
Abstract
In 2008, Kaiser Permanente Northwest identified the transition from hospital to home as a pivotal quality improvement opportunity and used multiple patient-centered data collection methods to identify unmet needs contributing to preventable readmissions. A transitional care bundle that crosses care settings and organizational functions was developed to meet needs expressed by patients. It comprises 5 elements: risk stratification, a specialized phone number for discharged patients, timely postdischarge follow-up, standardized patient discharge instructions and same-day discharge summaries, and pharmacist-supported medication reconciliation. The transitional care bundle has been in place for 6 years. Readmission rates decreased from 12.1% to 10.6%, Hospital Consumer Assessment of Healthcare Providers and Systems scores for the discharge instruction composite moved from below the 50th to above the 90th national percentile, average time to the first postdischarge appointment decreased from 9.7 days to 5.3 days, and error rates on the discharge medication list decreased from 57% to 21% (P<.0001 for all). The program, which continues to evolve to address sustainability challenges and organizational initiatives, suggests the potential of a multicomponent, patient-centered care bundle to address the complex, interrelated drivers of preventable readmissions. (Population Health Management 2016;19:56–62)
Introduction
R
Although the true proportion of avoidable readmissions is unknown, evidence is emerging about effective prevention strategies. A recent meta-analysis concluded that multifaceted interventions that address contextual issues and limitations in patients' capacity for self-care are most effective. 10 Trials included a median of 4 transitional care activities; 63% were provided by a single provider, most often a nurse, and 2 were multidisciplinary. 10 Although many trials targeted specific populations (eg, individuals with heart failure), few used multiple risk factors for readmission to stratify patients. 11 In addition, although many interventions focused on patients' needs, to the best of the research team's knowledge, only 1 was developed with substantial input from patients and caregivers; none included patients or caregivers in program design, implementation, and monitoring. 12 –15
In 2009, Kaiser Permanente Northwest (KPNW) developed a patient-centered bundle of multidisciplinary interventions crossing inpatient, home, and ambulatory care settings to support patients during the hospital-to-home transition. Developed and maintained with input and oversight from patients and caregivers, the bundle has been applied for 6 years by cross-functional teams on a risk-stratified basis. This article describes the development, implementation, and refinement of the transitional care bundle and its effect on readmission rates, patient satisfaction, time to follow-up care after discharge, and discharge medication list errors.
Methods
Setting
KPNW is one of 7 regions of the nation's largest not-for-profit integrated care delivery system. Nearly 500,000 members receive care from approximately 900 physicians and 9000 employees at 27 outpatient medical office buildings, 2 KPNW medical centers, and several community hospitals with contracts to provide care to local members. A comprehensive electronic health record (EHR), KP HealthConnect, is integrated across all KPNW care settings.
Developing the transition bundle
In 2008, KPNW identified care transitions as a pivotal quality improvement opportunity. To understand the challenges patients and caregivers face during the hospital-to-home transition, the research team collected data using a variety of methods, including patient interviews, video ethnography, and a readmission diagnostic tool adapted from the Institute for Healthcare Improvement that included a chart review and additional interviews with patients, family members, and care team members. 16,17 Engaging patients and family members provided a meaningful patient-centered perspective that was augmented when a health plan member of many years—a professional engineer experienced at quality systems improvement—joined the working group after approaching KPNW leadership and offering to help improve transitional care.
Interviews with and observations of patients and caregivers revealed 5 needs during the hospital-to-home transition that, if unmet, could lead to readmission. As patients expressed them: • I will have what I need when I return home. • I know when I should call and what number to use when I need help. • My regular doctor will know what happened to me in the hospital. • I will see my doctor soon after my hospitalization, and I know someone will check on me when I am home. • I understand my medications, how to take them, and why I need them.
Interviews and observations in the hospital with physicians, nurses, and patients yielded important learnings. No systematic process existed to identify patients' postdischarge needs, patients perceived care as neither coordinated nor patient-centered, and the hospital was a suboptimal setting for learning about postdischarge care, particularly medications. Patients and caregivers were often so focused on getting home that they had difficulty distinguishing between continuing medications they had on hand and new ones they needed to obtain. More generally, patients' and caregivers' distraction on discharge day made it difficult for them to foresee potential needs at home.
Administrative data supported findings from the readmission diagnostics, observations, and interviews. An average of 9.7 days elapsed between discharge and a first appointment with a primary care provider (PCP). Discrepancies were common between medications on the discharge list and those that patients took at home; 57% of discharge medication lists contained at least 1 error. Patient satisfaction, measured by the composite Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) discharge information composite score, was just above the 75th national percentile.
Thus, the goal of the improvement project was to create an integrated bundle of interventions to keep patients safely at home after discharge. Specific objectives were to reduce 30-day readmission rates from a 2008 baseline of 12.1% to 10%, improve patient satisfaction, reduce the time to first postdischarge appointment, and reduce discharge medication errors.
Developing the transition bundle
Transition bundle elements were developed over 3 months. Kaiser Permanente's Care Management Institute, which was working program wide to identify factors affecting transitions, helped KPNW select physician and health plan leaders for the transitions work and convene stakeholders: a health plan member and physicians, nurses, and other staff across settings (hospital, clinic, home health, skilled nursing facilities), and pharmacy, case management, and quality departments. A PCP survey identified a key issue; they did not receive timely discharge information from the hospital or, sometimes, even notification that patients were hospitalized.
Stakeholder groups began developing potential strategies to address the patient needs identified, based on published evidence and internal and external best practices. Doing so required breaking down silos between settings and stakeholder groups. For example, with leadership support and encouragement, hospitalists and PCPs worked together to improve information transfer from inpatient to ambulatory care settings. Over 6 months, more than 50 Plan-Do-Study-Act cycles were completed; the results were reviewed in weekly meetings of 8–20 stakeholders, yielding the bundle elements.
The transition bundle
All patients received a bundle of interventions: stratification into high, medium, and low risk for readmission; a specialized phone number; standardized same-day discharge summaries and instructions; timely follow-up; and medication reconciliation. Additional care components were added to follow-up and medication reconciliation according to readmission risk. For example, high-risk patients received earlier follow-up appointments, ongoing care coordination, and pharmacist medication reconciliation support.
All bundle elements were delivered by nursing and pharmacy staff and hospitalist physicians. For instance, on admission, nurses and physicians discussed with patients how they took their medications at home. Before discharge, nurses provided discharge education and the unit secretary discussed feasible appointment times with patients and caregivers. The number of contacts increased for patients at high risk of readmission; after discharge, a transitions nurse and pharmacist telephoned high-risk patients and their caregivers at home.
Risk stratification addressed the first patient-expressed need: to have what they needed when they returned home. Risk stratification of all patients admitted allowed tailoring of care to the special needs of those at high risk for readmission. Initial high-risk criteria included any diagnosis of heart failure, whether or not it was related to the admission, or an admission within the previous 30 days. In addition, any nurse, physician, or pharmacist could identify high-risk patients who did not meet the first 2 criteria.
A specialized phone number for discharged patients addressed their need to know what number to use to obtain help. A “post-hospital (telephone) hotline” ensured that patients had a single point of contact between discharge and the first follow-up appointment. Calls were transferred to a priority nurse advice line and triaged 24 hours/day, 7 days/week. Advice nurses handled the calls they could and paged an on-call hospitalist or specialist for the balance. An important part of the supporting infrastructure was an agreement brokered by leadership between hospitalists and PCPs, in which hospitalists' oversight and responsibility for patient care was extended to 48 hours after discharge, transferring to patients' PCPs thereafter.
Standardized same-day discharge summaries and instructions addressed patients' needs for their regular doctor to know what happened to them in the hospital and to know when to call for help. Standardized discharge summaries included an assessment of readmission risk and identification of pending studies and issues requiring attention at follow-up appointments (Fig. 1). Standardized patient discharge instructions included discharge diagnosis (in layman's terms), diet, activity, “call if/return if” instructions specifying signs and symptoms warranting a phone call to a physician or nurse, the hotline phone number, follow-up tests and appointments, and any additional instructions.

Example template for standardized discharge summary. IP, inpatient; H&P, history and physical; KPNW, Kaiser Permanente Northwest; OR, operating room; PVD, peripheral vascular disease; SIRS, systemic inflammatory response syndrome.
Timely post-hospital follow-up addressed patients' needs to see their doctor soon after hospital discharge and to know that someone would check on them after they returned home. All ambulatory care appointments were made before discharge and listed on the patient's discharge summary. Follow-up appointments occurred within 5 days for high-risk patients and within 10 days for all others. Transition registered nurses (RNs) followed up with patients by phone within 48 hours and provided case management services to high-risk patients for 30 days.
Medication reconciliation interventions addressed patients' needs to understand their medications, how to take them, and why they were needed. All patients received medication review and reconciliation at admission and an accurate medication list with instructions in lay language on discharge. Transition care pharmacists prioritized very high-risk patients for medication reconciliation at discharge, based on age, medications, and chronic conditions. After discharge, transition RNs reviewed medications during 1 or more follow-up phone calls. In some cases, determined in partnership with a transition RN, pharmacists provided outreach calls.
Implementation and oversight
The transition care bundle was implemented for inpatients on the internal medicine service in 2009 in one 269-bed KPNW medical center, using existing staff and resources and an additional 2.0 transition pharmacist full-time employees. It was expanded to inpatients on medical and surgical specialty services in late 2010, and the research team began tracking aggregated outcomes for all inpatient services on a rolling basis as each implemented the bundle. Specialty departments developed standardized discharge summaries and patient instructions tailored to their patients' needs and provided follow-up phone calls and appointments within risk-specified time frames.
Weekly stakeholder meetings, which continued to include a health plan member, provided program oversight; providers retained clinical reporting relationships. In addition to tracking outcome measures, oversight included ongoing physician review of all 30-day readmissions to determine preventability as an indicator of the need to implement additional strategies, identify the accountable service and physician, and note recurring themes. Primary and specialty care department chiefs received a monthly readmission report and shared the findings with their colleagues.
Outcome measures
The research team measured readmission rates over time:

Index discharges included all acute inpatient discharges during the measurement period for KPNW members, excluding: • deaths during the admission; • transfers to another acute inpatient facility (eg, for an interventional procedure, to a specialty facility such as a psychiatric hospital); • non-inpatient stays (eg, outpatient surgery, observation); • discharges from rehabilitation, psychiatric, and detox units, skilled nursing facilities, and long-term acute care facilities; • discharges of patients leaving against medical advice; • normal newborn discharges; and • discharges of members who disenrolled in the subsequent 30 days.
In 2011, Healthcare Data Effectiveness and Information Set measures incorporated a risk-adjusted ratio of observed to expected (O/E) 30-day readmissions, which the research team began tracking. To measure patient satisfaction, the team used the HCAHPS discharge information composite, consisting of 2 items with yes/no response options: (1) Did doctors, nurses, or other hospital staff talk with you about whether you would have the help you needed when you left the hospital? (2) During your hospital stay, did you get information in writing about what symptoms or health problems to look out for after you left the hospital? In 2013, HCAHPS added a care transitions composite measure including 3 items scored using a 5-point Likert scale (1=strongly disagree to 5=don't know/don't remember/not applicable) response: (1) The hospital staff took my preferences and those of my family or caregiver into account in deciding what my health care needs would be when I left the hospital; (2) When I left the hospital I had a good understanding of the things I was responsible for in managing my health; and (3) When I left the hospital, I clearly understood the purpose for taking each of my medications. The research team also tracked the time to first postdischarge follow-up appointment and the proportion of discharge medication lists containing errors.
Results
Between 2011 and 2013, an average of 18,488 patients were discharged annually. In 2013, their mean age was 54.9, and 60% were female. In 2013, the prevalence of discharge diagnoses of congestive heart failure, acute myocardial infarction, and pneumonia among discharged patients was 6.4%, 6.3%, and 3.0%, respectively. The case mix index (CMI) increased from 1.58 in 2010 to 1.72 in early 2014.
In April 2014, approximately 50% of all patients discharged to home were at high risk for readmission; 68% of these patients had an appointment within 5 days and 56% had pharmacist medication reconciliation.
Readmission rates and O/E ratios
Between 2008 and April 2014, the readmission rate decreased from 12.1% to 10.6%. Combined (Medicare and commercial) O/E ratios decreased between 2011 and the first quarter of 2014 from 0.71 to 0.66, moving from between the 75th and 90th percentiles to under the 90th percentile (Fig. 2). Both decreases were statistically significant (P<.0001).
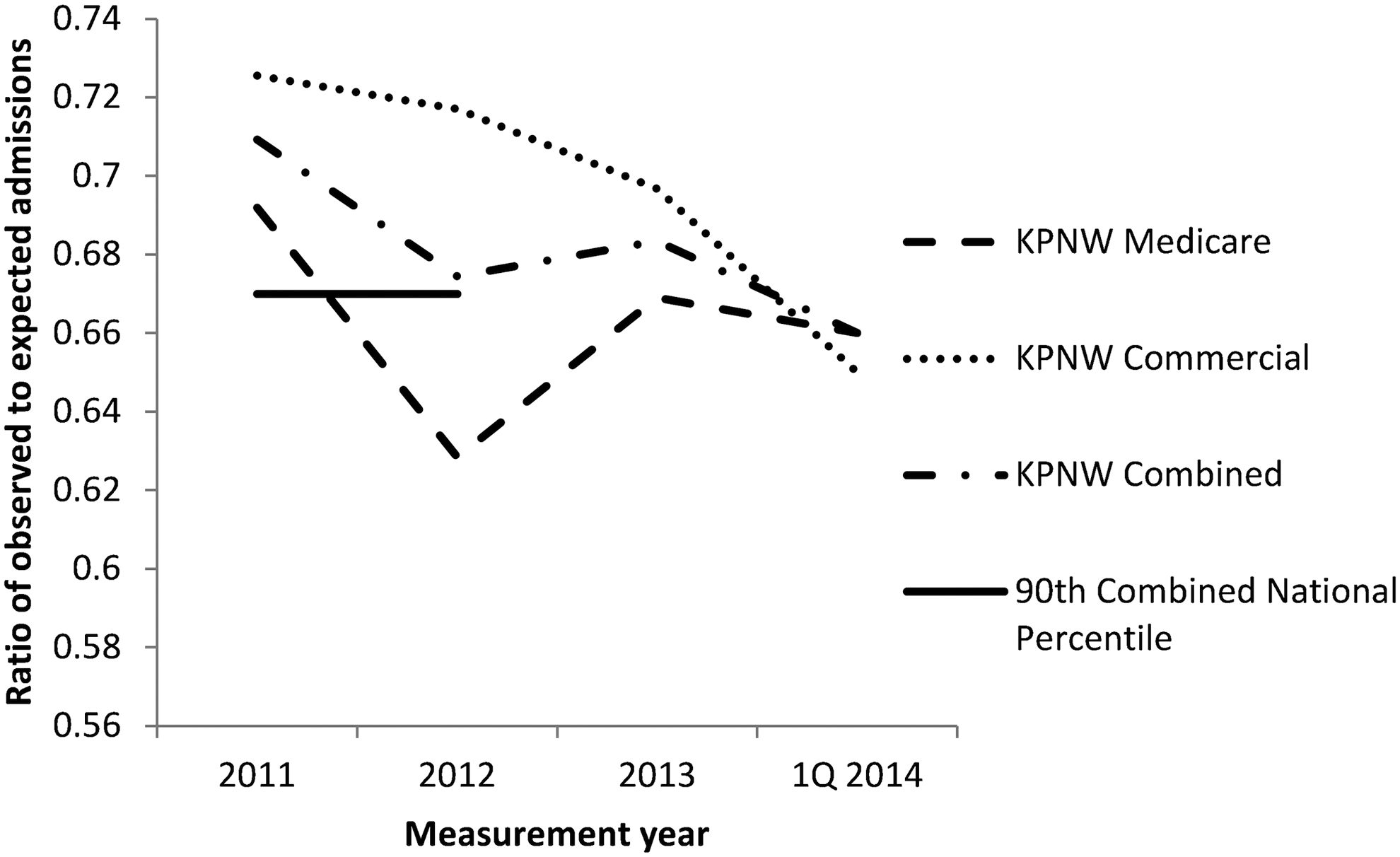
HEDIS observed/expected readmission ratios over time. HEDIS, Healthcare Effectiveness Data and Information Set; KPNW, Kaiser Permanente Northwest.
Patient satisfaction
Between 2008 and April 2014, HCAHPS discharge instruction composite scores increased from 80% to 90.9% (P<.0001), moving from below the 50th national percentile to above the 90th percentile (Fig. 3). The 2013 care transition measure score was 58.3%, just under the 90th national percentile in the first year the measure was used nationally.
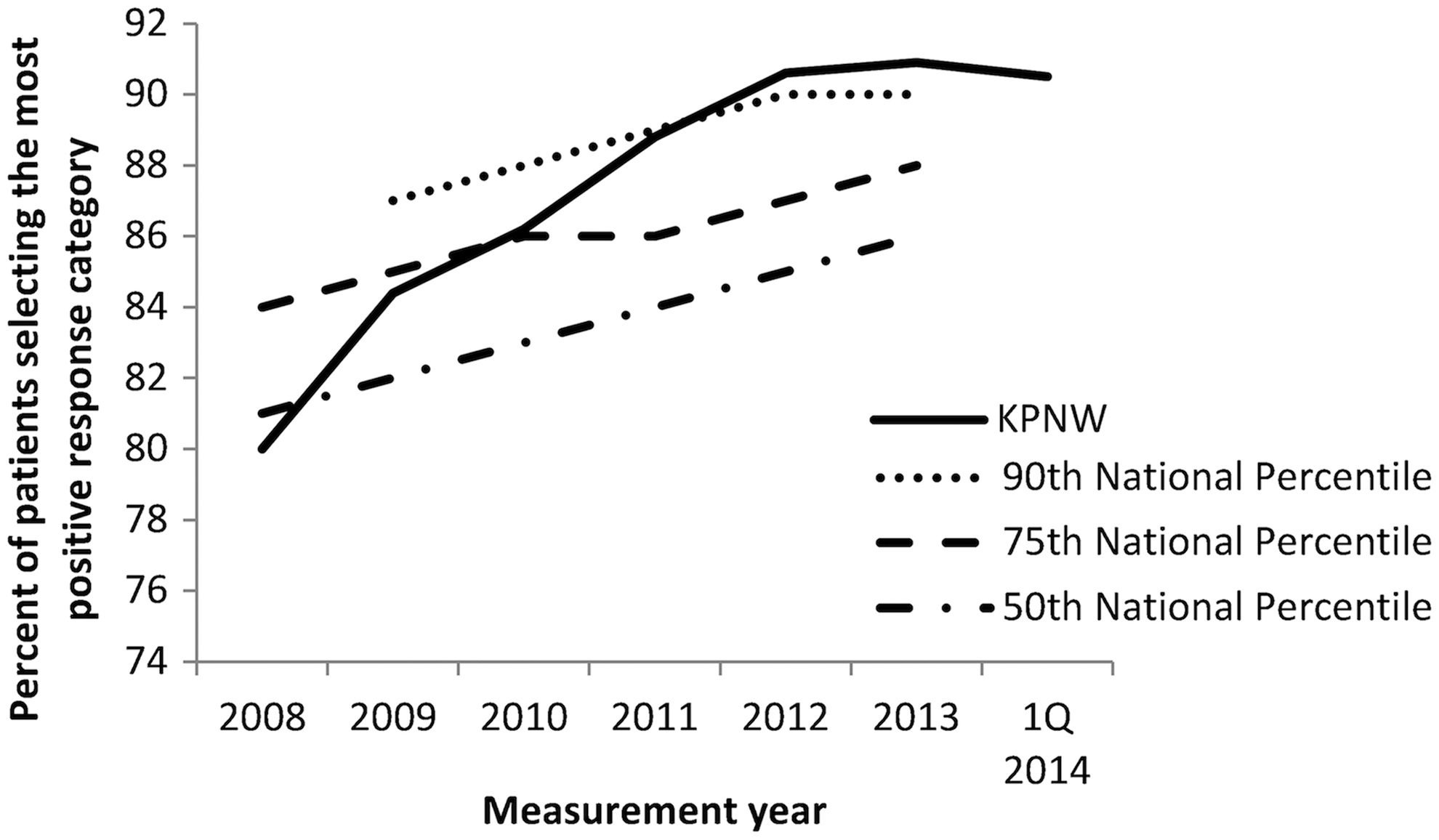
Scores on HCAHPS discharge information composite over time. HCAHPS, Hospital Consumer Assessment of Healthcare Providers and Systems; KPNW, Kaiser Permanente Northwest; Q, quarter.
Time to first follow-up appointment with PCP
Between December 2008 and April 2014, the average time between hospital discharge and the first follow-up appointment for high-risk patients on the internal medicine service decreased from 9.9 days to 5.3 days (P<.0001).
Discharge medication list errors
Errors on the discharge medication list decreased from a baseline of 57% to 21% in April 2014 (P<.0001). Most errors are detected and corrected before discharge by the pharmacist performing medication reconciliation.
Discussion
A transition bundle was associated with reduced readmission rates and O/E ratios, increased patient satisfaction, earlier follow-up after discharge, and fewer errors on discharge medication lists. Strengths of this report include the focus on patient experiences of the hospital-to-home transition, the length of time over which results have been sustained, and the use of multiple evidence-based strategies to address the complex challenge of reducing readmissions.
Limitations include a pre/post observational report and limited data regarding patient characteristics; however, readmission rates decreased as the CMI increased. The transitional care bundle was implemented in the context of an integrated EHR that facilitated some communication and reporting, and generalizability to settings without this capacity is unknown. The bundle did not reach 100% implementation during the period reported here, rendering the results a conservative estimate of its potential effect. It was implemented within a complex health care delivery system with multiple quality goals and initiatives; the reported improvements may not be due solely to the transition bundle, although no other quality programs focused on the hospital-to-home transition. Finally, the research team can make no assertions about the effectiveness of individual bundle components. In the team's experience, all are required to manage complex care pathways across settings.
The transitions bundle combines elements used elsewhere to varying degrees. Pharmacist or nurse medication reconciliation is frequently reported in multicomponent interventions to reduce readmissions. 11 –13,15,18 –20 A risk assessment component is reported less frequently, as are follow-up with a physician within 5 days and arranging follow-up appointments before discharge. 19,21 –24 Among 537 hospitals surveyed, 22% formally estimated the risk of readmission and 11% arranged follow-up appointments before discharge. 25 In contrast, 59% of hospitals provided a designated telephone number for patients to reach a physician in an emergency. 25
The transitions bundle was subsequently adopted by all Kaiser Permanente regions with similar results. 26 It has also evolved in KPNW to address emerging challenges and quality initiatives. For example, inpatient providers sometimes missed identifying high-risk patients because they overlooked the specific criteria of a previous readmission and any diagnosis of congestive heart failure (CHF) among patients who did not otherwise seem at risk. To ensure that all high-risk patients were identified, automatic stratification methods and an EHR best practice alert (BPA) were added in 2014. The research team incorporated the LACE readmission index, using data from the EHR and clinical data warehouse and score cut points developed by Kaiser Permanente colleagues to automatically identify all patients as low (0–6), medium (7–10), or high risk (11–19) for readmission. 26,27 Similarly, an internally developed algorithm automatically segments the population of older adults into 4 care groups with similar needs, trajectories, and utilization patterns. 28 A BPA prompting the discharging physician to implement the transition bundle is triggered for patients identified as being at high risk by the LACE index or belonging to the highest need care group. A recent readmission, any diagnosis of CHF, and identification of high-risk status by care coordinators, who are accountable for identifying high-risk patients, also trigger the BPA. Although all patients receive the elements of the transition bundle, those at highest risk receive the earliest and most robust interventions after discharge, such as the earliest available PCP appointment and nurse and pharmacist telephone follow-up.
In 2012, after observing that a majority of readmissions occurred within 5 days of discharge, the research team narrowed readmission reviews to that interval. Reviews check for the activation of bundle elements and identify recurring issues, such as managing anticoagulation therapy, poor support at home, and fragile living situations. Issues identified in readmission reviews are shared with leadership to develop strategies to address them. For instance, the implementation of an inpatient palliative care team addressed end-of-life care issues contributing to preventable readmissions. Review revealed that wound infections and constipation frequently contributed to readmissions; including guidelines for wound and bowel care in specialty care-specific standardized discharge instructions reduced their impact. Finally, reviewing oncology readmissions revealed that the operating hours of the outpatient infusion clinic drove some readmissions; expanding those hours addressed this driver.
Although reluctance in specialty care departments might have posed a challenge to bundle implementation, this was not the case. Department-level readmission data garnered department chiefs' attention and support. The potential to use transition pharmacists to address medication reconciliation was a powerful motivator for finding solutions to challenges, such as departmental capacity for providing postdischarge phone calls and the development and consistent use of standardized documentation templates in physician discharge summaries.
Sustainability requires attention. In addition to readmission reviews, a dashboard of operational process metrics helps identify improvement opportunities. Transition care leaders attend meetings of hospital leaders to provide updates on transition care performance. However, numerous challenges to sustainability exist. As the program demonstrated success, the frequency of stakeholder meetings decreased from weekly to biweekly; although it is taxing for a large group of stakeholders to attend weekly meetings on an ongoing basis, more frequent meetings helped maintain a sense of urgency about the need to ameliorate readmissions.
It also has proven challenging to keep other hospital staff members who implement bundle elements, such as nurses and unit secretaries, informed about the program and its current state, limiting their investment in its success. Turnover within these categories of hospital personnel also affects sustainability. The transition bundle is incorporated into staff orientation activities to varying degrees across inpatient units; a current goal is to incorporate it into hospital orientation. Changing resource levels and staff turnover also affect consistent bundle use. Readmissions increased slightly in 2013, contemporaneously with reductions in transition RN positions related to other organizational imperatives and in the ease with which hospital staff could schedule follow-up appointments. In addition, evolving KPNW delivery systems necessitate adapting transitional care. Regional implementation of a model to provide complex care required retaining the bundle elements while incorporating the patient's care navigator as a main point of postdischarge contact and identifying and incorporating community resources.
In 2013, the transition bundle was implemented at a recently constructed KPNW hospital and at all contract hospitals. Future plans include implementing a community paramedicine program in which paramedics visit patients at home, acting as an extension of the health care team and caring for those not covered by other services such as home health or hospice. 29 Additional opportunities under consideration include transition bundles tailored to other populations (eg, patients being discharged home from a skilled nursing facility, pediatric patients, patients seen in the emergency department).
Future research is required to replicate the transition bundle in other settings. Its utility is not limited to integrated care delivery systems. Although KP HealthConnect is integrated across care settings, it did not eliminate the need to ensure that PCPs promptly received thorough discharge summaries or the need to reconcile medications. A recent report describes a bundle including similar components that was implemented in a large public teaching hospital with positive results. 21
Finally, the research team notes that the involvement of a health plan member in the development and monitoring of the transitional care bundle is essential. From the health plan member's participation, the team continues to learn that collective clinical expertise and best intentions do not guarantee the ability to understand how patients experience care. His input consistently directs the transitions team toward elements of care that are important to patients, feasible, and comprehensible. To design, implement, and maintain patient-centered programs, we must turn to patients for guidance.
Conclusion
The implementation of a patient-centered transitional care bundle to address patient-identified needs was followed by reduced readmissions, increased patient satisfaction, reduced time to the first postdischarge follow-up appointment, and reduced errors on discharge medication lists. This experience suggests that a multicomponent bundle of strategies that crosses care settings and organizational functions has the potential to address the complex issue of preventing readmissions.
Footnotes
Author Disclosure Statement
Drs. Rice, Rastogi, Steinkeler, and Ms. Barnes and Ms. Hillstrom declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
This work was funded in its entirety by Kaiser Permanente.