
Abstract
CCA's efforts responded to interest from leading policy and government advisory organizations, including the Medicare Payment Advisory Commission and the Centers for Medicare and Medicaid Services (CMS) Medicare-Medicaid Coordination Office. In reviewing concerns of these advisory and regulatory groups, CCA identified a profound gap in the literature and case studies on models of care for dual eligibles; specifically, a severe lack of information on how to effectively design and implement programs that coordinate care for dual eligibles to improve health outcomes and achieve cost savings. This finding presented an important opportunity for population health management (PHM) industry members, whose expertise with care coordination for dual eligibles can significantly improve related health policies. By definition, PHM programs include a rich menu of services that assess health risks, engage patients, and deliver evidence-based interventions that are carefully tailored to the needs of specific populations. No single document aggregated the experience of PHM industry stakeholders and explained how these programs naturally provide a framework for care delivery for dual eligible populations. This placed CCA's Work Group in an ideal position to lead other health stakeholders down the path toward innovative strategies in care delivery and financing for dual eligibles.
Guided by CCA's PHM framework (Fig. 1), the Work Group drew on experience in the field to create an outline of the core features necessary in any health care delivery model to achieve coordinated care, improved health outcomes, and cost savings for dual eligibles. This project launched in the fall of 2011 and culminated in a formal policy paper released in March 2012 during a standing room only Congressional Briefing on Care Coordination for Dual Eligibles. CCA organized the briefing in collaboration with Representative Bill Cassidy (R-LA), who delivered compelling opening remarks on the imperative of addressing the health needs of dual eligibles through care coordination and other PHM strategies. Speakers shared real-world experience and data on care coordination strategies for dual eligibles from the perspectives of health plans, care management companies, state Medicaid directors, technology, and specialty services stakeholders. The packed audience and robust dialogue on speaker presentations confirmed that health policy makers have strong interest in further education on core components of models for dual eligible populations that successfully coordinate care, improve health outcomes, and achieve cost savings.
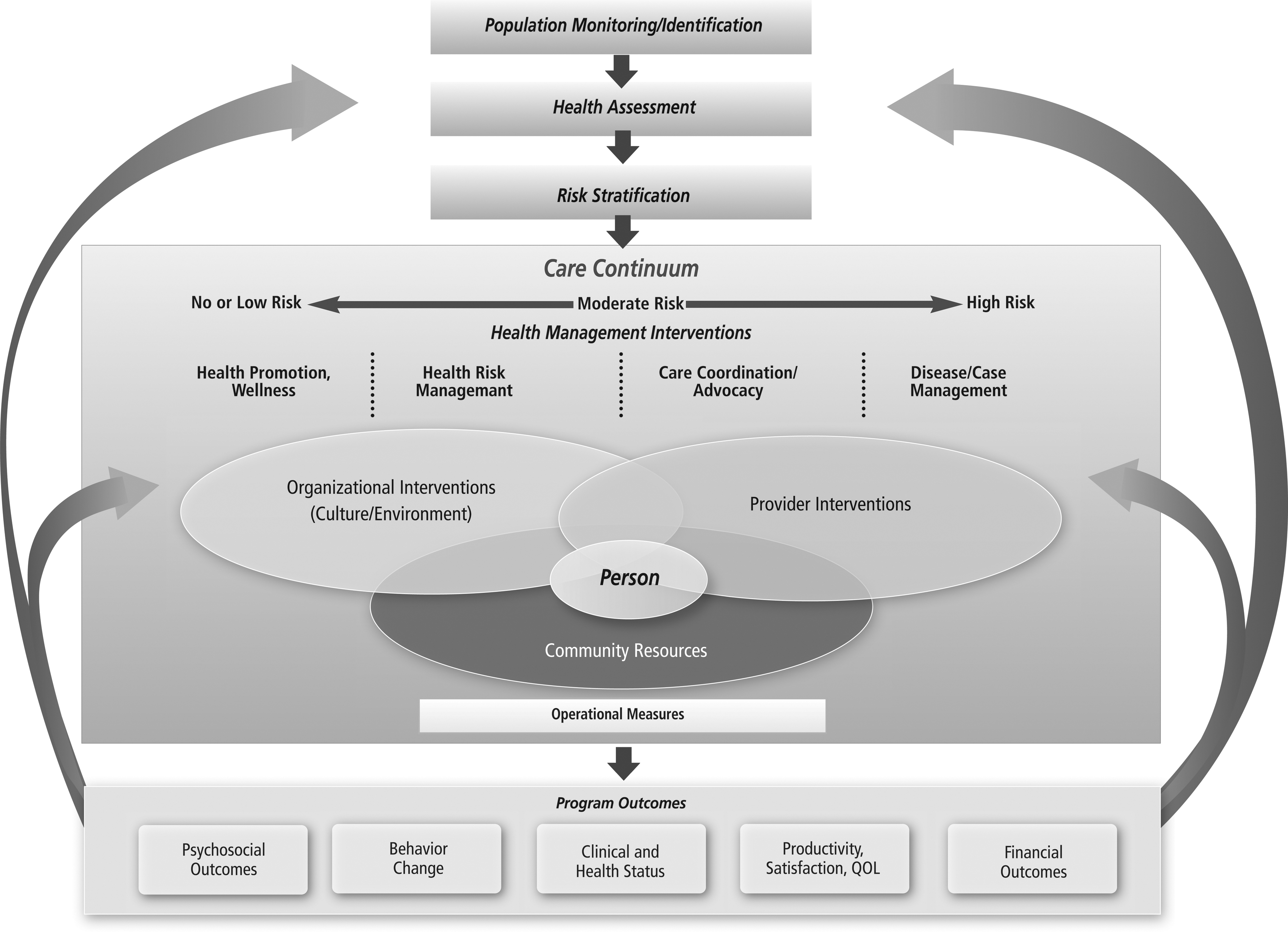
Care Continuum Alliance's population health management framework.
The policy paper defines core programmatic components of care delivery models intended for dual eligibles. Much of the experience reflected in the policy paper grew out of collaborative partnerships with health industry stakeholders working to design care delivery models that address the diverse needs of dual eligibles. Although many health care stakeholders, including federal and state governments, have spent years searching for policy strategies to improve care coordination in dual eligible populations, a lack of consensus and uncertainty persists.
This policy paper marks an important step in convening our industry to establish consensus on the core components necessary to design any dual eligible model of care. The positive attention and wide acclaim CCA received for the paper suggests industry consensus around policy strategies that have demonstrated success in care coordination, improving health outcomes, and cost savings for dual eligibles. The policy paper neatly captures insights from industry experience for the first time and works toward addressing the gap in literature on how to design and implement successful models of care for dual eligibles. This guide will be valuable to many important stakeholder groups seeking immediate solutions in care coordination for duals eligibles, such as policy makers, provider networks, and community health collaboratives. It also demonstrates how PHM approaches to care coordination for dual eligibles and individuals nearing this status can successfully improve health outcomes and achieve cost savings for this population.
The data behind this policy paper highlight positive outcomes and cost savings in many health care utilization areas addressed through PHM programs. Specifically, the evidence shows reduced utilization of nursing facilities, decreased hospitalizations, and improved medication adherence. This makes a strong case for underpinning models of care intended for dual eligibles with these core programmatic components.
Core Components of Care Coordination and Care Management Programs in Dual Eligible Populations
CCA outlined the following core components as an ordered system to build care delivery models that successfully improve health outcomes and achieve cost savings for dual eligible populations.
Component 1: Centralized, Comprehensive and Interconnected Data
The Problem
Insufficient or untimely data severely hinder care coordination for dual eligible populations. It impedes the ability of stakeholders to identify health risks and needs, communicate regularly, accurately tailor health care interventions, educate patients and care providers, and evaluate program outcomes. Without this information, stakeholders have a severely limited understanding of where patients fall on the continuum of care. This leads to significant clinical and financial risks for stakeholders related to inaccurate perceptions of patients' health status, health risks, and needs. The procedural hurdles that state Medicaid programs face when seeking access to Medicare data exemplify this problem. Although the sensitivity of Medicare data must be considered, access to this data is critical to achieving shared goals of the federal government and states for care delivery for dual eligible populations. Without easily accessible, comprehensive, connected data, stakeholders cannot accurately assess patient health or make value-based determinations about which strategies and interventions are clinically appropriate and patient-centered. This contributes to unnecessary, fragmented, duplicative care and higher health costs.
The Solution
Access to sufficient, accurate, and timely data is necessary to understand patients' increasingly acute health needs and to intervene before the next health episode occurs. It is the first building block of a successful program to coordinate care for dual eligible populations and intimately ties to all subsequent core components in CCA's guide. Through data resources, such as pooled aggregated databases and health information exchanges, care providers will be able to evaluate a patient's health status based on the whole patient, rather than fractured information. Databases of medical claims information, laboratory results, electronic medical records, electronic personal health records, and prescription history will play an integral role in providing a complete picture of the whole patient. Health information exchanges, coupled with these data pools, make the health data available in real time to all of a patient's care providers. Health information exchanges should span primary care physician practices, specialty health locations, hospital systems, long-term care facilities, and other relevant care settings. This type of integrated data gives stakeholders a full view of patients' health status. Stakeholders can then effectively use these robust data resources to calculate the trajectory of a patient's health needs through predictive modeling. Stakeholders would find themselves well positioned to accurately identify health risks and appropriately tailor health care interventions.
Centralized, comprehensive, interconnected data also support tools to create a fluid communication system for regular and continuous patient interaction. This type of communication is essential to patient education and engagement. It also encourages patients to actively participate in health care self-management. Regular interaction serves as a preventive mechanism to support patients in care management programs and alert patients about serious changes in their health conditions. These data resources make open dialogue and shared decision making possible for patients and care providers, which harmonizes care among the plethora of health care providers, plans, and programs.
In addition to energizing and streamlining the functional capacity of care management programs for dual and pre-dual eligibles, these data resources create opportunities for continuous program evaluation and improvement. As a constantly updating source of information, accessible, comprehensive, interconnected data offer a way to evaluate program outcomes and assess care management programs for dual eligibles. This feeds into a loop for continuous innovation and program improvement. Building these databases and health information exchange networks collaboratively permits health care industry stakeholders to leverage a uniform and system-wide infrastructure, collectively achieve meaningful use milestones, and improve the flow of information across payers. States also must have access to important Medicare data sets through a single, secure, no-cost data hub with minimum required administrative paperwork.
Component 2: Health Risk Assessments and Stratification
The Problem
It is difficult to identify health care risks and needs among dual eligibles because of this population's propensity to develop multiple and long-term chronic conditions. A 2010 Kaiser Family Foundation report found that at least 60% of dual eligibles have multiple chronic physical conditions; of those, 40% have mental illness. “Significant comorbidities among dual eligibles make service use high and care coordination across Medicare and Medicaid particularly challenging,” the report concluded. An additional complication is the tendency of patients in this population to shift into and out of dual eligibility status. The PHM industry's experience with risk assessment and stratification tailors health interventions to prevent patients from moving into higher-risk categories. Similar risk assessment for pre-dual eligibles could mitigate their rate of conversion to dual eligible status.
The Solution
Health risk assessment (HRA) and stratification are critical to dual eligible and pre-dual eligible care coordination. These tools offer accurate, patient-specific risk determinations to employ effective, clinically appropriate, value-based interventions. A health professional should conduct appropriately tailored individual HRAs with patients to determine where they fall on the continuum of care and how to plot a care management course that improves health outcomes and reduces health care costs. Long-term health costs often can be avoided or dramatically delayed through early identification of risk factors for chronic conditions or functional declines and the application of community-based services.
Policies to promote broader use of HRAs and risk stratification in dual eligible care coordination should: • Allow for design and administrative flexibility to accommodate dual eligible population characteristics. • Link HRA administration with health information technology to provide real-time, readily accessible, and easily understandable results to health care provider teams. • Create Medicare and Medicaid beneficiary incentives for HRA participation and provider incentives for administering HRAs. • Promote use of accredited or certified HRAs by nationally recognized, independent quality organizations, such as the National Committee for Quality Assurance and URAC. • Require HRA administration at the time of dual eligible enrollment to establish a baseline health assessment and conduct follow-up assessments every 6 months.
Component 3: Population-Specific and Personalized Care Planning
The Problem
Dual eligibles and pre-dual eligibles require individualized care plans that weigh health risks and assess all health needs to ensure that the services provided are tailored to improve health outcomes and achieve cost savings. Without this level of personalization, care management programs might apply ineffective resources and strategies that result in higher costs to all health care stakeholders. Further, personalized care plans require the expertise of a multidisciplinary care team to address specific health needs.
The Solution
Care plan development is critical to ensure that appropriate, value-driven services are delivered through a coordinated team of health professionals with expertise in multiple health areas. Care coordination programs reinforce engagement with dual eligible patients through simple, patient-friendly, and personal messages. This avoids fragmented communication with multiple providers. Care managers conveniently position dual eligible patients and care providers to coordinate health interventions in a patient-centered, collaborative, streamlined fashion. Care managers also increase the ability of multidisciplinary care teams and dual eligible patients to remain in routine and ongoing communication. This open dialogue continues educating patients, alerts patients to significant changes in health status, and maintains strong patient participation in their own care management.
Component 4: Care Coordination and Transitions of Care
The Problem
Coordination among all stakeholders involved in care delivery is difficult, given the many parties involved and the unique challenges of dual eligible populations. Care coordination among multiple providers and services includes pharmacy, behavioral health, and long-term care among others. Additionally, achieving seamless transitions in care among various health care settings requires synchronized approaches with all of these stakeholders. Lack of care coordination and fluid care transitions often increase health costs in Medicare and Medicaid related to duplicative screenings, clinically inappropriate treatments, administrative burdens, and reduced quality in delivery systems.
The Solution
Greater coordination across health care settings and services provides a foundation for smooth transitions in care. This would simplify government requirements and screening procedures, as well as incorporate coordinated services into health programs for dual eligibles. Coordinated services include a combination of medication therapy management and adherence, wellness programs, health coaching, mental health support, rehabilitation programs, end-of-life care, and counseling. Building upon previous CCA core components, care coordination programs use comprehensive data, risk assessment, care managers, and multidisciplinary teams of health professionals to strategically apply health services that will improve health outcomes while reducing costs. Community-based programs offer the best opportunities for population-specific and personalized interventions, especially for dual eligible populations.
Component 5: Education, Training, and Incentives for Patients and Providers
The Problem
Providers and states have little experience with integrated, coordinated, team-based health care strategies for dual eligible populations. Many health professionals also lack a fluid understanding of how to seamlessly integrate electronic health records into a physician's workflow. This limited experience, combined with misaligned incentives for providers and patients, translates to low patient enrollment in coordinated care management programs and poor provider participation.
The Solution
Education and incentives can play important roles in driving patient and provider participation in coordinated care management programs for dual eligibles. These tools also can help advance broader care coordination, quality improvement, and value-based goals of states and other stakeholders. Using a capitated joint reimbursement from Medicare and Medicaid, in addition to shared savings or bonus payments, offers one possible solution to create incentives for health professionals and patients.
Additionally, education programs must ensure that participating providers and other health professionals receive continuous training about strategies and tools deployed by new integrated care models. Technology innovations can facilitate training, support education goals, and disseminate best practices. Similar outreach should be provided for patients to enhance their understanding of available health services and coordination of their Medicare and Medicaid benefits.
Component 6: Program Evaluation and Outcomes Toward Improvements
The Problem
Assessing program outcomes, identifying problems, and finding gaps in care are critical to achieve success in care coordination. There is a pressing need in the health care industry to clearly understand which care strategies work best for dual eligible populations. This pressure stems from the health care system's drive toward value-based purchasing, pay-for-performance, comparative effectiveness research, and incentives structured around clinical and financial outcomes. However, the complicated health needs of dual eligible populations and the fractured state and federal health systems present particular challenges to outcomes measurement.
The complexity of dual eligible care poses special difficulties for broad program evaluation. Assessments need to consider many factors such as: care management programs for multiple chronic conditions; frail elderly services; behavioral health care; home and community-based services; nursing facility transitions; and hospital readmissions. Cultural and language differences also enter the mix.
The lack of data sharing between Medicare and Medicaid programs is particularly daunting for outcomes measurement. State program administrators often face significant data shortfalls when developing and assessing integrated care coordination programs for dual eligibles, working with limited Medicare crossover claims figures extracted from Medicaid records. Also, duals eligibles often have complex and multiple chronic conditions that necessitate receiving care and education from a variety of health care professionals. To offer patient-centered, coordinated care, these health professionals need access to the full breadth and depth of Medicare and Medicaid health information for their patients. Only this level of real-time information access will ensure true coordination of all health care services and ongoing program improvement.
The Solution
As coordinated care models for dual eligibles arise, the models must establish broad goals on program outcomes, as well as specific measures correlated to each outcomes goal. This system effectively tracks progress to improve program performance. It will be particularly important to choose appropriate evaluative measures and methodologies, given the complex health needs of dual eligible patients. Programs also must consider cultural and language barriers in the administration of patient surveys and other data collection tools.
Improved Medicare-Medicaid data sharing between state and federal systems will be paramount to assessment efforts. Data sharing systems also should align with program evaluation measures on quality and outcomes. CMS and states should work to ease access to the Medicaid and Medicare data that integrated programs need to effectively manage care and accurately measure performance. Further, state and federal agency administrators and industry stakeholders should collaborate on tailored and appropriate measurement systems for programs that serve dual eligibles.
Additional Health Policy Considerations in Models of Care for Dual Eligibles
In the months ahead, CCA will build and improve on its health policy work in the dual eligibles arena. A natural next step would be looking into the design elements of the financial models needed to sustain care coordination programs for dual eligibles. CCA looks forward to exploring care coordination programs for dual eligibles from the health care provider perspective and how providers can easily employ these core components in daily practice. CCA also plans to address the patient perspective in this population by considering how to help dual eligibles navigate these care coordination programs. Please consult the Care Continuum Alliance website,