
Abstract
Many health systems recovering from a massive investment in electronic health records are now faced with the prospect of maturing into accountable care organizations. This maturation includes the need to cooperate with new partners, involve substantially new data sources, require investment in additional information technology (IT) solutions, and become proficient in managing care from a new perspective. Adding to the confusion, there are hundreds of population health management (PHM) vendors with overlapping product functions. This article proposes an organized approach to investing in PHM IT. The steps include assessing the organization's business and clinical goals, establishing governance, agreeing on business requirements, evaluating the ability of current IT systems to meet those requirements, setting time lines and budgets, rationalizing current and future needs and capabilities, and installing the new systems in the context of a continuously learning organization. This article will help organizations chart their position on the population health readiness spectrum and enhance their chances for a successful transition from volume-based to value-based care. (Population Health Management 2015;18:159–171)
Introduction
P
Since that seminal 2008 publication, there have been significant advancements in thinking, innovation, and methods for further defining, measuring, and pursuing the Triple Aim, 2 including supporting legislation and demonstration projects. 3 –7 Specifically, the 2011 Patient Protection and Affordable Care Act promoted a transformation in the underlying business model of health care delivery systems, as well as third-party payers. 8 The Act encourages a transition from the current fragmented system focused on volume-based services toward one that financially rewards patient-centered, coordinated, accountable care through value-based payment models.
The response of health care delivery organizations has been wide ranging. A few bold companies have revised their organizational vision statements in keeping with the Triple Aim, taking board-level accountability for the health and health care affordability in the communities they serve. 9 –11 Organizations like these have taken dramatic and innovative steps to seek out Triple Aim responsibility for a population, regardless of the patient attribution to their delivery system. Other organizations are providing customer guarantees based on cost and quality performance. 12,13
Most health care delivery organizations are at least thinking about where they are on the PHM readiness continuum. Whether driven by vision, leadership, market competition, payer signals, employer demands, or the rising cost of their own employee health benefit, health care delivery and accountable care leaders are facing increasing pressure to define their organizations' PHM strategy in preparation for a shift to value-based reimbursement. 14 –16 There is also burgeoning awareness that traditional health care represents a minor determinant of overall health relative to other determinants (eg, socioeconomic factors, physical environment, genetics). 2
Encompassed in any PHM strategy is the requirement for supporting information technology (IT) and analytics. 17,18 Organizations pursuing PHM transformation have found that their investment in certified electronic health records (EHRs) provides a necessary foundation. However, the investment in their EHR and requisite IT infrastructure is insufficient to support the technology and analytic requirements of new accountable business models. Many of the early organizations aggressively pursuing population health risk-based contracts report that their initial exploration into PHM IT was marked by confusion, unclear vision and IT capability requirements, lack of internal expertise, and build-versus-buy debates without frameworks for decision making overlaid by a succession of overwhelming vendor product demonstrations.
In this paper we acknowledge the challenges facing leaders accountable for PHM IT investment and offer tactics for health care delivery systems and payers to develop and gain support for a PHM IT investment road map. The content of the paper was informed by published literature 17 –20 and case studies, 4 –6,15,21 –27 engagement with organizations with early experience in Medicare, Medicaid, commercial, and employer value-based programs, and interaction with technology vendors.
Challenges Facing Leaders Accountable for PHM IT Investment
Creating an IT investment strategy for any new business model can be a challenge. Beyond this expected challenge, leaders accountable for creating a rational, long-range PHM IT investment road map face additional issues that further complicate the decision-making process.
Ideally, IT strategy is thoughtfully crafted to support a business strategy designed to achieve an organization's overall mission, vision, and business objectives. However, nationally, the health care industry is in the early stages of gaining clarity and cohesion in the various business models that will align payment with the delivery of consumer value. Leaders accountable for creating a rational PHM IT investment road map will be challenged to articulate a concrete long-term strategy given the dramatic business experimentation and learning that is currently under way.
Further, although IT governance has always required political prowess, 28 the rapidly evolving dynamics of PHM can further complicate this process. The evolving Accountable Care Organization (ACO) environment is prompting new configurations of partner networks required to manage outcomes and cost over the full care cycle. Organizations may be thrust into situations that require common PHM capabilities with external partners that otherwise would be considered competitors in their fee-for-service business. As a result, we are seeing shifts in the identity of “stakeholder” and “decision maker” roles relating to PHM IT investment.
Beyond PHM strategy and IT governance, health care delivery organizations often lack key competencies for PHM IT discernment. Fluency with claims data manipulation, interpretation, and actuarial experience critical to competing in the ACO marketplace either do not traditionally reside within a health care delivery organization or may not be positioned to support business model innovation. For instance, health care organizations may have statistical competencies embedded in a research unit that could be applied to predictive modeling; however, that expertise often is not integrated with the strategic planning, care delivery, IT, and business intelligence units.
The alignment of competencies required for PHM is occurring in the wake of the 2009 Health Information Technology for Economic and Clinical Health (HITECH) Act, which stimulated a dramatic shift in the percentage of health care delivery systems and independent physician groups migrating to EHR platforms. 29 –31 To date, the benefits garnered from EHR implementation have been slow to develop. 32 –34 It is clear, however, that successful EHR adoption serves as a foundation to enable PHM. The value of health IT investments will be maximized further when coupled with care redesign and incentive changes promoted by value-based payment models. 32,35,36 Despite the foundational role of EHRs in PHM, Table 1 describes several unintended consequences of EHR implementation that can hamper an organization's ability to develop their PHM IT capabilities.
ACO, Accountable Care Organization; EHR, electronic health record; IT, information technology; PHM, population health management.
Finally, the unprecedented investment in health care technology and analytic innovation that will ultimately result in higher consumer value currently presents organizations with several challenges. Existing technology vendors are consolidating their portfolios to focus on PHM-related solutions. Both established companies and a surge of new entrepreneurs are entering the field with the potential for higher value portfolio and niche products. However, a single, integrated mature solution that meets all PHM IT needs does not exist in today's market. As a result, health care organizations must cobble together their PHM IT solutions.
Rapidly developing technology along with hyped-up sales and marketing promises make it difficult to develop clear build-versus-buy scenarios. Overlap in product functionality across vendor product suites can confuse buyers and/or lead to investment redundancies. These challenges are compounded by the financial pressures that make it difficult for organizations to devote the clinical, business, and technical resources needed to gather requirements, let alone understand the detailed capabilities and limitations of various IT alternatives.
In summary, leaders with PHM IT strategic and investment accountability already face challenges related to current or residual stress from EHR implementation and optimization, budget pressure, hiring and retaining skilled talent, and executing on other high-priority projects (eg, health information exchange, International Classification of Diseases, Tenth Revision, security). The national trend of value-based transformation has added new challenges to this already difficult situation. Recognizing that one or more of these challenges currently exist within an organization enables leaders to work together to mitigate negative ramifications.
Developing and Gaining Support for a PHM IT Investment Road Map
With the health care industry in a state of flux, making shrewd IT investment decisions has never been as critical for an organization's long-term success. Figure 1 depicts a logical, tested process to facilitate PHM IT investment road map creation and prompt stakeholder endorsement. Depending on where an organization is on its PHM, technology, and value-based contracting journey, these tactics may provide a place to start or reinforce existing processes well under way.

PHM IT investment strategy and deployment cycle. IT, information technology; PHM, population health management.
Step 1. Define the organization's PHM business strategy
The process starts with an articulation of the organization's PHM strategy over approximately a 3-year horizon. As clearly as possible, business leaders should summarize the organization's current state, as well as anticipated PHM and value-based contracting strategy.
41
Advanced health care organizations are broadening their services to enhance health and developing wider community-based partnerships. Minimally, a PHM strategy should address the following: • Payer and employer market opportunities • Provider network requirements • Services provided by public health and social service agencies • Existing IT infrastructure and data sources • Potential for nontraditional health care data sources (eg, public health, social services agencies, consumer purchasing patterns) • Existing care process strengths and opportunities based on available cost and quality data • Projected outcome of revenue shift from fee-for-service to value-based contracts
This initial step is critical to lay the foundation for creating a PHM IT road map that inspires confidence. This first step also can be leveraged in a parallel change management strategy that will be required to succeed in PHM. Although challenging, most organizations understand the need to engage employed and affiliated providers in the anticipated changes for their practice and/or business. Often overlooked is the opportunity to formally engage the IT, informatics, and business intelligence staff as key partners in the expanded PHM vision.
Step 2. Clarify PHM IT governance
As a derivative of corporate governance, IT governance is critical to forging the connection between business strategy and IT for value creation. With the PHM business strategy articulated from Step 1, the role of business leaders in the governance process is that of ultimate decision maker as well as taking subsequent accountability for return on investment. IT exists to serve the clinical and business functions of the organization. In their supporting role in the governance process, IT partners provide the business with options to meet the PHM business strategy. Role clarity and a collaborative partnership are integral to the subsequent steps in the cycle.
To the extent not already accomplished, the organization should design, approve, and socialize an IT governance process that aligns investment with the PHM business strategy. 28,42 To ensure an efficient and effective decision-making process, leaders should take stock of the maturity of existing IT governance processes, and proactively determine the need to expand, alter, or reinforce the process. When multiple health care delivery systems partner to manage populations, the IT governance process within a single organization may no longer serve as the vehicle for PHM IT investment decision making. In this more complicated scenario, executives across organizations will need to invest time in forming an overarching IT governance process that can comprehend the individual position and needs of each participating organization, along with their shared PHM IT needs.
Organizations may feel pressure based on signed, at-risk contracts to make rapid IT decisions. However, we have witnessed cases where failing to explicitly address this step has caused potentially avoidable strife within and between organizations, ultimately causing further delays or poor investment decisions.
Step 3. Create business requirements based on PHM stakeholders and their Jobs-to-be-Done (JTBD)
With an explicit PHM business strategy and an effective governance process, the organization is ready to consider its detailed PHM business requirements. Unfortunately, many organizations stall at this step because of an impasse between business leaders expecting their IT counterparts to describe how technology will enable PHM (ie, tell me what the technology will do for me), and IT leaders expecting business leaders to describe their PHM business needs (ie, tell me what functions you need done).
The JTBD framework 43 can provide the necessary bridge between PHM business needs and potential technology solutions. In this case, the JTBD specifies the PHM problems that must be solved (ie, jobs to be hired) by IT to efficiently and effectively deliver on Triple Aim outcomes for specific populations. When constructing the JTBD categories, it is enlightening to consider who will be the primary stakeholder responsible for each PHM job. Table 2 describes 4 categories of PHM stakeholders, along with their potential roles and perspectives.
With an understanding of the PHM stakeholder perspectives and their high-level JTBD, PHM business requirements can be created to support each job. Investing the time to create ideal future state PHM business requirements enables organizations to assess current capabilities, consider build-versus-buy alternatives, communicate their future direction to vendors, and seek innovative new solutions and partners for solving their PHM challenges.
The writing and socializing of PHM business requirements can be complicated by terminology. The language that surrounds PHM finds it roots in multiple sources, including hospitals, ambulatory clinics, health insurance plans, public health, and the technology industry. Depending on the source, terms such as “case management,” “care coordination,” or “patient engagement” may hold different meanings depending on the historical context, user role and/or marketing spin. These language nuances must be explicitly comprehended in the requirements to ensure astute evaluation of IT alternative solutions and, ultimately, wise investment.
Organizations' ideal PHM business requirements may be influenced by their PHM strategy, breadth of service offerings, and specific target populations. Additionally, there is certainly more than one “right” way to categorize PHM JTBD and business requirements. Given that, there are advantages to creating a single internal PHM business requirements document. Primarily, the document will align internal stakeholders and enable an apples-to-apples comparison of IT alternatives. In the absence of a designated document, each vendor will propose their own format and language, creating havoc for both analysts and decision makers. Using a multidisciplinary team and an interactive process, we have created, tested, and revised a list of PHM JTBD and business requirements (Table 3). We have found that this parsimonious list has resonated with clinical, business, and IT leaders in multiple organizations. Teams might find the information in Table 3 a useful starting place or might use the information for comparison with their own current thinking.
EHR, electronic health record.
Some organizations may find that the creation of ideal future state PHM business requirements is sufficient to support their IT road map development and subsequent product evaluation. Given limited resources, other organizations will determine that not all requirements are equally important given their current environment. Accordingly, a weighting system will assist these organizations to allocate their IT investment across short- and long-term priorities. Alternatively, teams might create a subset list of minimum or “must have” requirements.
Once drafted, the business requirements should be circulated with all the relevant stakeholders for feedback and revision. The circulation and sign-off on the PHM JTBD and requirements document can serve to educate, engage, and align leaders. As with any strategic document, the PHM requirements should be considered a working document that will evolve with changing market dynamics, organizational capabilities, and technology advancements.
Step 4. Conduct a gap analysis between PHM business requirements and current IT capabilities
Many organizations moving toward accountable PHM are, understandably, in the fledgling stage. As a result, their initial list of “must have” PHM business requirements is at high risk of changing. Creatively leveraging existing technology and options for rapid learning can advance an organization on its journey quickly and at a low cost of entrance.
Table 4 provides a template for considering how existing systems may provide the capabilities needed to fulfill an organization's PHM business requirements. The intent of the template is to quantify the ability of various IT alternatives to deliver on an organization's PHM JTBD. For instance, as a manual workaround, capable analysts can work in a spreadsheet to accomplish a business need. Once the volume of data increases, the need to scale exists, and funding is available, the organization can upgrade to a more sophisticated, automated, and integrated solution.
“+” represents the extent to which an IT system can accomplish specific business requirements within a JTBD category. The rating assigned to any IT system will vary based on the specific needs of the stakeholder and the capabilities of their specific IT system.
EHR, electronic health record; JTBD, jobs-to-be-done; PHM, population health management.
We observe organizations struggle to gain clarity on the potential of their existing EHR to deliver on their PHM business requirements. Certainly, there is benefit to leveraging existing technology and minimizing the complexity of the organization's IT architecture. Additionally, the HITECH Meaningful Use EHR certification program 44 impels EHR vendors to provide foundational components for at least basic PHM. The allure of relying on the existing IT system must be considered in balance with potential limitations. Considerations include the breadth of EHR capabilities relative to the PHM business requirements for each stakeholder, speed to market of new functionality, ability to leverage alternative data sources and integrate with other solutions, and the organization's backlog of existing EHR projects and resource constraints.
Assessing current state IT capabilities also requires a meticulous understanding of the advantages and disadvantages of available data sources in relation to the needs of specific user roles. For instance, claims information generated from billing data can provide insights into population-level cost of care opportunities, as well as specific patient-level care gaps opportunities. Accordingly, a business intelligence solution incorporating claims data may provide health care executives with sufficiently accurate information to identify high-level cost savings and determine population-based program development opportunities. However, the imprecision and time lag of claims data often render this an unacceptable data source to support automated messaging from a physician to his or her patients regarding recommended care changes. For instance, an automated message prompting a breast cancer survivor to schedule a mammogram following breast removal surgery is unacceptable from the perspectives of physicians and patients alike. Any solution that attempts automated patient outreach must include a mechanism to capture patient-specific information to enable mass customization of patient activation messaging while maintaining and even promoting the intimacy of the patient-provider relationship.
At the completion of this step, organizations should have a solid understanding of how their existing technology investments might be leveraged to support the organization's PHM strategy. It is common to find that many stakeholder JTBD can be supported using existing platforms. Doing so enables the organization to learn quickly and refine its specific business requirements. However, additional investment in a new PHM solution ultimately may be required to scale a program across the organization, drive standardization and efficiency into the process, and/or integrate functions with other stakeholders.
Step 5. Create a PHM IT investment road map, budget, and time line
Desired business requirements not met in the current state should be identified and prioritized for investment. When considering budget allocation, IT investments should be balanced and, ideally, synchronized with investments in care model redesign. For example, a sizable investment in a sophisticated data warehouse with longer term deliverables of integrating data from multiple sources should be balanced with short-term registry investment to immediately support care teams' improvement capabilities. Similarly, purchasing a high-end case management platform could be premature in the event that care coordinators have not been hired, trained, and incorporated successfully into care teams.
Business leaders should consider developing an estimate of revenue improvements or expense reductions (either in utilization or cost of delivery) that PHM IT implementation, along with care model redesign, is expected to yield. Budget adjustments or capital requests may be warranted or justified based on this potential return on investment. Lastly, when investment in an external solution is warranted, it is wise to keep in mind that the PHM IT market is immature and vendor consolidation is likely. These points argue for shorter term purchasing commitments with reevaluation in several years.
Step 6. Analyze external alternatives to fulfill unmet PHM business requirements
The unmet PHM IT needs of burgeoning ACOs and health delivery systems have spurred the rapid entrance, adaption, and/or evolution of multiple IT market alternatives. To assess IT market maturity, we start by defining “mature.” Classically, a mature market is defined as one that has passed the emerging and growth phases of industry development. 45 More specifically, we believe that the characteristics of a mature PHM IT market will include products that cover all or most JTBD, assimilate multiple data types, contain preconfigured evidence-based decision support for all stakeholders, enable plug-and-play installation, and provide easy access for all stakeholders with seamless integration across users. By this definition, the PHM IT market is decidedly immature, although rapidly evolving. Companies with historical roots in the insurance industry and disease management are working to develop more integrated platforms to cover a broader spectrum of PHM IT capabilities. However, at the present time, no single platform covers the breadth and depth of the PHM IT requirements represented in Table 3.
An organization that has clearly articulated its PHM business requirements, understands current state IT capabilities, prioritized unfilled PHM business needs, and determined budget and time line is well prepared to make discerning PHM IT investments. At this point, the organization should appoint a person or small team, under the guidance of an executive sponsor or committee, to conduct an analysis of alternatives. Given the complexity of the topic and overlap in solutions, we have found the following process to be expedient while yielding a robust outcome.
We suggest sending a request-for-proposal (RFP) composed of the organization's PMH business requirements to a narrowed field of vendors. It is helpful to vendors when background information on the organization (eg, PHM goals, number and type of providers, number of covered lives, time line for decision making) is included in the RFP. We found that it is essential to provide mandatory self-scoring instructions with clear, distinguishable scoring definitions in order to optimize the chances of receiving standardized vendor responses.
To validate the extent to which a product's suggested capabilities match the reality of the offering currently available in the market, we suggest a “deep-dive” assessment of viable alternatives. The deep-dive assessment, which differs dramatically from the typical vendor-driven demonstration, is conducted with a select few team members. In preparation for the deep-dive reviews, the team should create role-based use-case scenarios. The scenarios should consider the user perspectives that the business requirements must ultimately serve (Table 2). This provides a practical approach for the vendor to illustrate current product capabilities and/or acknowledge shortcomings.
We have found that deep-dive assessments are conducted successfully in person or remotely and typically require 3 to 5 hours per vendor product, depending on the breadth of solution capabilities. The deliverable from the deep-dive assessment and vendor interview is an internally validated rating of each product's capabilities against the organization's specific requirements. Additional time is required to complete product license and services quotes, estimate internal resource requirements, and interview existing customers for the final list of vendor alternatives.
Product demonstrations for all relevant stakeholders involved in investment decisions should be reserved for comparison of the final alternatives once all product information is gathered, compiled, and analyzed by the appointed clinical and technical team. Creating a visual display of the results aids decision makers by distilling complex criteria across multiple vendors into a color graphic that incorporates both functionality and cost. Our experience is that this methodology is efficient, maintains the governance process, and generates confidence-inspiring results that enable fact-based decision making.
Step 7. Implement PHM IT solutions in the context of a learning system
Organizations that have successfully traversed the previous 6 steps can, and often do, under-consider and under-resource this final step. It could be argued that this last step should, in fact, top the list of steps. It requires heroic effort for health care delivery systems to begin the transformation to a health and wellness focused business. Beyond implementation of technology, successful transformation requires leadership, planning, infrastructure and workflow design, measurement, and self-study. 26,46 –48
Successful learning organizations implement technology, information, and process within a supportive learning environment to create a cause-and-effect loop (Fig. 2) that encourages relational understanding and improvement of the system as a whole and its various components. 49 When redesigning processes, recognize that PHM stakeholders (ie, executive, mezzanine, frontline, and patient and family) will be on a continuum of embryonic to mature regarding their insights into their own needs, as well as their relationship to the needs of other user roles. Rapid production and deployment of actionable information within a well-executed project plan can promote learning and advancement within and between user roles.
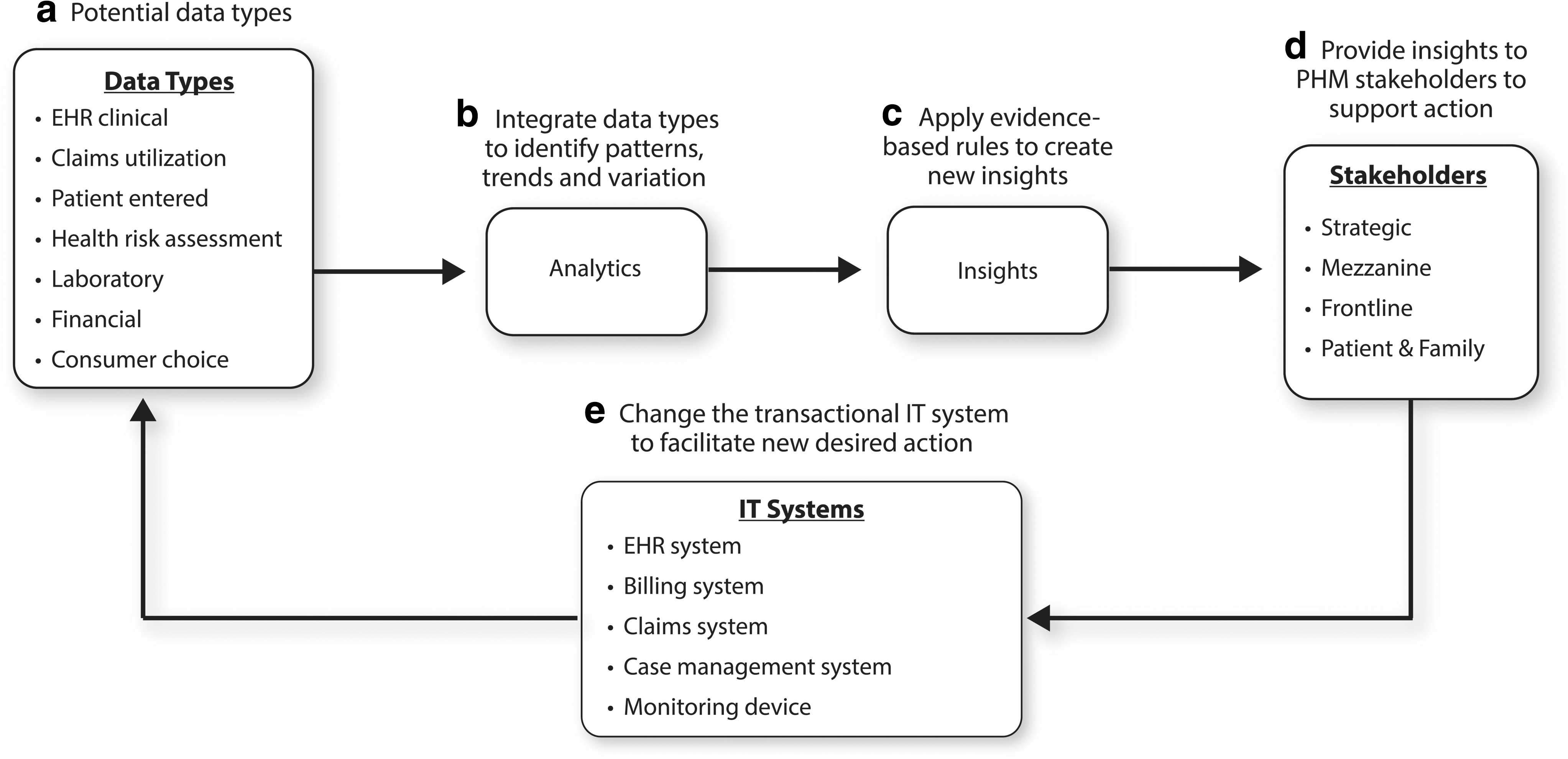
Feedback loop to support continuous learning and improvement. EHR, electronic health record; IT, information technology; PHM, population health management.
Team learning, built on personal mastery and shared vision, is another principle of a learning organization. We are impressed by the large and growing body of evidence demonstrating that workflow redesign emphasizing “team-based care” improves safety, quality outcomes, patient experience, and provider satisfaction. 50 Many organizations are investing in developing more team-based care models. Not surprising is the finding that team cohesion is associated with higher adoption and diffusion of health IT. 51,52 Thus, organizations that have been successful in creating high-performing teams with clear role-based workflows can expect that their investment in PHM IT will yield greater return.
At a high level, the 7 steps identified represent a logical approach to identifying any type of high-priority IT investment. However, during times of significant challenge and industry stress, it serves an organization well to ensure broad understanding of the process and fastidious execution of the steps.
Conclusion
Organizations embracing the transformation from traditional fee-for-service to value-based PHM are finding significant gaps in their IT capabilities. Shifting business models and care delivery partners complicate the IT governance, evaluation, and selection process. In the future, new data sources, funding, and innovation will drive more robust and patient-centered health IT development to enable superior Triple Aim performance. However, today the PHM IT market is immature. Most organizations find that more than 1 solution must be developed or purchased to close their PHM business requirement gaps. Executing a thoughtfully designed PHM IT evaluation methodology will bolster an organization's ability to make astute investment decisions. Ultimately, maximizing the value of any PHM IT investment is highly dependent on the extent to which teams work in a learning system to support continual innovation and improvement.
Footnotes
Acknowledgment
We would like to extend our thank you to Jane Rossner, PhD, at the Institute for Healthcare Improvement and David Barnes at Providence Health & Services for their support in manuscript review and preparation.
Author Disclosure Statement
Drs. Hunt, Gibson, Whittington, and Wozney, Ms. Powell and Ms. Knudson declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Providence Health & Services transferred intellectual property ownership of the CareManager software application to Kryptiq Inc. Dr. Hunt receives a portion of the royalty revenue generated from this transfer. The other authors declared no conflicts of interest. The authors received no financial support for the research, authorship, and/or publication of this article.