
Abstract
Lessons learned by countries that have successfully implemented coverage schemes for health services may be valuable for other countries, especially low- and middle-income countries (LMICs), which likewise are seeking to provide/expand coverage. The research team surveyed experts in population health management from LMICs for information on characteristics of health care coverage schemes and factors that influenced decision-making processes. The level of coverage provided by the different schemes varied. Nearly all the health care coverage schemes involved various representatives and stakeholders in their decision-making processes. Maternal and child health, cardiovascular diseases, cancer, and HIV were among the highest priorities guiding coverage development decisions. Evidence used to inform coverage decisions included medical literature, regional and global epidemiology, and coverage policies of other coverage schemes. Funding was the most commonly reported reason for restricting coverage. This exploratory study provides an overview of health care coverage schemes from participating LMICs and contributes to the scarce evidence base on coverage decision making. Sharing knowledge and experiences among LMICs can support efforts to establish systems for accessible, affordable, and equitable health care. (Population Health Management 2015;18:265–271)
Introduction
A
Based on a report from the Social Security Department of the International Labour Organization, almost 50 of its member countries have UHC. 2,6 Of the remaining, almost all LMICs are in the midst of transitioning toward UHC. 7,8 In the wake of the WHO 2010 World Health Report on the path toward UHC, more than 50 countries have contacted the WHO Secretariat to request technical assistance. 5 Experts acknowledge that, even under the most favorable planning scenarios, many countries will still face tremendous financial and organizational constraints in attaining UHC. 9 For example, in many LMICs, different socioeconomic groups often are covered by different funding pools and served by different providers, creating barriers to the successful creation and implementation of UHC. Entities involved in health care coverage decision-making processes (eg, legislators, administrators, researchers) are discussing how best to invest available resources, taking into consideration burden of disease, social protection and values, scientific evidence of therapeutic effectiveness, capacity of the health system to deliver care, and affordability. 9 –12 Important questions about who should be covered, what conditions or services should be covered, and when coverage should be applied must be addressed.
Countries are encouraged to share their experiences in developing and/or expanding their coverage schemes, with the understanding that the options for transitioning toward UHC must be developed within the particular macroeconomic, sociocultural, and political context of each country. 3,5,13,14 This study was conducted to review and document the characteristics of health care coverage schemes in LMICs and to explore the influential factors in the decision-making processes. The primary objectives are to review the characteristics of health care coverage schemes in participating LMICs and to identify the factors that may influence health care coverage decision making in achieving UHC.
Methods
Study design
For the purposes of this study, a health care coverage scheme was defined as “a delivery system or specific scheme established to guarantee organized access to necessary health care services while providing protection against financial risk.” 3 A target list of LMICs was generated based on gross national income (GNI) per capita data as reported by the World Bank. 15 A total of 144 of the 214 countries whose GNI was reported were LMICs, including 40 low-income, 56 lower-middle income, and 48 upper-middle income countries.
For each health care coverage scheme, the research team identified individuals who could provide expert insights on the decisions and processes used to form coverage-related policies. At least 1 of the following criteria had to be met for participation in the study: (1) member of the target Ministry of Health; (2) academic researcher studying coverage issues for the target health care coverage scheme; and (3) administrator of the target health care coverage scheme. Contact information was obtained from publicly accessible sources when possible, and professional networks or international conference participation otherwise. Participants were approached via e-mail stating the purpose of the study and an honorarium of USD200 per hour was offered for participation.
An online survey was administered, and responses were validated through interviews conducted using a semistructured guide. For the health care coverage schemes that were assessed during the second stage, the types of funding mechanisms were documented. Funding mechanisms were categorized as: (1) public insurance (ie, financed primarily by public funding); (2) social health insurance (ie, funded by contributions from a variety of stakeholders such as employees, self-employed, enterprises, and government); (3) private health insurance (ie, purchased by individual buyers from private insurers); (4) tax-based financing (ie, funded by government general revenue); and (5) community-based health insurance (ie, financing controlled by communities through locally based prepayment schemes). 16
For each participating LMIC, data on demographics and developmental indicators were collected and validated by the informants. Demographic characteristics included population size and geographic region. Developmental indicators included health and education status, MDGs, economy (ie, GNI per capita), and political structures of the countries; these data were retrieved from global databases available in the public domain and compiled by the WHO, the UN, and the US Central Intelligence Agency. 15,17 –22 The following topics were addressed in the first stage through the online survey: (1) type of health care coverage scheme, (2) enrollment criteria, (3) funding sources and distribution of funds, (4) coverage for health conditions and services, (5) evidence used to make coverage decisions, (6) coverage policies regarding drugs and medical devices, (7) restrictions on coverage, (8) outcomes monitoring and quality assurance, and (9) future plans (eg, forthcoming revisions of policies). Descriptive statistics were computed for all quantitative data. The information on health care coverage decisions collected through the study was mainly qualitative in nature.
Results
At least 1 informant with contact information was identified for 58 of the 144 eligible health care coverage schemes. Participants from 25 health care coverage schemes agreed to participate in the study (Table 1). The surveys were completed between September 2010 and May 2011. Approximately 52% of the respondents described themselves as academic health services researchers and the other 48% were self-identified in the field of health technology assessment or affiliated with health care coverage scheme administration. The most commonly reported criteria for coverage scheme eligibility pertained to age (n=15), citizenship (n=12), and income (n=11). Other criteria included employment status (n=8), sex (n=7), disability status (n=7), and disease status (n=3).
HTA: health technology assessment; UHC: universal health coverage.
Participated in in-depth second stage case study.
RSBY covers health services for 25 states, whereas the Chiranjeevi Scheme services the state of Gujarat specifically.
A total of 25 conditions and types of care were listed as one of the top-priority conditions for the coverage scheme (Table 2). Maternal/antenatal and neonatal health were most often listed as top-priority conditions for coverage, identified from 9 (36%) health care coverage schemes. Other top-priority conditions included cardiovascular disease, cancer/oncology, and HIV.
Health care coverage schemes also had policies on coverage for specific supplies and services. All health coverage schemes provided some level of coverage for medications. Most coverage schemes (n=22; 85%) had an “essential medicines” list. More than half (n=13) of the coverage schemes indicated that beneficiaries of the health care coverage scheme had to make some form of out-of-pocket payments; co-payment was the most commonly reported type of out-of-pocket payment.
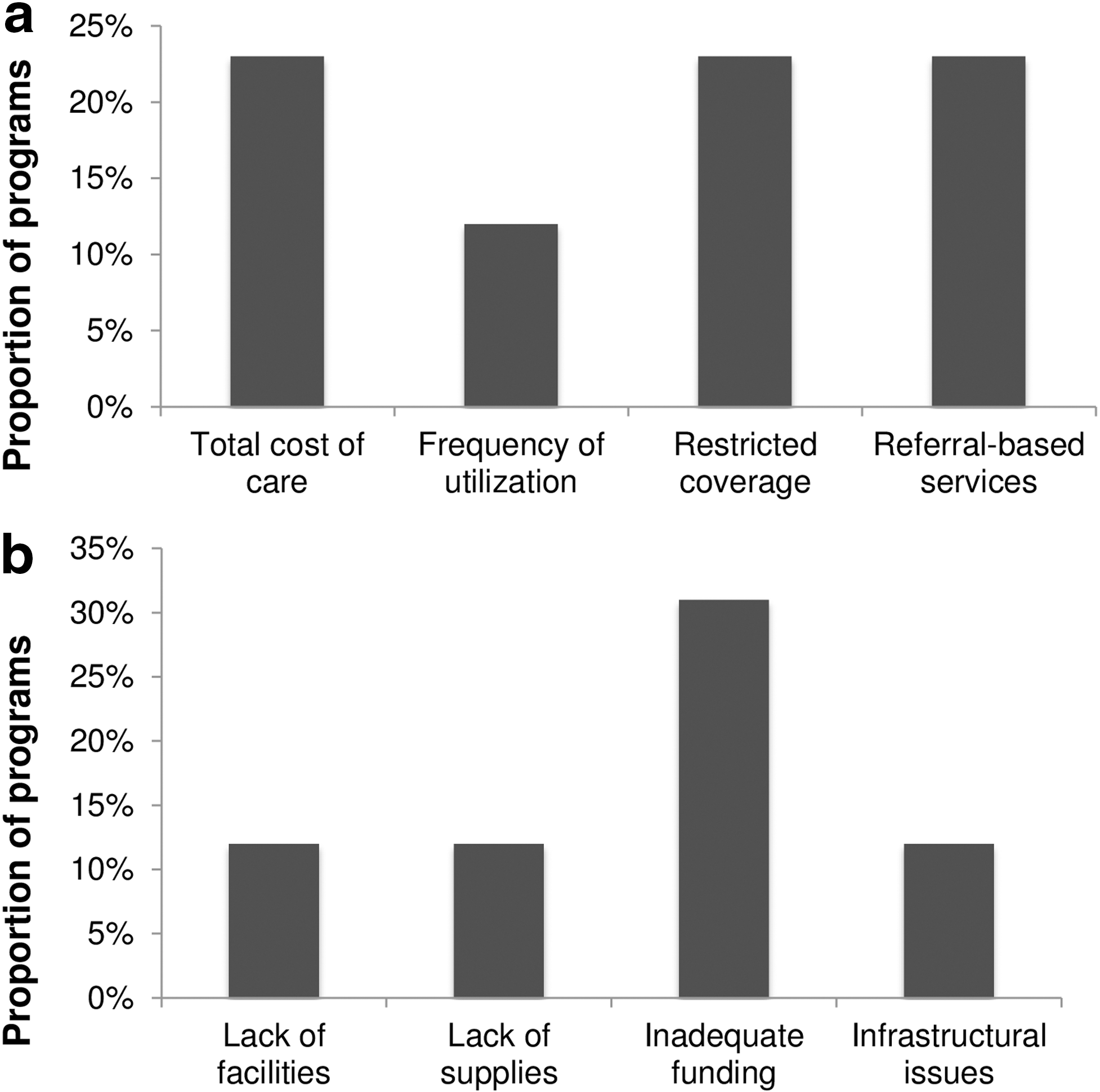
Information was collected on factors that influence coverage decisions for top-priority conditions. The evidence used to make decisions on coverage included published guidelines, reviews of medical literature, global and local research studies, and health coverage policies of other schemes (Fig. 1). Political polls and media reports were seldom used in decision making. Participants from approximately one third of coverage schemes reported that economic appraisals were undertaken to determine the coverage policies for drugs and medical devices. Twelve coverage schemes had policies that restricted the use of services through spending limits, limited numbers of services or visits, or services that could be provided only after referral to a specialized facility (Fig. 2a). Inadequate funding was the most commonly reported reason for restricting coverage (Fig. 2b).
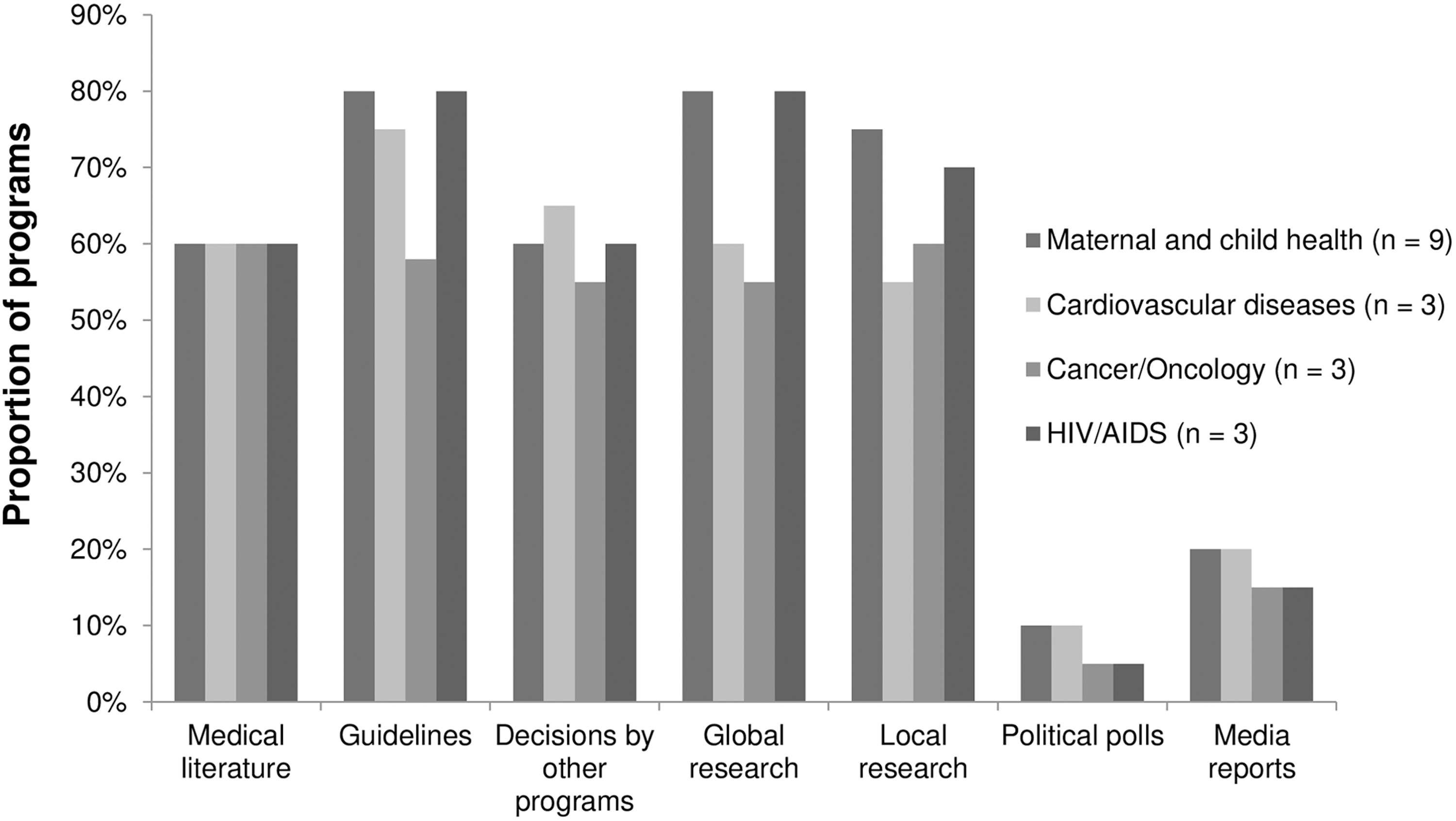
Evidence used in decision making for top-priority conditions
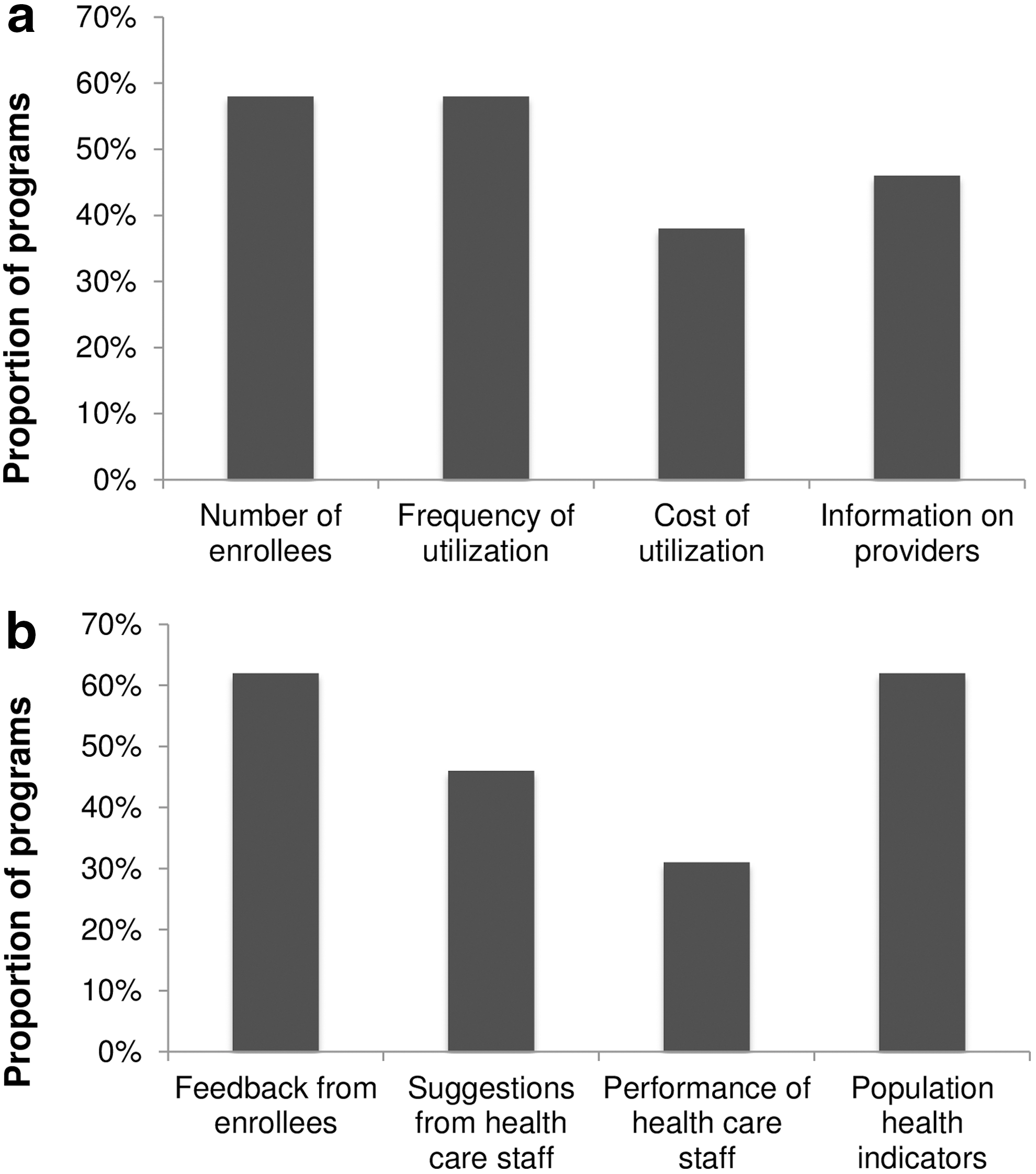
Data on beneficiaries, utilization of services, and services providers were monitored by approximately 50% of the health care coverage schemes (Fig. 3a). More than half of the health care coverage schemes monitored quality using metrics such as feedback received from beneficiaries and statistics on health indicators (eg, maternal and child mortality, prevalence of infectious diseases) (Fig. 3b).
Discussion
Despite complex financial and organizational hurdles, many LMICs are transitioning toward UHC for all citizens. 23 –25 The global trend toward UHC creates new opportunities for governing bodies to compare political ideologies, health care decision-making processes, and coverage decisions. 26 The approaches taken toward health care coverage reform varied across the LMICs represented in this study. This study explores some of the challenges faced by population health management decision makers in achieving UHC.
Findings bring to light a number of areas for future studies. It is necessary to develop a more complete understanding of the relationship among level of health care coverage, processes of health care delivery, and population health. Such evidence from health system research will help in the creation and adaptation of health coverage policies that are feasible to implement, are likely to have the greatest impact for the largest proportion of citizens, and are the most affordable. Decision-making processes and health care coverage schemes varied widely across LMICs. The interview data showed this variation extended to the terminology used to describe basic concepts (eg, enrollment eligibility) as well as the conditions and services to be covered under the health care coverage scheme. A standardization of coverage policy terminology may improve evidence to support decision making in health care coverage reform and promote progress toward UHC.
Another important aspect of the findings is that they represent a set of heterogeneous functional mechanisms and financing structures for health care delivery and coverage schemes. A successful financing structure is critical for LMICs to achieve UHC goals. Investigating the relationship between the financing structure and the health care coverage schemes will provide valuable information in facilitating LMICs with the transition. Interviews also highlighted the role of political influence in pursuing UHC goals. Different political ideologies and levels of political commitment perhaps determine whether a country has tax-based versus social health insurance, or a single scheme versus multiple schemes. Studying the direction of this influence among LMICs would be useful in the future.
The most reported information source influencing the decision makers was scientific evidence on disease epidemiology, suggesting that robust epidemiological studies in LMICs would improve understanding and promote informed decision making. Among the health care coverage schemes studied, inadequate funding was the most frequently reported reason for coverage restrictions in the majority of LMIC's health care coverage schemes. However, increasing funding alone would be ineffective in achieving UHC unless coupled with appropriate leadership and increased public awareness of social health protection. 27,28 Health care coverage schemes used outcomes such as feedback received from beneficiaries and statistics on health indicators to monitor the quality of health care services. Future studies on how these outcomes are being utilized can provide insight into how to improve the service quality.
A recent study published by McIntyre et al collected evidence on factors that facilitate or hinder progress toward UHC reform for 7 LMICs. 29 The study reported that Thailand has made an explicit commitment to ensuring financial protection, while this was not necessarily the case in countries adopting targeted reforms, especially in African countries where the burden of disease is particularly concentrated. It is interesting to note that the development stage toward the UHC goal in these LMICs has remained more or less the same over the past couple of years.
A systematic documentation of decision making and sharing experiences with health care coverage scheme development across LMICs are critical steps to achieving UHC goals by enabling decision makers to learn from prior accomplishments and to develop a better understanding of effective policies and practices. The information provided herein can be used in several ways to support UHC achievement in LMICs. Through decision and policy comparisons across institutes, improvements made by one country may shed light on solutions to coverage policy gaps in another. These comparisons may help promote more efficient use of resources. Tracking trends of key indicators is a necessary step to understanding what works and what does not in human development initiatives. Tracking health system indicators (eg, infrastructure, processes, outcomes) is integral to learning what works in health care. 4,30 Various local and international organizations routinely track health outcome indicators.
To facilitate information sharing on health care coverage decision making, the present study (1) avoided linking the identities of health care coverage schemes to specific decisions or findings from that coverage scheme; (2) provided remuneration for participants' time; and (3) provided a standardized, easy-to-use data collection instrument. Participation in this study was voluntary. Though a significant incentive was offered to LMICs for participation, informant enrollment proved challenging. The most common reason given for nonparticipation by the informants contacted was insufficient resources and time. Several persons declining to participate indicated that discussing decision making involving multiple stakeholder interests is a delicate topic, and/or voiced concern that such research may suggest that the coverage schemes were unsuccessful in achieving their stated objectives. It also is considered that health care coverage schemes or countries that were not included in the study might be those in which cross-country health services research may not be an important factor in decision making. The findings presented, therefore, may be more representative of countries wherein health services research was a high priority.
This study examined the health care coverage decision-making processes from a population health management and academic perspective. However, the processes establishing health care coverage schemes involve many different stakeholders such as health care providers, patients, and beneficiaries. Therefore, future studies are encouraged to assess health care coverage reform processes from a different stakeholder's perspective in order to build a more comprehensive understanding. Additionally, it would be valuable to see how these policies impacted actual health outcomes. Because enrollment was low, interpretation of the results is limited by the inability to validate information on each health care coverage scheme across multiple regions. Therefore, the study should be viewed as exploratory in nature; future studies that focus on specific issues related to coverage in various strata of health care coverage would be useful.
Conclusion
This study provides an overview of health care coverage schemes from 7 LMICs and contributes to the evidence base on the factors that influence decision making in achieving UHC, which is a critical component of sustainable development and reducing social inequities. The information collected in this study suggests that the out-of-pocket payment in LMICs is very high along with strong financial and political factors influencing coverage decision making. The goal of UHC is to provide an increasing number of health care services over time while reducing out-of-pocket costs for patients. Sharing knowledge and experience on health care coverage schemes among LMICs will support efforts to establish systems for accessible, affordable, and equitable health care for all citizens.
Footnotes
Author Disclosure Statement
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received the following financial support for the research, authorship, and/or publication of this article: This work was supported by a research grant from the Rockefeller Foundation. The sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The authors had full access to all of the data in the study and had final responsibility for the decision to submit for publication. Dr. Hornberger, Ms. Gutierrez, Ms. Dai, and Ms. Shewade are/were employees of Cedar Associates LLC, and received the research grant from the Rockefeller Foundation. Drs. Mendoza-Arana, Gómez-Dantés, Jain, Teerawattananon, and Nabyonga-Orem received honoraria from Cedar Associates LLC for their participation in the current research. Ms. Khonelidze and Dr. Saleh may have previously received research grants and/or honoraria from the Rockefeller Foundation. Dr. Nishtar has previously received research grants and/or honoraria from the Rockefeller Foundation.