
Abstract
The follow-up rate among children with vision problems in the authors' outreach programs has been <5%. The authors therefore developed a social worker (SW) intervention, the Children's Eye Care Adherence Program (CECAP), for Philadelphia school children. The objective of this study was to measure CECAP's effectiveness and cost, as well as to identify barriers to care through a conceptual framework and geomapping software. A SW reviewed records to identify children needing follow-up and phoned families to identify and resolve barriers to eye care and scheduled appointments. Effectiveness was defined as the percent completing ≥1 follow-up visit within the physician-recommended time frame. Cost was measured for SW time (SW wage rates+benefits) and additional materials (forms, postage, phone charges). Barriers were organized into a conceptual framework depicting predisposing factors, system factors, and financial factors. Geomapping software was used to illustrate follow-up rates. In all, 120 patients required additional pediatric ophthalmic care; 71 patients were contacted and returned for care (59.2%); 49 patients were contacted but did not return (40.8%). SW time was 3hrs/patient for those who returned and 2hrs/patient for those who did not return. Based on the CECAP program total cost ($14,249) and the reimbursement payment ($6265.66), the net cost of the CECAP program was $7983.59. Predisposing factors were the primary barrier theme for patients who did not follow up. CECAP significantly improved adherence to eye care but comes at an additional cost. Future efforts should focus on reducing operational efficiencies and targeting CECAP based on predictors of follow-up. (Population Health Management 2015;18:223–231)
Introduction
M
The Pediatric Ophthalmology and Ocular Genetics Service at Wills Eye Hospital participates in 2 clinical outreach programs to deliver care to high-risk Philadelphia children identified as having eye problems requiring the care of a pediatric ophthalmologist. The Eagles Eye Mobile (EEM) visits schools in low-income neighborhoods during the academic year and provides optometric examinations to children who have failed their state-mandated school vision screenings. EEM examines approximately 3200 children each school year and refers children who need additional vision care to a special Eagles clinic conducted at Wills Eye Hospital Pediatric Ophthalmology service almost every other week during the academic year. The number of children who arrive at each clinic varies.
Give Kids Sight Day (GKSD) is an annual 1-day event available for uninsured and insured children in Philadelphia and surrounding areas who are younger than 19 years of age and need vision screenings. Typically, 1200 children attend this popular community event and receive full comprehensive ophthalmologic exams. If vision can be corrected with eyeglasses, both EEM and GKSD programs then make provisions to supply the children with 2 pairs of eyeglasses at no cost to the family.
Although EEM and GKSD have proven to be very successful outreach programs in providing ophthalmic care to children in need, less than 5% of patients identified as requiring ongoing follow-up care had returned for their prescribed visits. Prior to the initiation of the project discussed in this paper, no formal efforts were made to contact the families of children who were evaluated by these programs and who were determined to need follow-up care. Thus, the parents or guardians had been primarily responsible for scheduling subsequent appointments for their children.
In response to this poor follow-up rate, Wills Eye Hospital and Thomas Jefferson University developed the Children's Eye Care Adherence Program (CECAP), which utilizes a licensed social worker to identify and address barriers to follow-up care. Components of CECAP include: 1. Reviewing records of children identified as needing follow-up vision care 2. Scheduling subsequent appointments with Wills Eye pediatric ophthalmologists 3. Assessing and attempting to resolve or lessen psychosocial barriers to follow-up care 4. Tracking patients' show and no-show rates to ensure that return visits are maintained 5. Providing continuous intervention and case management on an ongoing basis
The primary objective of this project was to measure the effectiveness of CECAP, defined as the number of children who completed at least 1 of the recommended follow-up vision exams, with the goal of boosting follow-up rates from a pre-study rate of less than 5% to a higher rate of 25%. The secondary objective was to measure the cost of CECAP, total and per child, by conducting an economic evaluation of direct and indirect expenditures for effective delivery of services. In addition, an exploratory analysis was conducted using geomapping software to identify characteristics of neighborhoods of patients who returned for appointments (RFA) vs. those patients who did not return for appointments (NR).
Methods
Study population
Eligible participants for this study were children ≤18 years of age who were identified to have an eye concern after an ophthalmology examination at GKSD 2012. This included any child whose vision was not correctable to 20/20 with glasses or who was suspected to have an ocular disorder requiring follow-up, such as amblyopia, strabismus or structural defects of the eye. Children who were examined at the Wills Eye Eagles Clinics during the 2011–2012 academic year and had eye abnormalities that required a return visit within 1 year also were eligible.
Study procedures
Study procedures are summarized in Figure 1. The social worker identified and reviewed all charts and medical records for eligible patients and contacted parents and guardians of patients via telephone to schedule follow-up appointments within a 6-month period. The social worker confirmed demographic information, which included the following: patient's name, date of birth, date of medical service, school, parent/guardian contact information, diagnosis, and type of insurance coverage. The social worker interview was unstructured as historical experience has shown that families are sometimes reluctant to divulge personal or private information. Utilizing a more casual approach via phone conversation made it easier for the social worker to obtain optimal information in a brief time period, while being sensitive to this issue. When GKSD patients were identified as needing follow-up care, a process of collecting up to 5 telephone numbers was used as this proved helpful in contacting family members.
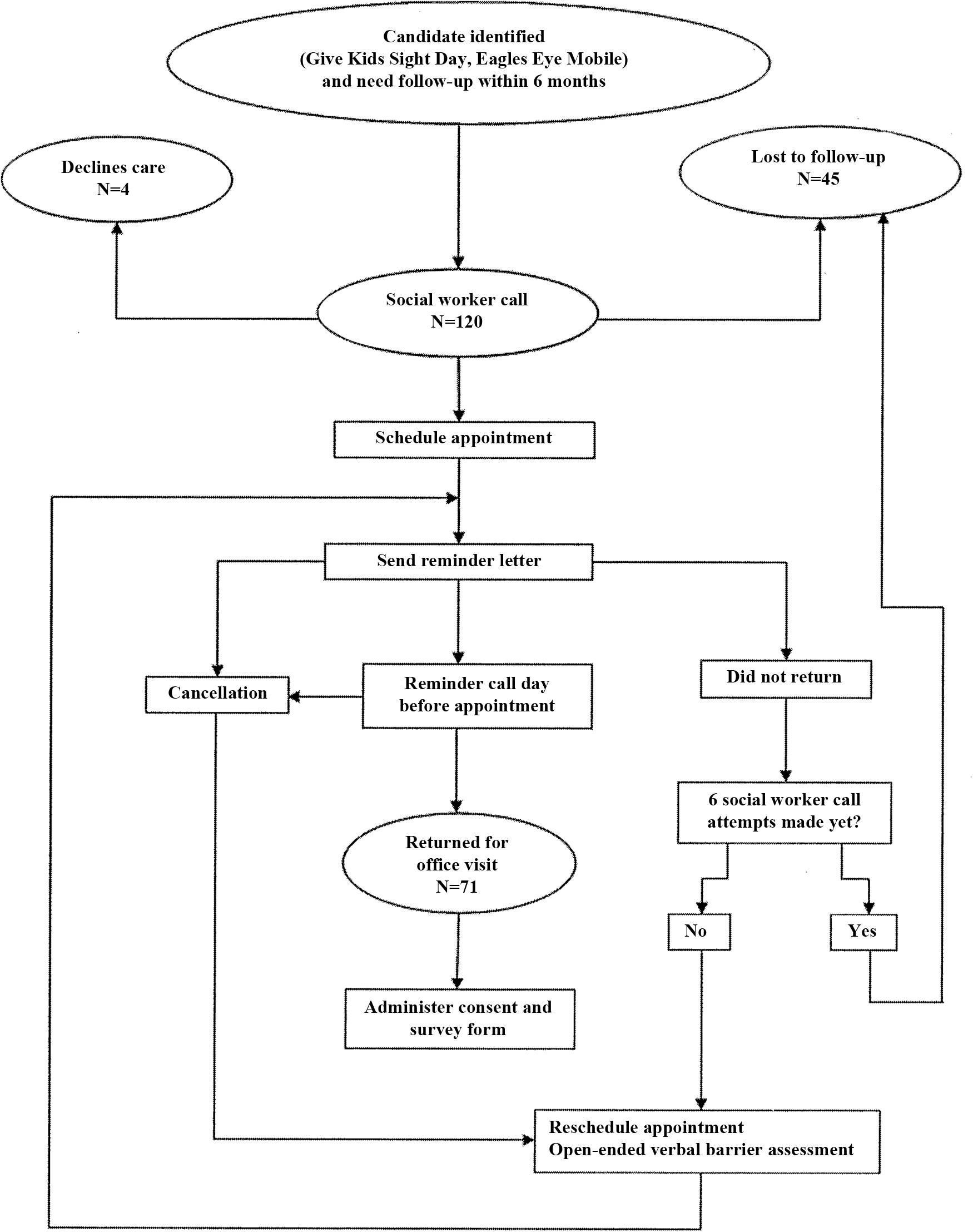
Overview of study procedures.
The social worker relied on consent and demographic information from the Philadelphia School District and EEM for children examined in the Wills Eye Eagles clinics. Often, only 1 phone number was listed on parental consent forms. The social worker attempted phone contact to parents or guardians a maximum of 6 times, exhausting all available working phone numbers, tracking results with each attempt. If parents or guardians were successfully reached, then follow-up appointments were scheduled with the social worker, who also documented whether or not patients showed. If no successful contact was made via phone following these efforts, then the patient was considered lost to follow-up.
During the phone conversation, the social worker assessed psychosocial barriers and issues, carefully documenting responses to a series of queries about potential barriers to care. Once issues were identified, the social worker provided the intervention to lessen or alleviate barriers, with the hope of continuing the intervention once the patient followed through with the appointment. A few examples of the social worker intervention included: 1. Assisting with insurance referrals from primary care physicians (PCPs) 2. Referring families to community welfare/Medicaid offices for health insurance 3. Assisting children with eyeglass repairs and/or replacements 4. Accessing prescribed medications not covered by insurance 5. Arranging transportation to medical appointments 6. Utilizing interpreter services for non-English-speaking families
The social worker also mailed appointment reminder letters 1 or 2 weeks prior to the patient's appointment, in conjunction with a reminder phone call 1 or 2 days in advance of the expected follow-up appointment. Patients with scheduling conflicts were asked to reschedule appointments via the social worker in a timely manner. The social worker also documented the reasons for appointment rescheduling and the upcoming dates of the follow-up exams.
When patients failed to present for appointments, the social worker tracked the reasons for absence, documented the psychosocial barriers, and rescheduled exams. Patients were scheduled a maximum of 3 times before they were considered lost to follow-up, at which point no further attempts were made to schedule the appointment. The social worker also was available on an as-needed basis to accompany the patient and family in the exam room on the actual appointment day.
Study design
A prospective analysis was conducted using insurance claims data, social worker clinical notes, and patient records data.
Data collection
Demographic data on the study sample was collected from Wills Eye Eagles clinics and GKSD 2012 patient records. Barriers to care were assessed during telephone contact between the social worker and parents/guardians. The intervention continued during the patient's follow-up exams. Costs associated with CECAP were captured in the following cost categories: 1. Social worker time spent with patients and their parents/guardians in delivering CECAP 2. Program materials 3. General project management
Ancillary service costs were not collected in this study. Clinic charges and reimbursements from claims data were evaluated by the specific type of payer: private and employer-based insurance, Medicaid/Children's Health Insurance Program (CHIP), and self-pay/no insurance. All data were de-identified.
Data analysis
Descriptive statistics for variables of interest were calculated for all patients. The frequencies of ocular diagnoses were determined for all patients who attended at least one follow-up appointment. The costs of having a social worker deliver this program were calculated using the time (hours) spent executing CECAP multiplied by the average wage (including fringe benefits) for a social worker in Philadelphia, Pennsylvania, in 2012 based on data from the Bureau of Labor Statistics. 6 For outcomes of interest, t tests were performed to compare means for continuous variables and chi-square tests were used to compare proportions for categorical variables. For all analyses, a value of P<0.05 was considered statistically significant. Statistical analysis was performed using SPSS statistical software, version 19.0 (SPSS Inc., an IBM Company, Chicago, IL). The exploratory geomapping analysis was performed using Google Maps software.
Results
Patient population
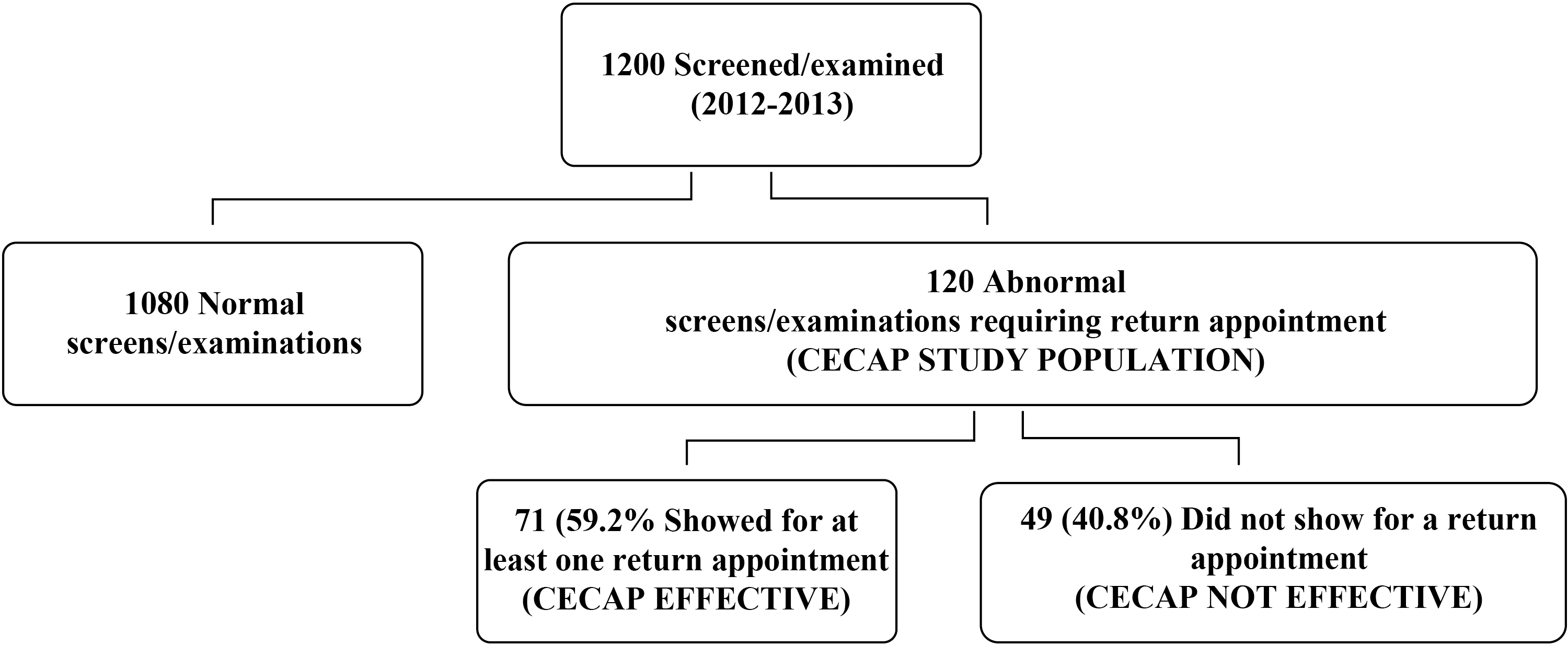
Figure 2 provides a breakdown of the patients who were screened, examined, and required ongoing follow-up pediatric ophthalmic care. A total of 120 children were the subjects of this study. The baseline characteristics of the patients are outlined in Table 1. Of the 120 patients receiving CECAP services, 71 children (59.2%) returned for their recommended follow-up ophthalmic exam, therefore representing the effectiveness of this program.
CECAP effectiveness. CECAP, Children's Eye Care Adherence Program.
t Tests were used to compare means for continuous variables. Chi-square testes were used to compare proportions for categorical variables.
CHIP, Children's Health Insurance Program; NR, did not return for appointments; RFA, returned for appointments; SD, standard deviation.
Barriers
Ten barriers to follow-up were identified and organized into a conceptual framework within 3 categories: 1. Predisposing factors (lack of awareness, level of perceived importance, conflict of commitment, lack of communication means) 2. System factors (lack of referrals, clinic time/scheduling difficulty, lack of transportation access) 3. Financial factors (lack of insurance, health care payment difficulty, transportation payment)
(See Figure A1 available in the online article at
CECAP, Children's Eye Care Adherence Program; NR, did not return for appointments; RFA, returned for appointments.
Relationships between the 10 specific barriers reported and patient characteristics are reported in Table 3. Significant relationships were identified as follows: (1) the youngest age groups (0–5 years and 6–12 years) were less likely to have parents/caregivers who did not perceive the importance of pediatric vision care; (2) difficulty in obtaining referrals for vision care was significantly more likely to be reported in the oldest group (13–18 years); (3) children covered by private insurance were less likely to have parents/guardians who reported that vision care was unimportant—the privately insured population also was more likely to report a lack of communication means. These findings may be confounded by socioeconomic status, as children with private insurance are likely to have better socioeconomic status and, along with that, parents/guardians who have adequate communication means and report that vision care is important.
Values shown in the cells are the number and percent of children within each subgroup reporting each barrier. Bolded text indicates relationships that were statistically significant based on Fisher Exact Test (2-sided) P≤0.05.
CECAP, Children's Eye Care Adherence Program; CHIP, Children's Health Insurance Program.
Diagnoses
The ocular diagnosis reported among children in the CECAP study is presented in online Table A1 (available in the online article at
Cost of CECAP
The costs associated with delivering CECAP to all 120 patients, including expenses for all follow-up visits, are presented in Table 4. The total CECAP program cost was $14,249.25 (118.74 per patient). Furthermore, based on this table, the team determined the CECAP intervention (cost of social worker's time spent with children and their parents/guardians plus social worker's time spent on general project management) accounted for a total of 475.58 hours, which is approximately 4 hours of social worker time per patient. The costs associated with delivering the intervention to the subgroup of 71 RFA patients (Table 5) was $5004.77 or $70.49 per patient who followed up.
CECAP, Children's Eye Care Adherence Program; NR, did not return for an appointment; RFA, returned for an appointment; SW, social worker
Excludes costs beyond the initial follow-up visit.
CECAP, Children's Eye Care Adherence Program; DOS, date of service; NR, did not return for an appointment; RFA, returned for an appointment; SW, social worker.
Clinic charge and reimbursement from CECAP
The amount charged by the clinic and the total reimbursement was assessed based on the patient's method of payment (private insurance, Medicaid/CHIP, or self-pay). For the 71 patients who attended at least 1 appointment, total clinic charges were $24,355.00 with a total reimbursement sum of $6265.66. As a result, the mean reimbursement for delivering CECAP was $63.29 per visit ($88.25 per patient). Table 6 indicates that patients with private insurance have a higher reimbursement rate per visit compared to Medicaid/CHIP and self-pay.
Visits were defined as the number of unique dates of clinic service.
CECAP, Children's Eye Care Adherence Program; CHIP, Children's Health Insurance Program; SD, standard deviation
Exploratory geomapping analysis
To further understand patterns of follow-up among children receiving CECAP, geomapping was used to depict RFA vs. NR patients based on geographic indicators. The general patterns revealed by this geomapping analysis suggest that patients who returned for appointments were more concentrated in western Philadelphia, while those who did not return were somewhat concentrated in northern Philadelphia. Using US Census data from 2010, follow-up rates were compared in Philadelphia based on mean household income and high school graduate rates (see online Figures A2 and A3 available in the online article at
Though mean annual household incomes differ between eastern and western Philadelphia, additional geomapping results show the high school graduation rates of these 2 areas to be ≤85% (Figure A2). Approximately two thirds of patients living in these neighborhoods returned for follow-up. In contrast, the high school graduation rate in northern Philadelphia is lower and 55% of patients returned for follow-up appointments. These results suggest that education level has an impact on follow-up rates for additional vision care.
Discussion
Findings from this study revealed that the CECAP social worker intervention significantly improved follow-up vs. the pre-study period, with an increase from <5% to more than 50%—far in excess of the target. The effectiveness of CECAP represents a nearly 12-fold improvement in rates of patients returning for an appointment among children identified as having vision problems in the community. Analysis of barriers to care indicated that the main barriers for patients who did not return for an appointment were related mainly to predisposing factors: lack of communication, lack of awareness, lack of perceived importance, and conflict of commitments with scheduling.
Of these barriers, the most common was the lack of communication because of home and cell phones not working properly or being out of service. This often was caused by limited access of phone card points or the inability to pay monthly phone bills. There was a lack of consistency with phone service—some cell phones worked while others were out of service for weeks or months at a time. As previously identified in other studies, 2 lack of communication because of inefficient phone service was identified as the major barrier to follow-up vision care.
A second issue of communication involved working with family members who did not speak English as their first language. As of 2012, approximately 12% of Philadelphia's population was foreign born, and another 21.2% speak a language other than English at home. 7 Even with the use of a language–line phone interpreter, it was very time consuming to schedule and coordinate appointments for foreign speaking families. There was often a lack of follow-through on the parent's part, likely attributed to the challenges of obtaining referrals and the difficulty of navigating the health care system.
Additional predisposing factors included lack of awareness and also lack of perceived importance by parents/guardians toward their children's vision problems. These factors affected show rates. For parents with lower income and education levels, there was sometimes a limited understanding of the urgency and/or need to pursue medical care in a timely manner. Some parents/guardians thought their children only needed eyeglasses or a refraction to cure the vision concern. Others had difficulty understanding that their child might have a serious eye disease that might require extensive follow-up care and possibly even corrective surgery.
In terms of the intervention, CECAP required approximately 4 hours of social worker time per patient. The cost of the program per patient, across both shows and no-shows, was $118.74. However, the cost per patient among only those who showed was far less (Table 5). Based on the CECAP cost analysis, the net cost of the CECAP program using the cost of the social worker intervention ($14,249.25) as expenditures and payer reimbursement ($6,265.66) as revenue, was $7983.59. This represents an investment of only $66 per child including both groups of patients who showed and did not show. The majority of CECAP costs were attributable to the social worker's time with patients and parents/guardians.
Although analysis of reimbursements for the RFA patients indicates that revenue generated by CECAP was exceeded by its costs, the program was supplemented by a $20,000 private foundation grant toward the salary of the social worker. Thus, the CECAP intervention yielded a net profit that could be reinvested in increasing the social worker's time with the CECAP program. Therefore, a relatively small contribution of external funding is needed to make this program financially viable. Future implementation of CECAP will examine whether the intervention time can be reduced without compromising its effectiveness, and whether the intervention can be targeted to those patients who are more likely to show. In addition, the exploratory geomapping analysis will be critically evaluated to consider which neighborhoods yield higher rates of patients returning for appointments.
Although a partnership with a primary care medical home may have reduced some of the social worker's time, no letters were sent to the medical home by the social worker. Access to community case managers involved with these children was limited at best, and it took much effort on the social worker's part to even obtain referrals by phone/fax from PCPs when many parents did not bring referrals with them upon their return.
There are several limitations to this study. The findings may not be generalizable as the study sample only consisted of children with eye abnormalities in Philadelphia. Challenges in follow-up care may be different in other settings (eg, urban, rural, varying socioeconomic groups) and with non-ocular disorders. In addition, only intervention costs were collected for this study, which underestimates the true costs of ocular disorders the CECAP population.
Limited information is available about the patients who did not show for follow-up exams at Wills. Preliminary exam records showed potential (but unverified) diagnoses, which most commonly included strabismus, amblyopia, esotropia, and exotropia. Based on these limited data, there is no reason to believe that these patients had potential vision disorders that were any less than those who did show. This leads the research team to suggest that the severity of the ocular concern was not a reason that distinguished those who showed from those who did not.
Conclusions
As described in this report, CECAP significantly improved adherence to eye care from the previous <5% rate to a notable 59.2%. Although room for improvement still exists to meet a higher rate of adherence, the research team surpassed the primary objective of boosting the RFA rate to at least 25%. The motivation for the team to deliver a comprehensive outreach program has been to prevent the long-term biopsychosocial consequences that often burden underserved children. Efforts to deliver this health initiative came at an additional cost, but the research team has successfully constructed a framework that is likely to be scalable to other institutions looking to develop a similar program. Future efforts to refine CECAP should focus on reducing operational efficiencies (eg, capping outreach attempts) and targeting CECAP based on predictors of follow-up. By enhancing these aspects of the program, the team believes another level of efficiency can be achieved, essentially delivering greater outcomes for children at a reduced cost. Capturing program costs is critical for making decisions regarding the affordability, scalability, and sustainability for future vision cost research.
Footnotes
Acknowledgments
The authors wish to acknowledge Elizabeth Cannon-Dang, MPH, for her critical review of this manuscript and William Aultman for his assistance with project management.
Author Disclosure Statement
Drs. Pizzi, Amos, and Levin, Ms. Snitzer, Ms. Prioli, Ms. Steele, declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Prevent Blindness America Investigator Award, 2012, The Foerderer Fund (AVL) and the Robison D. Harley, MD Endowed Chair in Pediatric Ophthalmology and Ocular Genetics (AVL).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.