
Abstract
Patients with multiple chronic conditions (MCCs) are a significant concern for the US health care system. MCC patients represent an increasing proportion of the US population and are associated with increased health care cost and utilization, and poor quality of care. Research that has been conducted on MCC patients to date has been at the national level using large data sets, such as Medicare and Medicaid claims and the National Inpatient Sample. These studies have produced research evidence that may be of little utility to individual employer-based health plans given the inherent differences in the patient populations they serve. This study analyzed evaluation and management claims for patients ages 18 years and older (n=632,477) from the Beaumont Employee Health Plan (BEHP), a regional health insurance provider serving Beaumont Health System employees and their families across Southeastern Michigan. The study found that individuals with MCCs are associated with increased cost and visits, and decreased time between appointments in the outpatient setting. Despite decreasing prevalence of MCCs over the study period, substantial increases in cost and visits, and a decrease in time between appointments was observed for MCC patients. Asthma and chronic back pain were uniquely identified as additional primary targets for disease management programs for employer-based health plans. These findings speak to the value of studying MCCs at the employer-based health plan level, where population-specific MCCs can be identified for meaningful intervention and management. Significant opportunity exists for employer-based health plans to study, prevent, and manage MCCs among adult patients. (Population Health Management 2015;18:421–428)
Introduction
N
As of 2010, 96 million Americans (32%) were estimated to have MCCs, which represents an 8% increase in MCC prevalence since 2001. 3 MCC prevalence will continue to rise in the United States as the baby boomer population grows older and acquires new and/or additional chronic diseases, and as younger populations are continually exposed to chronic disease risk factors. Approximately 80% of individuals 65 years and older are known to have MCCs, while 49% of individuals ages 45–64 and 18% of individuals ages 18–44 have MCCs. 3 Our health care and public health systems must be prepared to successfully treat and manage these patients who will undoubtedly become even more numerous and clinically complex over time.
Patients with MCCs have health care experiences unlike those of individuals with acute conditions. MCC patients are burdened with fragmented and uncoordinated health care appointments to arrange, numerous instructions from different providers to decipher, and multiple treatments and prescriptions to manage, all while attempting to maintain a balanced life as well as care for their families. 4 Health care costs are disproportionately higher for MCC patients. Approximately $.71 of every dollar spent on health care in the United States is used to treat MCC patients. 3 With every additional chronic condition a person has, inpatient and out-of-pocket costs are known to increase drastically. 5 –7 Additionally, a number of studies have found that patients with MCCs have more inpatient admissions, hospitalizations, primary care consultations, and outpatient visits compared to patients without MCCs. 8,9 In fact, almost 40% of all physician office visits in the United States can be attributed to patients with MCCs. 10 Although convincing evidence indicates that MCC patients experience poorer quality of care related to absent care coordination, 11,12 inappropriate treatment, and inadequate disease management, notable studies have found that MCCs may be associated with increased health care quality. 13 –16
In the United States, MCCs have been studied primarily on the national level using large data sets, such Medicare and Medicaid claims, the Healthcare Cost and Utilization Project's National Inpatient Sample, and numerous national health surveys. 17 Although these data sets are advantageous for epidemiological investigations and establishing generalizability, it is difficult for employer-based health plans, in particular, to use information obtained from these studies to definitely target specific MCCs for meaningful intervention. Employer-based health plans represent practical and manageable systems wherein critical health care improvements can be designed, tested, and standardized for MCC patients, such as the rollout of new and innovative disease management programs. 18 –20 In addition, prior published evidence may be of little utility to individual employer-based health plans given that these plans serve patient populations that are generally younger, healthier, and more affluent than those previously studied. Therefore, the purpose of this investigation was to investigate MCC prevalence, and to determine the relationship between MCCs and health care cost and utilization in the outpatient setting among enrollees of a regional employer-based health plan.
Methods
Study population
Outpatient evaluation and management claims (n=632,477) from the Beaumont Employee Health Plan (BEHP) were analyzed to study MCC prevalence, cost, and utilization for the years 2008 through 2013. BEHP is a regional health insurance provider serving Beaumont Health System Employees and their families across Southeastern Michigan. Beaumont Health System is comprised of 3 primary health care campuses (Royal Oak, Troy, and Grosse Pointe, Michigan) and numerous other satellite clinics and facilities. This study utilized BEHP data for both employees and their dependents. As part of their health management program, BEHP employs nurses to serve as health advocates and coaches for BEHP patients. These nurses are responsible for telephonic outreach, disease management/case management, patient education, disease self-management skill development, and providing support to BEHP members and their families to maximize health outcomes and reduce the long-term effects of chronic illness. Nurses also perform other clinically based duties to coordinate care between members and providers, and monitor hospital admissions and readmissions to decrease fragmentation of care and reduce health care costs. BEHP's health management program focuses primarily on providing support to patients with diabetes, coronary heart disease (CAD), chronic back pain, asthma/chronic obstructive pulmonary disease (COPD), and congestive heart failure (CHF). Over the study period, BEHP provided health insurance coverage to approximately 30,000 individuals annually. The Beaumont Health System Research Institute Human Investigation Committee provided approval for this investigation (HIC# 2014-051).
To determine MCC prevalence, chronic conditions were identified using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes as defined by Office of the Assistant Secretary for Health at HHS. 21 ICD-9-CM codes were used to identify the following 20 chronic conditions in the claims data: hypertension, CHF, CAD, cardiac arrhythmias, hyperlipidemia, stroke, arthritis, asthma, autism spectrum disorder, cancer, chronic kidney disease, COPD, dementia (including Alzheimer's and other senile dementias), depression, diabetes, hepatitis, human immunodeficiency virus (HIV), osteoporosis, schizophrenia, and substance abuse disorders (drugs and alcohol). The study also used ICD-9-CM codes to identify chronic back pain (724.4; thoracic or lumbosacral neuritis or radiculitis, unspecified) and backache, unspecified (724.5) for the analysis. Primary and secondary diagnosis codes were considered when identifying chronic conditions. Subsequently, patients were categorized into different chronic condition categories for descriptive purposes: zero chronic conditions, 1 chronic condition, and 2 or more chronic conditions (ie, MCCs).
In addition to investigating MCC prevalence, the study team examined the outpatient cost, number of visits, and the number of days between appointments associated with MCC patients. Cost was defined as the total dollar amount paid by BEHP for each patient over the study period. Outpatient cost, visits, and days between appointments were calculated at the patient level using all insurance claims processed for each patient, regardless of the primary or secondary diagnoses listed on these claims.
Statistical analysis
The study team determined the number of BEHP patients who fell into each chronic condition category, as well as the number of individuals falling into groups of increasing numbers of chronic conditions (eg, 1, 2, 3, 4, 5, 6 chronic conditions). Average outpatient cost, visits, and days between appointments were then calculated for each chronic condition category for each year of the study. The team examined the crude and adjusted relationship between MCCs and outpatient cost, visit frequency, and days between appointments using linear regression. Adjusted analyses controlled for patient age and sex. Using the year 2008 as a reference, odds ratios for MCC occurrence were calculated for each year of the study period using multiple logistic regression, adjusted for age and sex.
Lastly, an analysis was conducted at the level of unique chronic condition combinations. A unique identifier was assigned to patients with the same disease constellation and these identifiers were used to evaluate the prevalence of specific chronic condition combinations, as well as the association between these combinations and outpatient cost, visits, and days between appointments. For example, patients with hypertension, hyperlipidemia, and diabetes were assigned one unique identifier, while patients with hypertension and COPD were assigned another. In this manner the study team was able to determine the top 10 chronic condition combinations in terms of prevalence and cost. All possible permutations of chronic condition combinations were considered in this particular analysis, including 1-way combinations (eg, diabetes only). To align the results with similar studies, the study team also calculated the most prevalent 1-way, 2-way, 3-way, and 4-way chronic condition combinations. Prior to all analyses, extreme outliers (n=25) and patients missing demographic information (n=67) were omitted from the study sample.
Results
From 2008 to 2013, 34,190 different adult patients of BEHP received outpatient care. Average patient age for these individuals was 40.4 (SD±13.8) years old and 61.3% (n=20,983) of this population was female. Looking at all years of the study, 33.1% (n=11,331) of patients were found to have MCCs (2 or more chronic conditions), while 23.8% (n=8145) had 1 chronic condition, and 43% (n=14,714) had no chronic conditions. Patients with up to 11 co-occurring chronic conditions were identified.
Patient characteristics did not change substantially over the study period (Table 1). The proportion of BEHP patients with MCCs decreased from 2008 to 2013, from 19.6% to 18.8%. The number of patients with only 1 chronic condition also decreased during the study period (25.3% to 24.3%). Despite declining rates of MCC prevalence, outpatient cost and utilization associated with MCC patients were found to increase. From 2008 to 2013, the average cost ($463.3 to $966.8) and number of visits (8.5 to 14.6 visits) associated with MCC patients increased 2-fold, while average length between appointments decreased approximately 2-fold (57.5 to 32.6 days) (Table 2). The bulk of the temporal change in outpatient cost and utilization occurred in the last 2 years of the study, 2012 and 2013. Through all years of the study, average cost and number of visits was significantly higher for patients with MCCs compared to those with 1 or no chronic conditions. Similarly, the number of days between appointments was consistently found to be lower for MCC patients (Table 2). In a subgroup analysis comparing males to females, females were more likely to have MCCs, but both sexes experienced similar patterns of MCC prevalence and associated cost increase over time. When looking at different age groups, all age groups experienced similar patterns of MCC prevalence and associated cost over the study period, with the exception of patients 45–64 years of age. Patients in this cohort were more likely to have MCCs and experienced the largest increase in cost during the study period compared to all other age groups. (Data not shown but available on request.)
SD, standard deviation
SD, standard deviation
Linear regression analysis revealed that greater numbers of chronic conditions significantly predicted outpatient cost (β=571.7, P<0.001), visit frequency (β=9.4, P<0.001), and days between appointments (β = −21.6, P<0.001) in models adjusted for patient sex and age (Table 3). Using logistic regression, the adjusted odds of MCC occurrence in 2013 compared to 2008 were 0.86 (95% CI: 0.82–0.92), which aligned with the temporal analysis results. The adjusted odds of MCC occurrence in 2013 compared to 2008 were found to decrease among patient sex and age groups (Table 4).
CI, confidence interval
CI, confidence interval; OR, odds ratio
In the chronic condition combinations analysis, 1560 unique disease constellations were found among BEHP patients receiving outpatient care. As can be seen in Figure 1, 50% of the BEHP's total outpatient cost can be associated with 33% of patients with one of the 24th to 1560th least common chronic condition combinations. In other words, there is a long tail distribution of BEHP patients with low-prevalence, unique chronic condition combinations associated with a significant percentage of BEHP cost. The most prevalent disease constellation in this analysis was hyperlipidemia (n=1795), a 1-way combination, while the most costly disease constellation was hypertension-hyperlipidemia ($1,496,987), a 2-way combination. The top 10 chronic condition combinations in terms of prevalence and cost are displayed in Table 5.
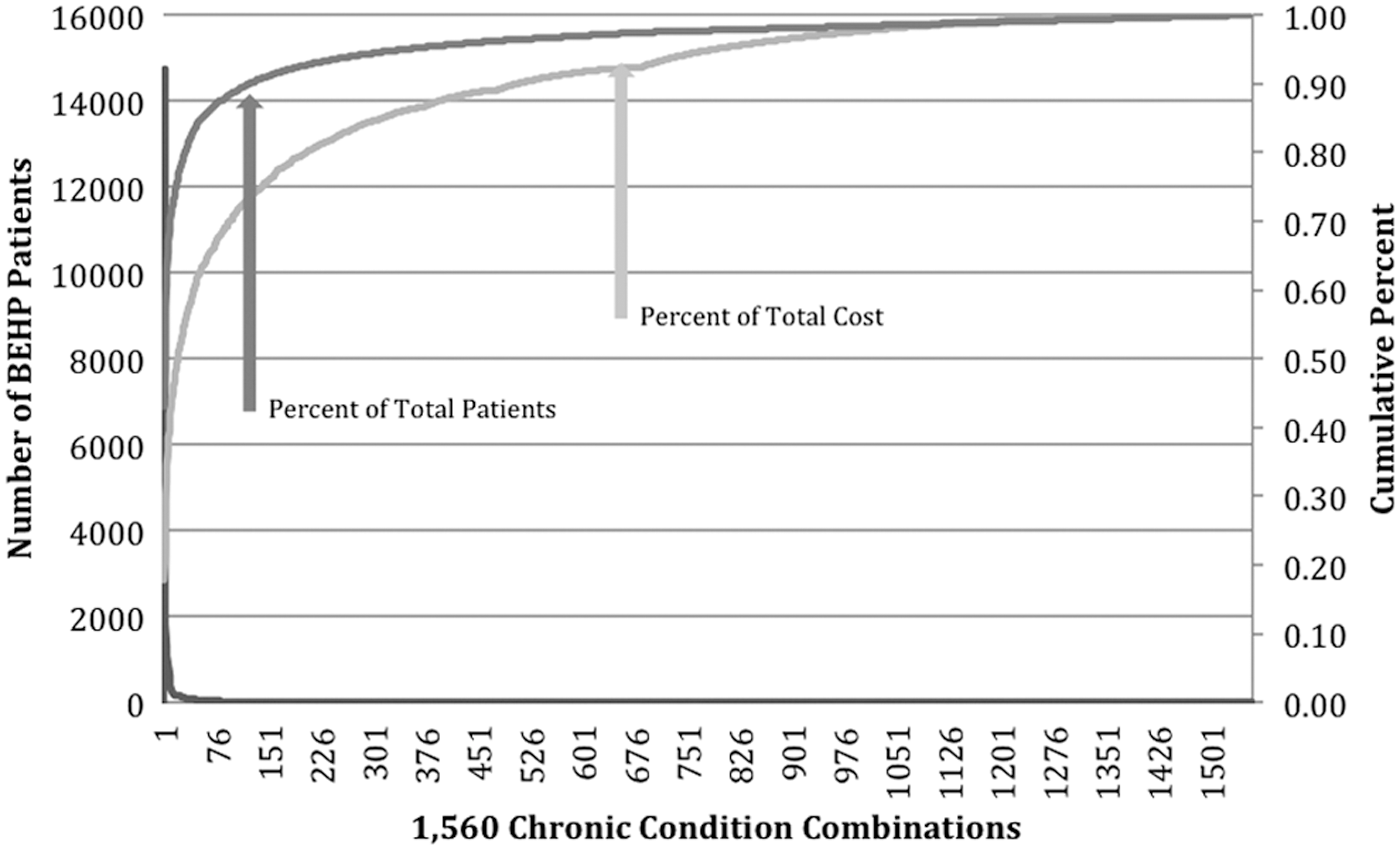
Pareto chart displaying the number of Beaumont Employee Health Plan patients with unique chronic condition combinations vs. cumulative percent of total outpatient cost and patients.
Discussion
This analysis of adult patients of an employer-based health plan found that patients with MCCs were associated with increased outpatient cost and visits, as well as decreased time between appointments. An additional outpatient cost of almost $600 dollars was found for each chronic condition a patient had. In other words, a patient with 3 chronic conditions would be expected to be associated with an additional $1800 worth of outpatient cost. Similarly, an additional 9 outpatient visits and 21 fewer days between appointments were found for each chronic condition an individual had, highlighting the immense time and coordination burden experienced by MCC patients in this population. Over the study period, average outpatient cost and number of visits associated with MCC patients increased 2-fold, while average length between appointments decreased 2-fold. During this same time period, however, the odds of patients having MCCs decreased significantly. Thus, despite MCC prevalence declining over the study period, the impact of MCC patients on health care cost and utilization increased dramatically over time. The study team also identified the top 10 chronic condition combinations in terms of cost and prevalence. The team found that a significant proportion of outpatient cost and utilization can be associated with low-prevalence MCCs. These findings demonstrate the immense opportunity that exists to study, prevent, and manage MCCs among adult patients of employer-based health plans.
In 2011, Naessens and colleagues reported the results of an investigation examining MCC prevalence and associated cost among working-age adults enrolled in a self-funded health plan. Similar to the results of the present study, they found that MCCs are a great concern for younger and healthier populations, as more than 54% of their patients were found to have MCCs. 6 The mean annual cost per person, which was comprised of inpatient, pharmacy, and physician services costs, was $300 higher for patients with 4 chronic conditions compared to patients with no chronic conditions ($1700 to $2000). 6 Unlike Naessens and colleagues, only one third of the present study population was found to have MCCs. This can be explained by the focus on the outpatient setting compared to the inpatient setting, in which MCCs are more prevalent and costly. 5,8,22 Despite the focus on the outpatient setting, the mean annual cost per patient was $360 higher for patients with MCCs compared to those without chronic conditions ($205 to $565). Prior research also has demonstrated that MCC patients are associated with an increased number of outpatient visits. The estimates in the present study far exceed the numbers previously reported. Glynn and colleagues found that MCC patients experience 2 to 3 outpatient visits per year on average. 9 The present study found that MCC patients have anywhere from 9 to 15 visits per year on average. These findings indicate that a patient with 3 MCCs will have 18 more appointments and 63 fewer days between appointments compared to a patient without MCCs.
Surprisingly, MCC prevalence decreased over the study period. It has been well documented that the prevalence of MCCs is increasing in the United States and around the world. 2,3,23 The study team anticipates that the declining MCC prevalence estimates that were observed were a direct result of employee transitions, layoffs, retirements, and enrollment in other types of insurance (eg, Medicare) over the study period, which may have adversely impacted older individuals who are at greater risk for being ill and having chronic conditions. Regardless of the reasons, however, an important takeaway from this analysis is that despite declining MCC prevalence, health care cost and utilization associated with MCC patients increased. In other words, although MCC patients dropped out of the sample, MCC patients entering into the population or remaining in the cohort became significantly more costly over time. It is important to note that the increases in utilization and cost, particularly in the last 2 years of the study, were not explained by changing patient demographics (eg, increasing average age). Although only speculative at this time, part of the observed rise may be explained by the increasing effectiveness of BEHP's health management program to ensure that chronic condition patients receive all of the care that they require. If true, this suggests that disease management programs may increase health care visits and cost for MCC patients, at least in the outpatient setting and in the short term. Future research is needed to determine whether increased outpatient utilization results in back-end savings in the inpatient and emergency department settings for this population.
Epidemiological investigations into MCC prevalence at the national level have highlighted the significant role that hypertension, hyperlipidemia, and diabetes play as single or co-occurring chronic conditions. 10,23 –25 Similar to these studies, hypertension and hyperlipidemia occurring alone or together were highly prevalent and costly in the present study. Diabetes was found to be prevalent, but not very costly. Unlike prior investigations, asthma and chronic back pain ranked 4th and 5th in the chronic condition combinations analysis, respectively. These findings speak to the need to study MCCs at a more local or regional level, where population-specific MCCs can be identified for meaningful intervention and management. For example, the high rate of asthma observed in this study may be explained by the underlying prevalence of this condition in metropolitan Detroit. 26 Likewise the high rate of chronic back pain may be related to the large number of clinical employees captured in the cohort, who are known to be at increased risk for developing work-related musculoskeletal disabilities. 27
BEHP has had a disease management program in place for asthma patients since the beginning of 2013. Initial reports indicate that this program has resulted in an increased number of office visits for patients. Potential cost savings in the inpatient and emergency department settings as a result of this program have yet to be evaluated, but are anticipated. Studies have demonstrated the reductions in cost and utilization (eg, emergency department visits), as well as improvements in patient outcomes, that can be achieved through asthma disease management programs. 28 –30 Positive return on investment for asthma programs also has been demonstrated. 31,32 However, it is important to note that these findings have not been universal. Other studies have shown that asthma disease management programs often operate at a loss. 33 Overall, evidence supporting the adoption of asthma disease management programs by employer-based health plans is mixed at this time. Online tools, such as the Agency for Healthcare Research and Quality's Asthma Return-on-Investment Calculator, are available to health plan medial directors to help guide their decision making on this matter. 34
In 2014, BEHP established a multidisciplinary disease management program for patients with chronic back pain. It is well known that the overall economic, medical, and personal cost of chronic back pain is immense. 35,36 Unfortunately, wide variation exists in the care and treatment of patients with chronic back pain in the United States. When compared to other types of clinicians, primary care practitioners are known to deliver less expensive care with comparable patient outcomes. 37 However, the value of comprehensive disease management programs for patients with chronic back pain have not been well described in the literature to date.
When comparing BEHP's costliest and most prevalent chronic conditions (Table 5) to diseases actively managed by other employer-serving health plans, such as Blue Cross Blue Shield of Michigan and Health Alliance Plan, a great deal of homology can be observed (eg, hypertension, hyperlipidemia). 38,39 However, differences do exist (eg, osteoporosis, migraines) and likely represent the unique needs of the different patient populations that are served by these health plans. In comparison to the Veteran's Health Administration, BEHP observes drastically different chronic conditions among its patients. The top chronic conditions in terms of cost among veterans include dementia, renal failure, lung cancer, and spinal cord injury. 5 Many of these conditions are uniquely prevalent in this population. Additionally, although similarities can be observed between chronic conditions among Medicare and BEHP patients (eg, hypertension, hyperlipidemia), the order of importance of these conditions differs. For example, in terms of cost, diabetes was found to be less important for BEHP compared to Medicare, while asthma and chronic back pain were more important. 40 These differences likely are driven by the fact that BEHP's patient population is younger (average age 40 years), primarily female (61%), and at increased risk for environmental (eg, air pollution concerns in Michigan) and occupational (eg, health care workers lifting patients) exposures associated with certain chronic conditions.
Despite the importance of identifying the top MCCs in terms of prevalence and health care cost and utilization, there is growing emphasis on the importance of approaching chronic disease burden from a wider perspective. 17,41 –43 There are many unique constellations of MCCs, all of which will require tailored treatment and disease management guidelines. A recent study of approximately 32 million Medicare beneficiaries found more than 2 million unique combinations of MCCs. As described by Sorace and colleagues, the distribution of constellations of MCCs results in a curve with a very “long tail” of complex patients that changes nationally over time. 44,45 More than 79% of Medicare expenditures can be associated with patients with unique, low-prevalence MCCs belonging to this “long tail.” 44 The study team conducted a similar analysis looking at all the different permutations of chronic conditions in the employer-based health plan population. The team found 1560 unique disease constellations.
Similar to Sorace and colleagues, the team discovered a “long tail” distribution of BEHP patients with low-prevalence, unique chronic condition combinations associated with a significant percentage of BEHP cost. Fifty percent of the BEHP's total outpatient cost was found to be associated with 33% of patients with 1 of the 24th to 1560th least common chronic condition combinations. These results indicate the importance of not only intervening with patients with highly prevalent and costly MCCs, but also intervening with patients with low-prevalence MCCs who are attributable to a large percentage of total cost. Employer-based health plans that focus only on the “top 10” chronic condition combinations in terms of cost or prevalence may not be able to adequately control costs associated with MCC patients.
Employer-based health plans have historically been mainstays in the development of chronic disease management programs. 46 As the burden of MCC patients increases on the US health care system over time, significant opportunity exists for employer-based health plans to be leaders in engineering innovative care coordination and disease management practices, and supporting the development of multifaceted treatment guidelines for MCC patients. However, the first steps to achieving these goals are for health plans to characterize their MCC populations and understand these patients' experiences with health care quality, cost, and utilization. Based on the results of this analysis, BEHP is expanding their “chronic conditions of interest list” to include additional conditions for disease management, and is determining how to cast a wider net to support patients with unique chronic condition combinations (the long tail), who are not currently being adequately tracked or supported.
The strengths of this study are the large sample size and that a standardized approach was used to identify chronic conditions to improve comparability of results across investigations. In addition, both employees and their dependents were included in the analysis, meaning that anyone from physicians and their spouses to security officers or clerks and their immediate adult family members were captured. By doing so the study team was able to capture a more diverse patient population to improve the generalizability of the results.
This study has several important limitations. Health system employees and their dependents are known to experience higher health care costs, a larger number of hospital admissions, and somewhat greater chronic disease burden compared to the general US population. 47 This may result in overestimation of outcome measures, particularly in terms of outpatient utilization and cost, as well as the prevalence of MCCs when trying to apply these results to other patient populations. In other words, the generalizability of these results may be limited to employer-based health plans serving employees and dependents of hospitals and health systems only. ICD-9-CM codes were used to identify chronic conditions. Diagnosis validity could have been improved if the study team had additional clinical or laboratory data to identify conditions or cross-check billing codes. In addition, the estimates may underrepresent the true burden of MCCs among these patients given that the analysis was limited to the outpatient setting. Because many patients are lost during follow-up care, the study team may have missed diagnoses that occurred in the inpatient setting, but were never noted in the outpatient setting. In addition, the team did not capture ancillary costs such as medical equipment or medications.
In summary, among adult patients of an employer-based health plan, this study found that MCCs are associated with increased cost and visits, as well as decreased time between appointments in the outpatient setting. Despite decreasing prevalence of MCCs over the study period, substantial increases in cost and visits, as well a decrease in time between appointments was observed for MCC patients. Asthma and chronic back pain were uniquely identified as additional primary targets for disease management programs for employer-based health plans. Many similarities can be observed between health plans in terms of chronic conditions that are highly prevalent and costly. However, important differences exist and likely are driven by underlying patient population characteristics. These findings speak to the value of studying MCCs at the employer-based health plan level, where population-specific MCCs can be identified for meaningful intervention and management. Significant opportunity exists for employer-based health plans to study, prevent, and manage MCCs among adult patients.
Footnotes
Author Disclosure Statement
Mr. Rezaee and Dr. Pollock declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for the research, authorship, and/or publication of this article.