1 or 2 chronic conditions, thereafter declining relative to chronic costs and reaching a plateau at approximately 8 chronic conditions (39% of chronic costs). The average cost for multi-morbid patients was almost 4 times that of single-morbid patients (Fig. 3). Furthermore, when compared to the average costs of the population with only nonchronic conditions, the average costs of multi-morbid patients were 8-fold higher and single-morbidity chronic condition patients were about 2-fold higher.
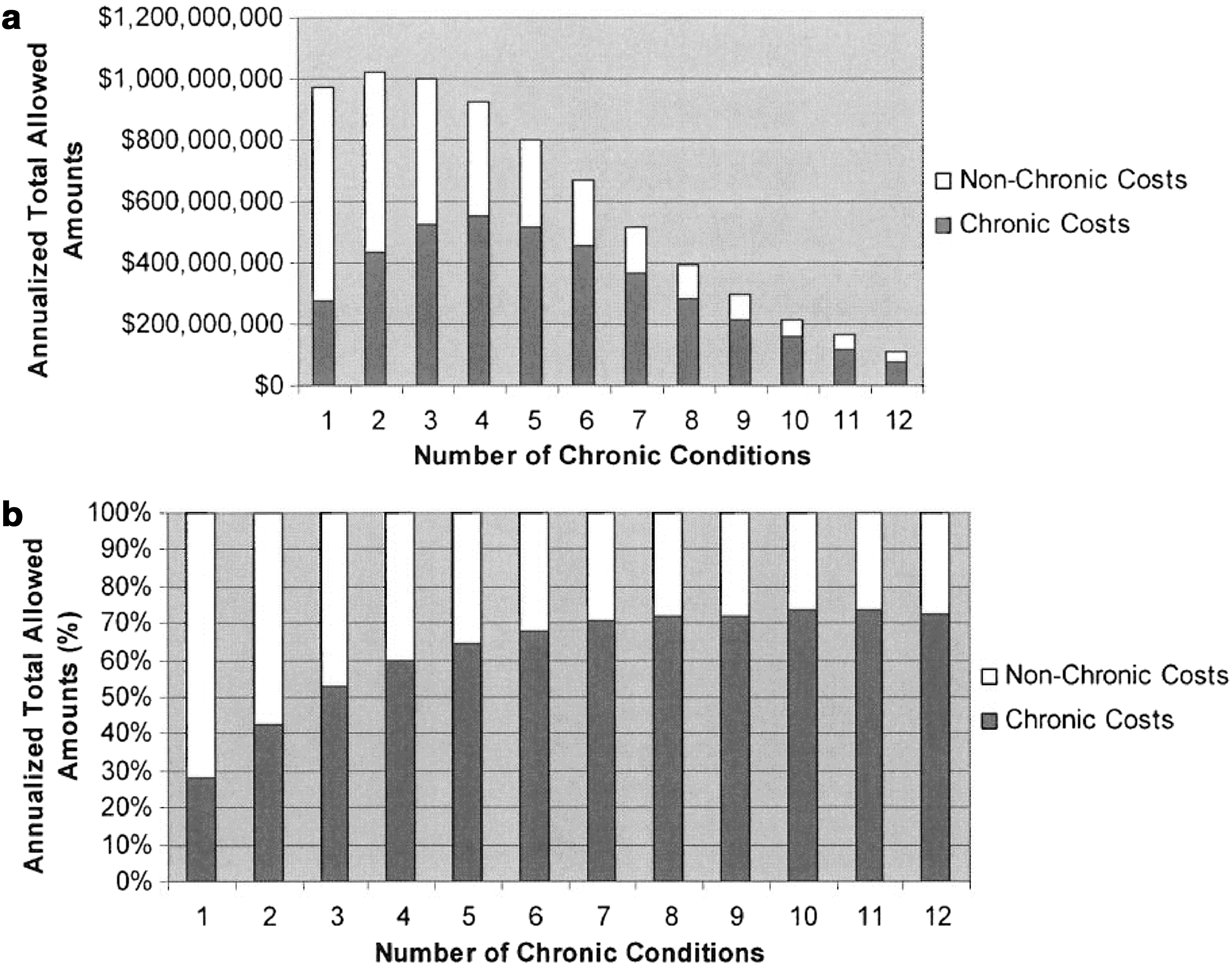
Annualized total spending as a function of the number of chronic conditions.
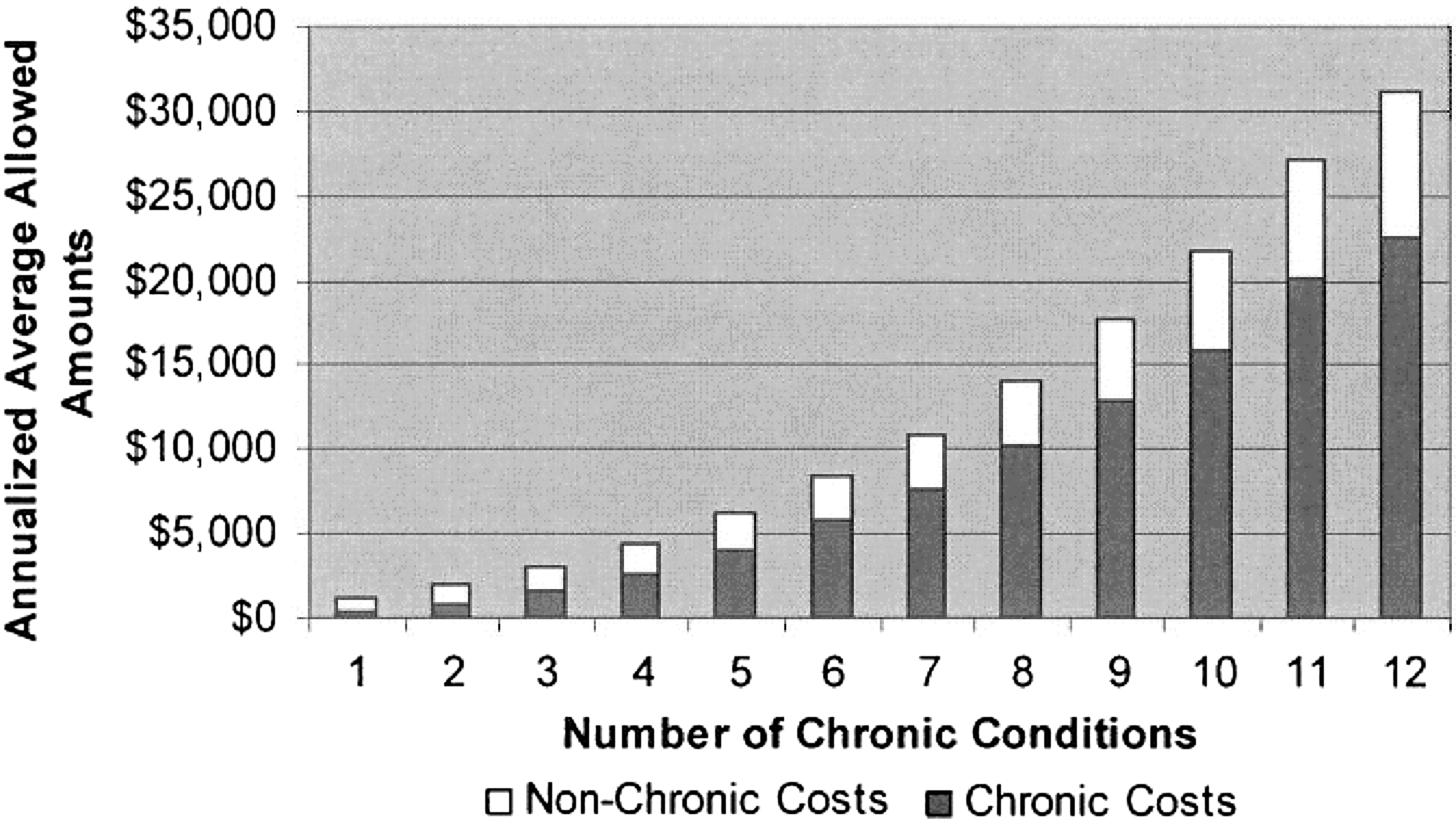
Annualized average spending per patient as a function of the number of chronic conditions.
About 49.9% of all households had a single member with chronic conditions. The remainder of households had 2 or more members with chronic conditions, with 29.4% having 2 members with chronic illnesses, 13.3% having 3 members, and 7.4% of households having 4 or more members with chronic illnesses. Households with more than 1 member with chronic conditions accounted for 51.1% of all the costs for the chronic population. Among the remainder, households with 2 members with chronic conditions were responsible for 32.5% of all costs, households with 3 members with chronic conditions were responsible for 11.9% of costs, and households with 4 or more members with chronic conditions were responsible for 6.7% of all costs.
Frequency of chronic medical practice categories and conditions, linked to nonchronic practice and conditions
Table 1 shows the distribution of chronic MPCs. In general, endocrinology, orthopedics-rheumatology, cardiology, and psychiatry accounted for almost two thirds of chronic morbidities. For example, endocrinology episodes as a proportion of all episodes increased between 1 and 3 chronic conditions and then declined for 12 chronic conditions.
Table 2 breaks chronic MPCs down into the most prevalent specific conditions. For example, the proportion of diabetes in endocrinology increased steadily with an increase in the number of chronic conditions. Furthermore, other prevalent conditions increased with an increase in the number of chronic conditions. For patients with 12 chronic conditions, hypertension recorded the highest proportion and anxiety disorders the lowest. For patients with 1 chronic condition, however, hyperlipidemia was the most frequent chronic condition and ischemic heart disease the least frequent.
Otolaryngology, gastroenterology, dermatology, orthopedics-rheumatology, and preventive-maintenance episodes were the most frequent nonchronic MPC linked to chronic conditions. They accounted for 54.4% of all nonchronic episodes with each averaging 10.8% (Table 3). Orthopedics and rheumatology was the only MPC to reach double digits in both chronic and associated nonchronic conditions. Its presence was consistent in both single and multi-morbid patients. The most prevalent nonchronic conditions are also shown in Table 4.
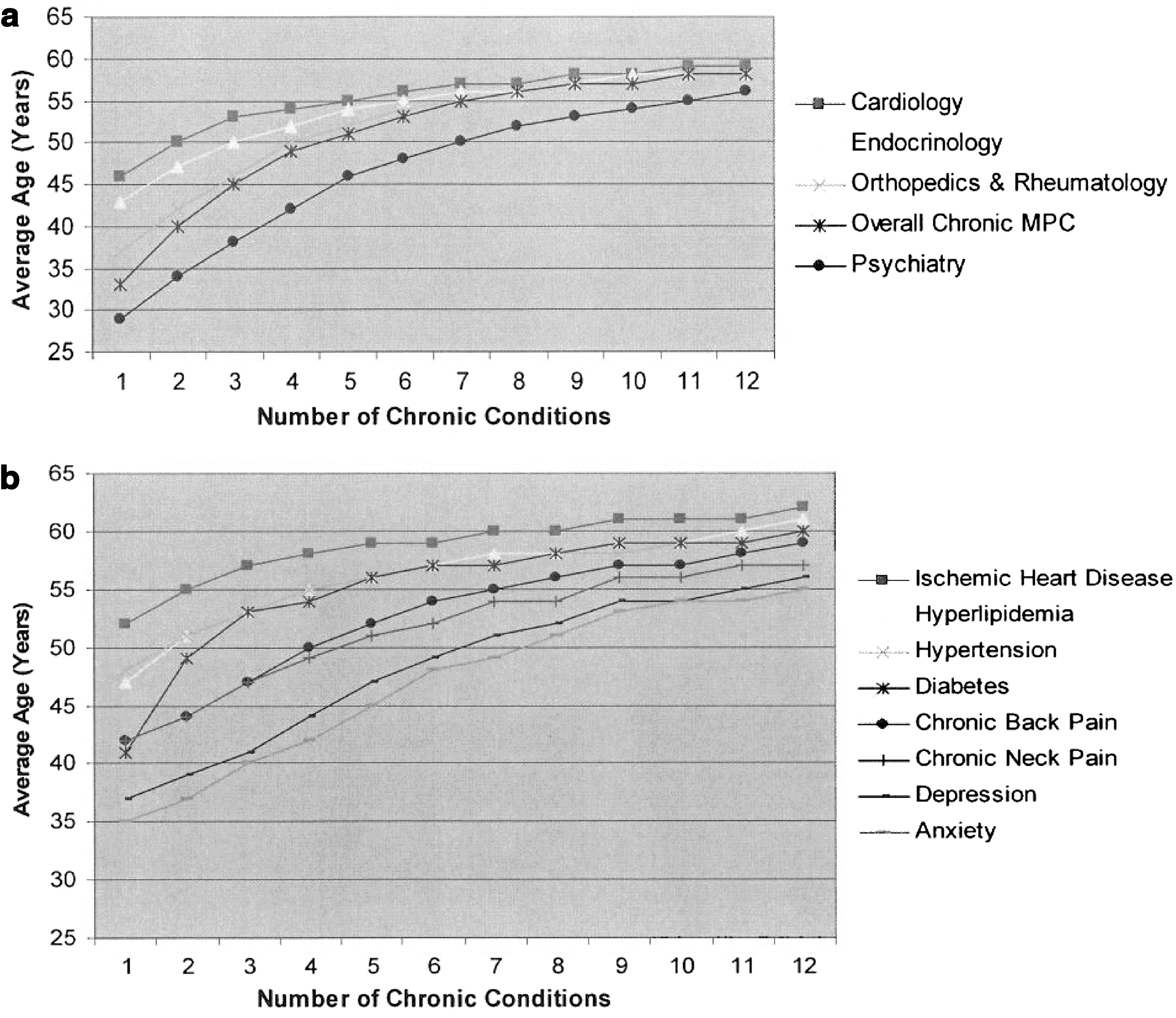
Figure 4a shows the relationship between average age and number of chronic conditions for chronic MPCs. The average age for persons with psychiatric conditions was consistently lower than that of other chronic MPCs and also was below the average age across all MPCs. In particular, depression and anxiety had the lowest average ages as a function of the number of chronic conditions (Fig. 4b). The average age for persons with orthopedics and rheumatology cases was consistently lower than those for endocrinology and cardiology for patients with 1 to 7 chronic conditions.
Overall, the average age for nonchronic MPCs was 2 years less than that of chronic MPCs with 1 to 4 chronic conditions, and then fluctuated between 1 and 2 years for 5 to 12 chronic conditions (Fig. 5). Patients with otolaryngology conditions were consistently younger than the average age across all nonchronic MPCs. Patients with gastroenterology conditions were consistently older than the average age for all nonchronic MPCs, as well as being older for between 1 and 6 chronic conditions for chronic MPCs. Dermatology conditions had average age equal to that for overall nonchronic MPCs.

Age as a function of the number of chronic conditions for nonchronic Major Practice Categories.
Discussion
Frequency and health care spending of multi-morbid patients in working and younger individuals and households
An analysis of a large administrative database has shown that multiple chronic conditions are common in an insured US population of younger and working individuals and families. The chronic conditions consisted of predominantly cardiovascular, endocrine, orthopedic-rheumatologic, and psychiatric conditions, and commonly occurred in more than 1 member of a household. Furthermore, in every cohort of patients with 1 to 12 chronic conditions, the average ages increased for conditions in a predictable order, with psychiatric conditions being the lowest and increasing in the following order: orthopedics and rheumatology, endocrine, and cardiovascular conditions. Collectively, the authors believe these results have significant implications for the sustainability of health care expenditures and the improvement of health care quality in the United States.
In this study, multi-morbidity accounts for 62% of all chronic conditions and 86.8% of total chronic costs. The prevalence of multi-morbidity is greater than the 52% value reported elsewhere 3 in a much smaller US sample. In addition, 2 or more members with chronic conditions in the same household constitute 50.1% of all chronic conditions and 51.1% of all respective costs. This issue has not been addressed previously and, therefore, the authors feel requires further attention. Interventions aimed at all noted multi-morbid conditions for both the household and the individual may be necessary, and actually may be a more cost-efficient approach. These findings truly amplify the role of the social element in health. As rightly stated by Smith and Christakis, “People are interconnected and so their health is interconnected.” 5 Future research is warranted in this important area of study.
Holistic view of multiple chronic illnesses
Traditionally, disease and case management programs are designed to treat chronic disease patients for an index condition. It is customary to tackle the few percent of highest risk patients in these programs, with the logic that such actions will stabilize the medical conditions of patients and make health care expenditures sustainable. According to the present study's findings, these patients would be located in the predictable high-risk and cost cohorts of 8 or more chronic conditions, where chronic costs plateau (Fig. 2b). Although annual health expenditures per person in those cohorts are high (11 times relative to that of a person with between 1 and 3 chronic conditions), the number of patients is much lower (3.1% of the chronic population) relative to the number of patients who have between 1 and 3 chronic conditions (75.9% of chronic population). Furthermore, the total health care expenditures for patients with 8 or more chronic conditions (19.6% of all chronic costs) are about half the costs of those patients with 1 to 3 chronic conditions (40.8% of all costs). The authors suggest, therefore, that the focus should be expanded to include those cohorts with 1 chronic condition and lower level multi-morbidity if US health care costs are to become sustainable.
Early control of multi-morbidity requires an in-depth understanding of the interplay among all psycho-socio-physical influences on chronic conditions. Wade and Halligan argued the presence of 3 faulty assumptions that do not allow one to fully explain many forms of illnesses in health care: any illness has a single underlying cause, disease is always the single underlying cause, and return to health is a consequence of removal or attenuation of disease. 6 The present findings, for example, show that the average age associated with chronic psychiatric conditions is consistently lower than those for other dominant MPCs. These psychiatric conditions may be a factor that triggers conditions in other MPCs, hence, leading to higher multi-morbidity levels. Collectively, one can infer that further research is warranted to explore the dynamic interplay among the physical, mental, and social elements of health to improve the outcomes and costs of chronic care.
Based on the foregoing discussion, the present findings lend support to a holistic view of chronic illnesses in at least 3 ways. First, it is more useful to address patient-level multi-morbidity than to divide patients into individual index disease states. Attempting to classify patients by specific combinations of chronic diseases quickly runs into, among other problems, a Cartesian product of combinations (eg, diabetes with/without hypertension). Second, the multi-morbidity view is more person-centered than a traditional medical classification. The latter approach is commonly criticized by patients: “I am not a case of diabetes, I am a person with diabetes and other issues.” Multi-morbidity reflects the total medical experience of a person. Lastly, the holistic view finds age-related patterns among mental and physical multi-morbid conditions. For example, in the authors' experience as well those of others, the specific orthopedic conditions are often presentations of underlying chronic pain that has significant overlap and interaction with depression and anxiety. 7
Adopting a holistic view of chronic illnesses resonates with other authors who have called for an integrated approach to cardiovascular morbidity rather than the traditional disease-specific practices. 8,9 The authors caution, however, that multi-morbidity should not be confined to a particular disease category; rather, it should be integrated as relevant across medical, behavioral, and social aspects of health. This issue also relates to the combinations of chronic conditions present in a given patient and warrants further research. This view is shared by the authors of the 2011 proposed national strategy for multi-morbidity. 10 The notion of a holistic view does not suggest discarding disease-focused clinical guidelines in favor of new ones for multi-morbid patients. Rather, one should adopt relevant guidelines and develop others as needed. In this respect, the evidence-gathering process for multi-morbidity should not be based only on knowledge generated from randomized clinical trials, which work by isolating factors to determine their effectiveness with respect to treatment effects. Multiple chronic conditions involve time, observation, and medical complexity. Thus, one must search for integrated solutions to provide individualized care for the multi-morbid patient. 11
A suggestion for revisiting models of care for multi-morbid patients
As pointed out in the previous section, the frequency and costs of multi-morbidity require a holistic perspective in terms of care management. Consequently, a number of researchers have voiced the need to shift the focus of care models from single diseases to a patient-centered approach in order to address the needs of multi-morbid patients. 11 –13 The US Department of Health and Human Services (HHS) pointed out that current models of care do not explicitly address the needs of patients with multiple chronic conditions. 10
In light of this, the authors suggest that there is a need to revisit the composition of and relationships among key participants in health care for persons with multi-morbidity. Older care models, which are disease focused, stressed the doctor–patient relationship. Wagner's chronic care model added community resources and health systems. 14 Health plans and payers also must be considered, because they have an important role in care management (eg, care coordination, disease and case management, patient and physician data reporting, and incentive programs. The present findings show an additional, missing element—the household member—who more often than not also has multi-morbidity and may act as a caregiver to the patient. An effect on caregivers is consistent with the findings of others. 15 Therefore, the authors suggest that the smallest unit of health care is the tetrad of patient, physician, payer, and household member/caregiver (Fig. 6). The tetrad is embedded in a larger social context, but the authors believe further consideration of this basic unit would be an important step toward understanding and transforming health care.
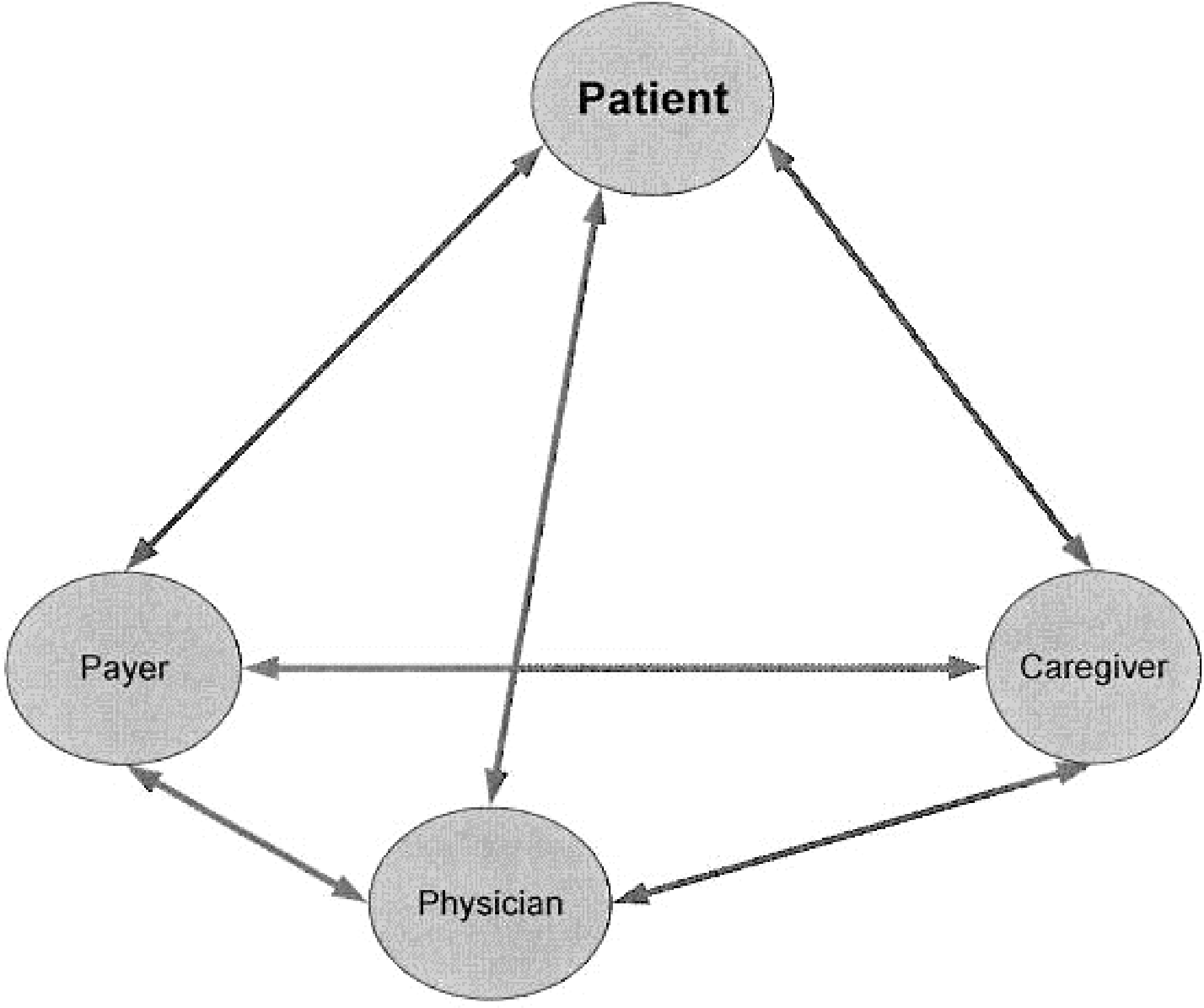
Smallest unit of health care, a tetrad of key participants.
Wagner's chronic care model has been an important innovation in enlarging care from the patient-physician relationship perspective. 14 However, in its current version it is incomplete and does not account for the role of and value added to/from stakeholders, with particular emphasis on the medical complexity embedded in multi-morbidity. The chronic care model emphasizes that the provider team is responsible primarily for the treatment process of chronic care. Although it calls for the involvement of an informed and activated patient, it does not explicitly recognize that patients, household members, and caregivers are essential and interacting stakeholders in patient-centered care. A more comprehensive approach that starts with the health care tetrad would allow us to focus on the roles, added values, and interactions of the 4 stakeholders. By emphasizing the relationships among stakeholders, the approach adds to the list of goals and objectives outlined in the HHS strategy. 10
Although the proposed framework is supported by the data presented and could be expected to work on theoretical grounds (as it takes into account important aspects of prior models), further research is warranted to further advance the science of care models within the context of multi-morbidity. In this respect, a systematic review, a critical appraisal, and a meta-analysis would be an important next step to compare the cost-effectiveness and clinical impact of prior care management models (eg, population health models) with a focus on multiple chronic diseases to the proposed framework.
Collectively, the multifaceted aspects of the present study results call for the synthesis of integrated health care solutions grounded in care management along medical, behavioral, and social lines. The evidence for these solutions must be gathered from a variety of quantitative and qualitative learning vehicles in incremental yet significant ways to accelerate the process. In recent years, a hierarchy of evidence for assessing qualitative health research has been building up20 to fill up the gaps in evidence-based medicine, particularly for chronic care management and prevention. An innovative health economic model also will be required to document the benefits of proposed care interventions in terms of positive health and not merely disease avoidance and treatment. Economic valuation methodologies must account for both material and meaningful actions to properly calculate the true returns on short- and long-term investments in health care when building healthier lives.
Study limitations
One must acknowledge the study limitations to keep in perspective the implications of the findings reported herein. The study is a cross-sectional investigation based on a 39-month analysis period. Consequently, the results obtained do not establish cause–effect relationships. The data were extracted from claims databases, which have inherent limitations on clinical information. To protect against coding errors, the ETG condition classification system uses only codes based on face-to-face visits (as opposed to codes on radiology or laboratory claims). In addition, ETGs use a clinical hierarchy to assign the most accurate disease descriptor over a course of an episode. The authors believe these techniques mitigate the limitations of administrative data. Also, much mental health data was unavailable because of separate handling by a behavioral health management firm. However, any missing mental health data would only have strengthened some of the arguments above. Despite these limitations, the large sample was representative of diverse geographic markets and allowed the authors to uncover practical insights that may stimulate future research that will lead to the radical improvement of health care quality and reduction of health care expenditures for multi-morbid patients and families.
Footnotes
Author Disclosure Statement
Drs. Greene, Dasso, Ho, Frank, and Genaidy, and Mr. Scandrett declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for the research, authorship, and/or publication of this article.