
Abstract
The objective was to understand how Federally Qualified Health Centers (FQHCs) and local health departments (LHDs) address their shared mission of improving population health by determining the scope of primary care and public health activities each provides in their community. A brief mail survey was designed and fielded among executive directors at all 14 FQHCs in Iowa, and 13 LHDs in Iowa representing counties with and without an FQHC. This survey contained a mixture of questions adapted from previously validated primary care and public health survey instruments. Using survey responses, each FQHC and LHD was given 2 scores (each ranging from 0–100) measuring the extent of their primary care and public health activities, respectively. The overall response rate was 85.2%; the response rate was 78.6% within FQHCs and 91.7% within LHDs. Overall, FQHCs had higher scores (73.8%) compared to LHDs (27.3%) on total primary care services, while both LHDs (79.3%) and FQHCs (70.9%) performed particularly well on public health services. FQHCs and LHDs in Iowa address a variety of public health and primary care issues, including but not limited to screening for chronic diseases, nutrition counseling, immunizations, and behavioral health. However, FQHCs provide a higher amount of primary care services and nearly as many public health services when compared to LHDs. In a value-based health care delivery system, integrating to improve population health is a wise strategy to maximize efficiency, but this will require maximizing coordination and minimizing duplication of services across different types of safety net providers. (Population Health Management 2015;18:137–145)
Introduction
T
Today, integration is proposed as a strategy that will lead to improved health outcomes, lower costs, and reduced health disparities over time. 7, 11 –14 Integration has the potential to reduce duplication of services, capitalize on the sharing of existing resources, and facilitate data sharing. Numerous small-scale efforts to integrate primary care and public health have been attempted but these undertakings have either failed to become sustainable 15 –17 or have yet to be widely implemented. 18–19
The resource constraints that make integration particularly attractive are especially prevalent among health care safety net providers, including Federally Qualified Health Centers (FQHCs) and local health departments (LHDs). However, like the fields of primary care and public health more generally, FQHCs and LHDs have historically been concerned about competing against each other by providing overlapping services and applying for funding support from many of the same sources. 14
FQHCs are federally funded facilities legally mandated to provide primary care to all without regard for their ability to pay, using an income-sensitive sliding fee scale. Consequently, FQHCs serve a low-income, often uninsured population with higher rates of chronic disease than the general population. 13 FQHCs also are required to provide preventive services such as immunizations, nutritional counseling, hearing and vision screening, blood pressure screening, and health education. 20 Some of these activities overlap with services provided by LHDs in the community. However, because of time constraints in primary care settings, physicians are more likely to focus on acute care delivery than preventive care and chronic disease management. 4
LHDs also are an integral part of the health care safety net in most parts of the country. Typically financed by state and local governments, LHDs are frequently organized at the county level, where they are tasked with performing a wide array of public health functions including but not limited to disease surveillance and prevention, regulation and oversight of environmental health risks, and direct care delivery. Because the assurance of available care is a core public health function, LHDs are sometimes primary care providers of last resort for the uninsured and indigent. LHDs in Iowa offer immunization clinics, screening and diagnostic services, health education, and skilled nursing visits in the client's home in addition to the other essential public health services LHDs are required to provide their communities. 21
The Affordable Care Act (ACA) recognizes the importance of preventive public health and primary care services in improving population health. 22 With the establishment of the Prevention and Public Health Fund, the ACA provides funding for evidence-based clinical prevention and public health services aimed at improving health outcomes and health care quality. 23 FQHCs and LHDs could benefit from the increased funding opportunities provided under the ACA as they both provide public health and primary care services. Encouraging the collaboration of health care delivery between these providers could result in a more effective expansion of health programs to promote population health.
Although both FQHCs and LHDs clearly have an interest in improving population health, and have the potential to be engaged in both primary care and public health activities, little is known about their respective functions in practice. Thus, the overall objective of this study is to understand how FQHCs and LHDs address their shared mission of improving population health by surveying executive directors of both FQHCs and LHDs in Iowa to determine the scope of primary care and public health activities each provides in their community. The research team terms this range of services “organizational scope of practice” and considers delineating it to be a fundamental starting point for any successful and sustainable effort to integrate primary care and public health.
Methods
To determine the scope of primary care and public health activities provided by FQHCs and LHDs in Iowa, the research team designed and fielded a brief mail survey among executive directors at all 14 FQHCs in Iowa, and 13 LHDs in Iowa representing counties with and without an FQHC. However, the team did not indicate that the executive directors were required to complete the surveys themselves. Therefore, it is possible that the executive directors delegated the task of completing the survey to staff members who had better knowledge of the specific services provided by the facilities.
This survey contained a mixture of questions adapted from previously validated instruments including the National Association of Counties and National Association of Community Health Centers Community and Public Health Center Questionnaire, 24 the Modified Primary Care Assessment Tool, 14 and the Public Health Involvement Questionnaire. 14 The questions in these instruments were designed to identify a core set of primary care and public health activities at the organizational level. To increase response rates, potential survey respondents were contacted by telephone prior to receiving the survey, and received a small monetary incentive ($25) along with the survey for their participation. Nonresponders received a series of reminder phone calls beginning 3 weeks after the initial survey invitation was sent and were sent another copy of the survey if necessary. After allowing ample time for individuals to respond, the survey was closed and responses were analyzed.
The survey instrument contained a total of 50 questions. Of these, 25 asked about primary care activities, and 25 asked about public health activities. Respondents were asked if their clinic provided each of the listed services, and response categories included definitely, probably, probably not, definitely not, and don't know. Point values were assigned to each response category as follows: definitely (4 points), probably (3 points), don't know (2 points), probably not (1 point), and definitely not (0 points). These point values were then summed separately for primary care and public health activities. In this way, each FQHC and LHD received 2 scores describing the scope of its primary care and public health activities on a scale from 0 (definitely do not provide any services) to 100 (definitely provide all services). The research team summarized these data in the aggregate and present descriptive statistics on the state of primary care and public health at FQHCs and LHDs in Iowa.
Overall, FQHCs responded don't know on 6 items on the primary care services scale and 4 items on the public health services scale. LHDs, on the other hand, responded don't know on 4 items, all of which were on the primary care services scale. It is important to note that don't know responses were scored as 2 points. This was done to reduce nonresponse bias, assuming that, on average, not knowing was equally likely to reflect provision or no provision of a given service. To examine this assumption, a sensitivity analysis was conducted using 2 alternative scoring methods, which only modestly changed the numerical results without changing the basic findings. In the first alternative, the weights for don't know and probably not responses were switched, so that probably not=2 points and don't know=1 point. Using this scoring system, FQHCs scored 75.9% and LHDs scored 28.8% for primary care services and 73.0% and 81.3% for public health services, respectively. In the second alternative, points were reassigned as follows: definitely (4 points), probably (2 points) and probably not, don't know, and definitely not (0 points) each. Using this scoring system, FQHCS scored 67.0% and LHDs 23.0% on primary care services and 61.0% and 71.0% for public health services, respectively.
Results
A total of 23 of 27 surveys were received for an overall response rate of 85.2%. The response rate within FQHCs was 78.6% and the response rate within LHDs was 91.7%. Locations of respondents are shown in Figure 1. Note that one of the responding LHDs is located in Illinois but, given its location on the border with Iowa, its service area spans into Iowa, and thus it is included here as part of Des Moines County. Overall, we find that FQHCs had higher scores (73.8%) compared to LHDs (27.3%) on total primary care services, while both LHDs (79.3%) and FQHCs (70.9%) performed particularly well on public health services.
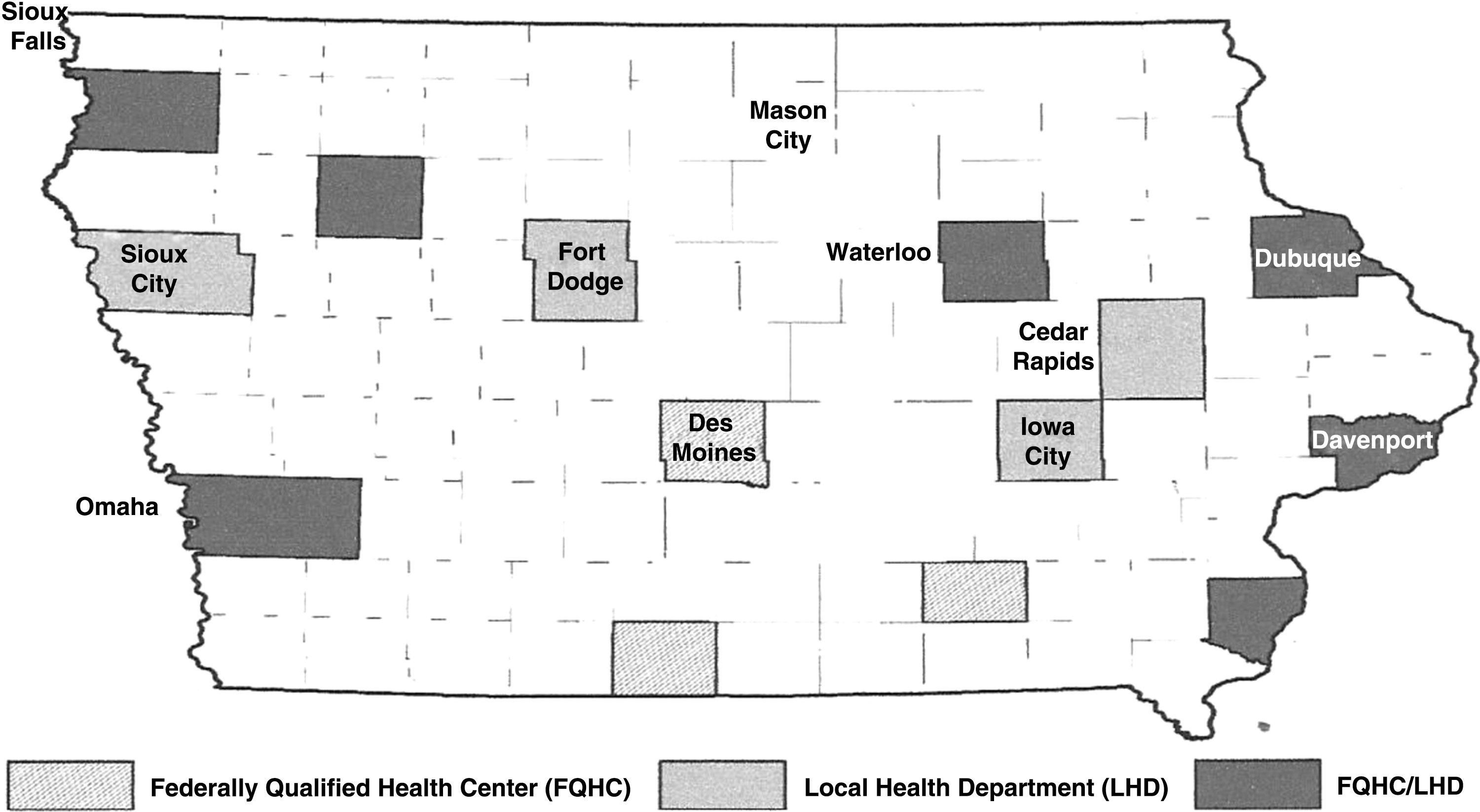
Location of respondents.
Primary Care Services
Figure 2 compares the proportion of FQHCs and LHDs that achieved the maximum score of 4 (ie, definitely provide) for each primary care service listed on the survey. More than 90% of FQHC respondents in Iowa indicated that they provide preventive primary care services such as smoking counseling, pap smears, and vision screening to their patients. At least half of FQHCs reported providing services tailored to meet the needs of their aged patients. Concerning mental health and substances abuse, the proportion of FQHCs that reported providing counseling and treatment to their patients ranged from 35% to 55%. Although more than half of FQHCs reported providing eligibility screening for social services, none of the FQHCs reported definitely providing Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) to their low-income mothers and children younger than 5 years of age.
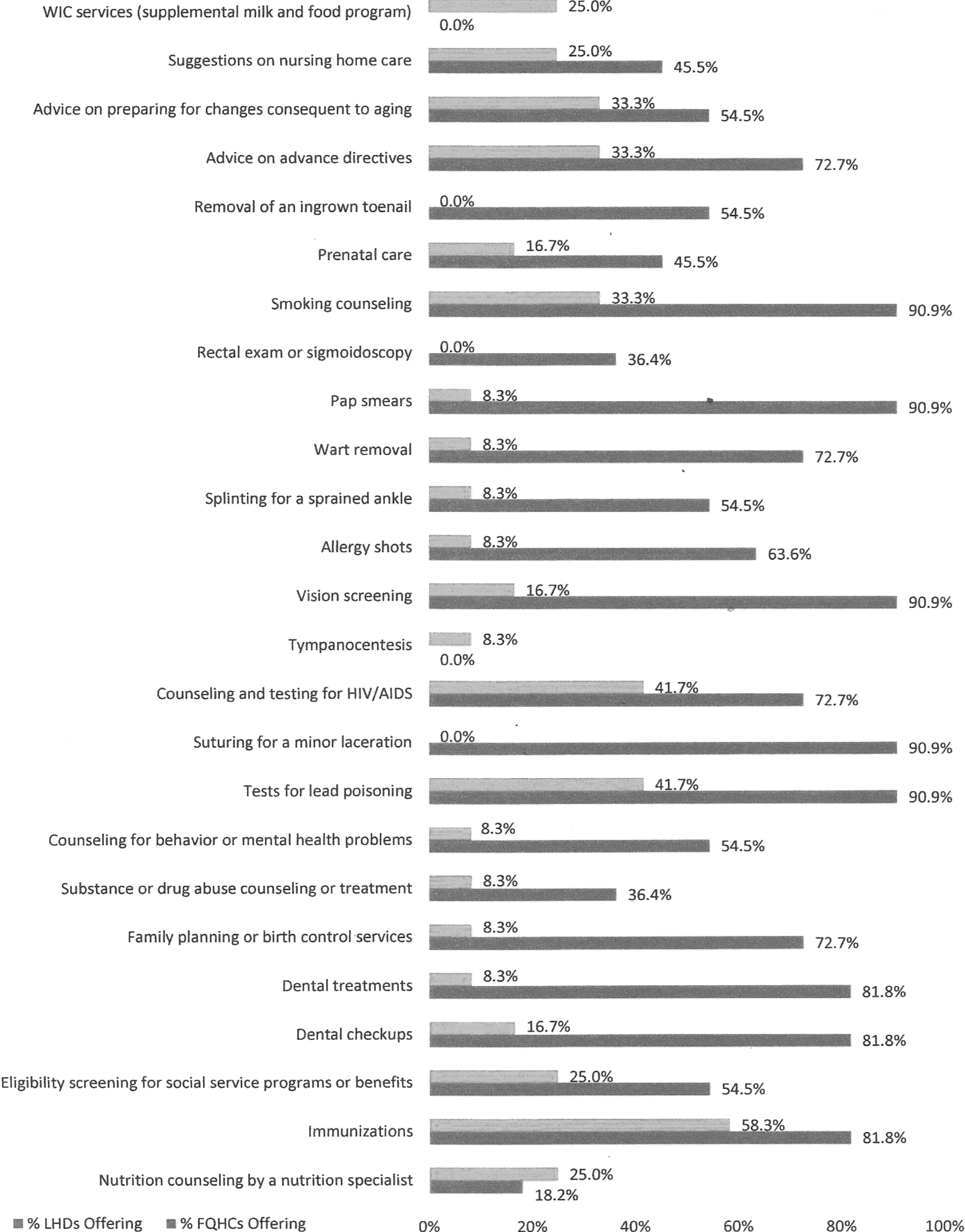
Proportion of respondents providing a given primary care service, by provider type. FQHC, Federally Qualified Health Center; LHD, local health department; WIC, Special Supplemental Nutrition Program for Women, Infants and Children.
By contrast, the total average score for primary care services by LHDs was less than 30%, as mentioned earlier. The results in Figure 2 show that more than 40% of the LHDs accessed reported providing primary care services like immunizations, HIV counseling and testing, and lead testing. Also, at least one quarter of LHDs have eligibility screening services for social service benefits for patients and WIC for low-income mothers and children younger than 5 years of age while about 25% to 33% of LHDs give their elderly patients advice on aging and suggestions for nursing homes. Interestingly, fewer than 1 in 10 LHDs surveyed reported providing mental health and substances abuse services to their patients.
Public Health Services
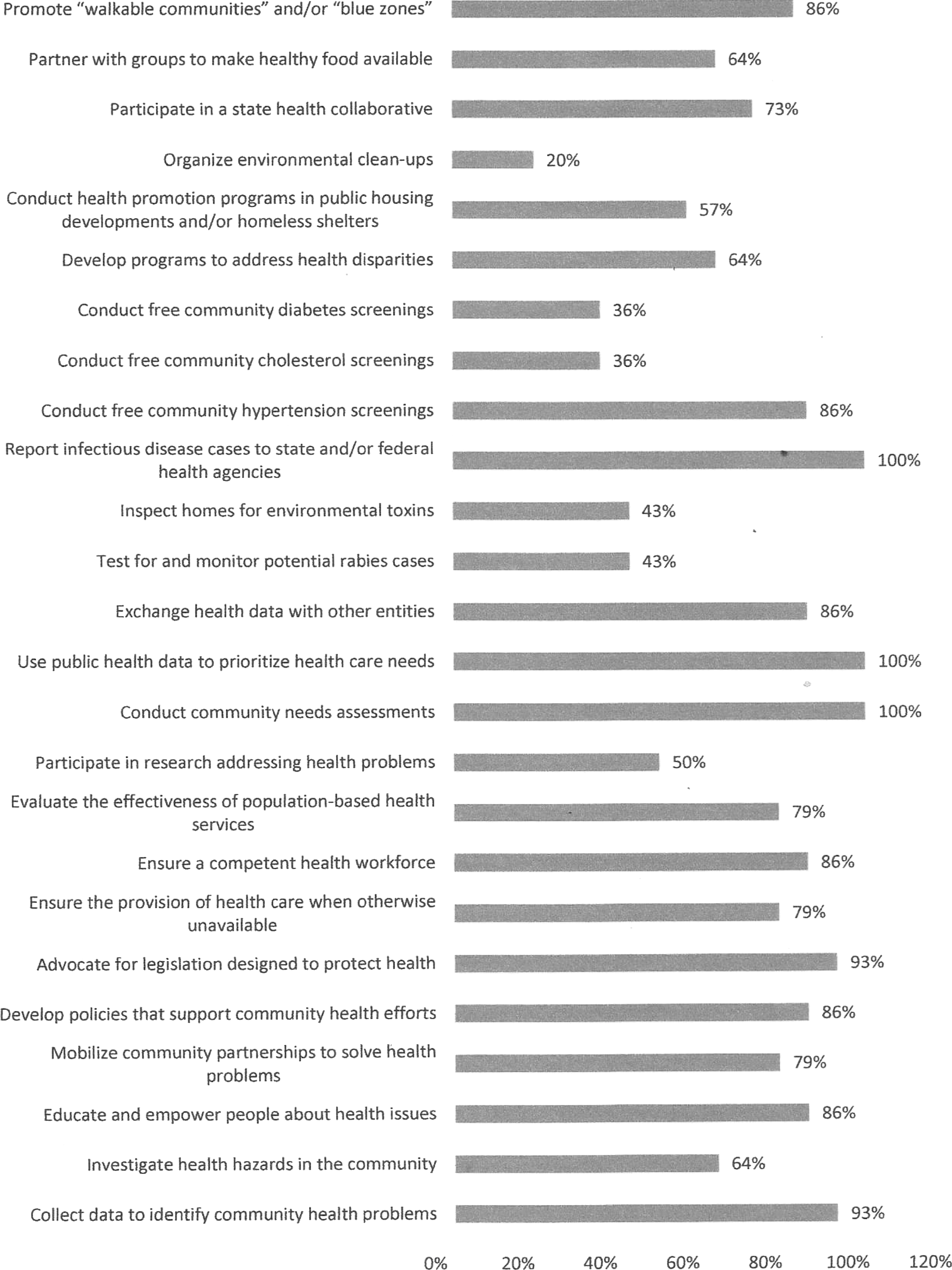
Figure 3 compares the proportion of FQHCs and LHDs that reported definitely providing each of the 25 public health services listed. A majority of the FQHCs in the survey reported that they undertake needs assessment in their communities and inform, educate, and empower their patients on health issues (>80%). A majority of FQHCs also reported collecting and sharing health data with other providers and using data to prioritize the health care needs of the community they serve (70%–80%). More than 80% of the FQHCs reported developing programs to reduce health disparities among their patients. For management of chronic diseases, at least two thirds of FQHCs reported that they conduct hypertension screenings but less than one third provide screenings for diabetes and cholesterol.
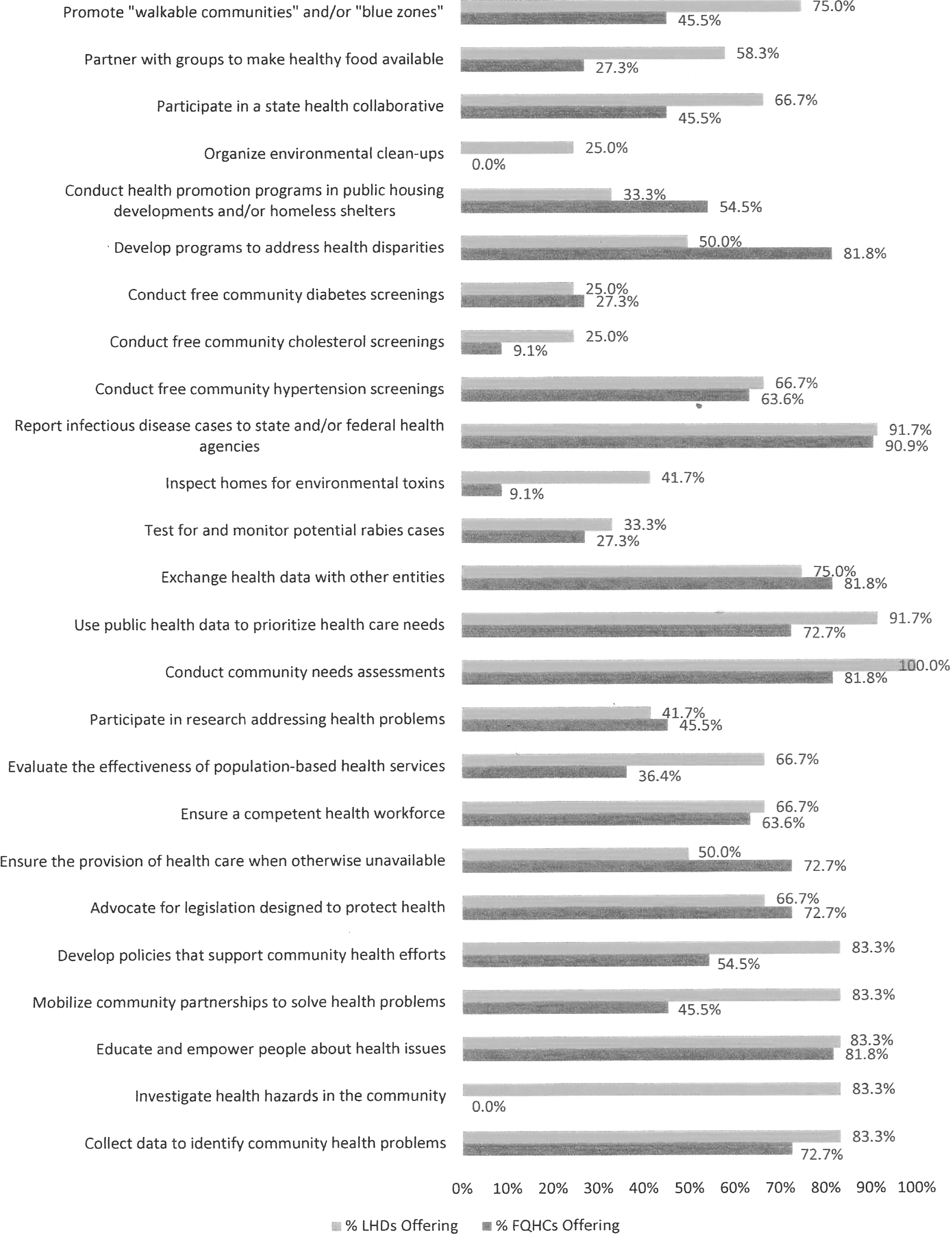
Proportion of respondents providing a given public health service, by provider type. FQHC, Federally Qualified Health Center; LHD, local health department.
Similarly, LHDs achieved good total average scores on public health services. All the LHDs in the survey conduct community needs assessment. A majority of them reported that they collect data to identify community health problems, use the data to prioritize health care needs and inform, empower, educate, and mobilize the community to solve health problems (>80%). At least three quarters of all LHDs share health data they collect with other entities, and nearly 92% of the LHDs report cases of infectious diseases to the appropriate agencies. About two thirds of LHDs reported providing hypertension screenings, and only about a quarter reported providing diabetes and cholesterol screenings.
To explore the potential effect of FQHC availability on LHD service provision, the research team compared the primary care and public health services provided by LHDs in counties with and without FQHCs. LHDs in counties without an FQHC present provide, on average, 26% of the primary care services asked about, compared to an average score of 28% among LHDs in counties with an FQHC present. Similarly, LHDs in counties without an FQHC present provide, on average, 75% of the public health services asked about, compared to an average score of 81% among LHDs in counties with an FQHC present. Thus, there are no significant differences overall in the services provided by LHDs in counties with and without FQHCs. In fact, if anything, LHDs in counties with an FQHC actually report providing more public health and primary care services.
The research team also combined the responses of FQHCs and LHDs for both primary care and public health services to identify any overall gaps in services provided at the county level. This study found that, even when taking FQHC and LHD services as a whole, many counties do not provide the full array of primary care and public health services about which the survey inquired. In fact, a majority of counties in the study sample do not provide 36% of the primary care services about which the survey inquired (see Fig. 4). Similarly, a majority of counties in the study sample do not provide 20% of the public health services about which the survey inquired (see Fig. 5). Moreover, none of the counties in the sample provide all 25 of the primary care services, and only 3 of the 25 public health services (ie, infectious disease reporting, using public health data to prioritize health care needs, conducting community needs assessments) are provided by all of the counties in the sample.
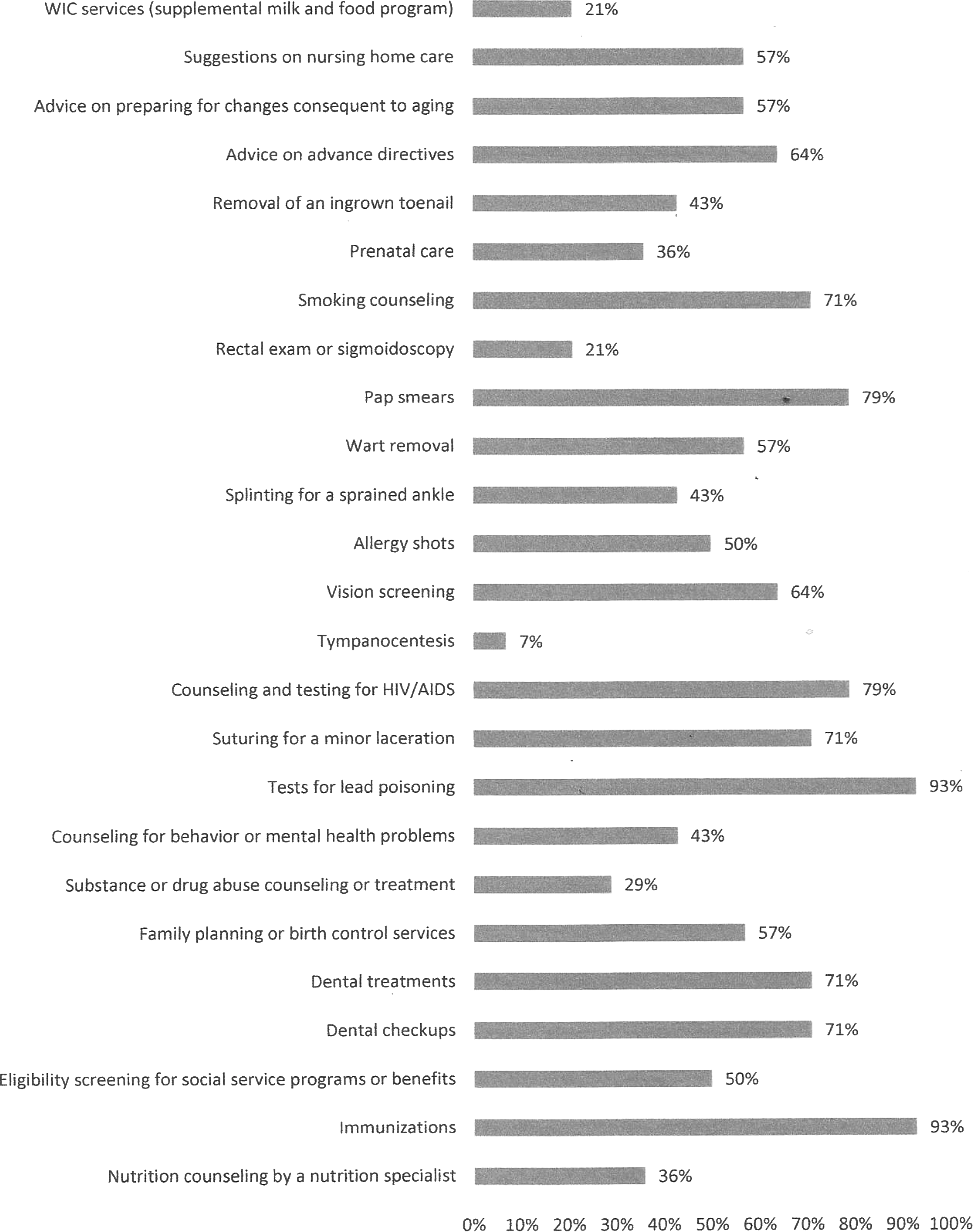
Percentage of counties where a given primary care service is available from either a FQHC, an LHD, or both. FQHC, Federally Qualified Health Center; LHD, local health department; WIC, Special Supplemental Nutrition Program for Women, Infants and Children.
Percentage of counties where a given public health service is available from either a FQHC, an LHD, or both. FQHC, Federally Qualified Health Center; LHD, local health department.
Discussion
Both FQHCs and LHDs have a common interest in improving population health and have the potential to be engaged in both primary care and public health activities. Primary care and public health have a common focus of improving population health. 17 However, little is known about their respective functions in practice. This study provides an overview of the organizational scope of practice of FQHCs and LHDs in one Midwestern state.
Although the cross-sectional study design prohibits the research team from commenting on trends in service provision over time or making causal inferences about the effect of policy implementation, the team is able to provide a snapshot of the organizational scope of practice of both FQHCs and LHDs. This study finds that FQHCs provide a high number of both public health services and primary care services. That is, not only do they provide significantly more primary care services than LHDs (as expected), but they also report providing nearly as many public health services as LHDs, which was unexpected. However, these findings are consistent with a previous study on FQHCs. 14
As expected, this study finds that LHDs in Iowa provide a significant amount of public health services. However, the study also finds that, despite the assurance of access to care being a core public health function, LHDs in Iowa are providing relatively few primary care services. 21 The research team is unable to conclude from this study whether the provision of primary care services by LHDs varies with the availability of other sources of primary care in the community.
The ACA places an emphasis on primary care and preventive services to improve the health of underserved and vulnerable communities, and to eliminate health disparities. 22 The findings of this study indicate that both FQHCs and LHDs in Iowa address a variety of public health and primary care issues, including but not limited to screening for chronic diseases, nutrition counseling, immunizations, and behavioral health. Integration of health care delivery among these providers, with a focus on improved care coordination and reduction in the duplication of services, would lead to more efficient use of scarce resources and promote overall efficiency and effectiveness. 17 Integration of care between these providers also may reduce the competition between them for scarce funding resources. LHDs and FQHCs are eligible for funding opportunities under the ACA by virtue of the services they provide and the populations they serve. These opportunities include community transformation grants offered for community health teams, 25 primary care extension programs, 26 and community-based prevention and wellness programs. 27–28 Integration of health care delivery among these providers would make them eligible to collaborate on, rather than compete for, these grants and could result in expansion of programs that promote population health.
Another means of strengthening public health and primary care collaboration is by sharing data between facilities. 13 This study shows that both LHDs and FQHCs collect data for community surveillance and disease burden and share data with other health providers. The data provide information needed to forge evidence-based policies that effectively address the needs of the community and reduce or eliminate health disparities. Promoting data sharing and coordination between both provider types could reduce duplication of data collection efforts.
FQHCs and LHDs in Iowa also provide services for chronic disease management including smoking counseling, nutrition counseling, and free community screening for diabetes, hypertension, and cholesterol. Chronic disease directly affects roughly half of the US population. 12 The provision of these services by both FQHCs and LHDs may lead to an increase in access to care in the community. Collaboration between providers to integrate service delivery for the management of chronic diseases and to reduce duplication of services would ensure seamless delivery of services in an efficient and cost-effective manner. However, a drawback in the effort to reduce duplication of services is the possibility of producing an unintended effect that would further silo primary care and public health. 10
The findings of this study reveal important gaps in care for WIC services (supplemental milk and food program), prenatal care, nutritional counseling, and screening for chronic diseases. The importance of prenatal care and maternal nutrition programs have been documented as important means of reducing the risk of prematurity, stillbirth, early and late neonatal death, and infant mortality. 29–30 Both FQHCs and LHDs serve as “safety net” providers for low-income, often uninsured populations who bear a disproportionate burden of chronic diseases and neonatal and infant mortality compared to the general population. 13,31 Therefore, these gaps in care may have detrimental effects on this population.
One of the limitations of this study is that the research team compared the primary care and public health services provided by LHDs and FQHCs in Iowa, a mostly rural Midwest state. 32 Consequently, the results may not be easily generalizable to more urban states. LHDs serving urban populations more frequently provide a greater array of services than those serving rural populations. 33 However, given the well-documented lack of data on the type and volume of specific services provided by LHDs, 34 this study provides valuable information about service delivery in a Midwest state that is required for evidence-based decision making. There is room for further studies on the pattern of services provided by LHDs and FQHCs in more urban states. Also, a longitudinal study design would be beneficial in commenting on trends in service provision over time and the effect of policy implementation on service provision.
Another potential limitation of this study is that the survey was sent to the executive directors of FQHCs and LHDs, who may not be the best source of information on the details of the types of services provided because executive directors usually have major administrative functions. However, it is possible that these directors delegated the task of completing the survey to staff members who had better information on the details of the primary care services provided by the facilities, as the directors of these facilities were not required to complete the surveys personally.
In summary, the ACA focuses on increasing preventive health services, improving the efficiency of health care delivery, and reducing health care costs. 35 Integration of primary health care and public health service delivery plays an important role in achieving these goals. Greater collaboration and coordination of FQHCs and LHDs will lead to improved care coordination for patients and a reduction in the duplication of services. The gaps in care as seen in this study also could be addressed by delegating certain services to one or the other type of facility depending on the type of providers available at each. For example, services that require a primary care physician could be delegated to FQHCs. This study provides an overview of the organizational scope of practice of FQHCs and LHDs in Iowa and provides a starting point for the consideration of possible ways to integrate primary care and public health in a health care delivery system that is shifting to an increased emphasis on value and population health outcomes.
Footnotes
Author Disclosure Statement
Dr. Wright, Ms. Ugwi, and Mr Nice declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. This study was supported in part by a University of Iowa College of Public Health New Investigator Award.