
Abstract
Increasing scrutiny of hospital readmission rates has spurred a wide variety of quality improvement initiatives. The Preventing Avoidable Readmissions Together (PART) initiative is a statewide quality improvement learning collaborative organized by stakeholder organizations in South Carolina. This descriptive report focused on initial interventions with hospitals. Eligible participants included all acute care hospitals plus home health organizations, nursing facilities, hospices, and other health care organizations. Measures were degree of statewide participation, curricular engagement, adoption of evidence-based improvement strategies, and readmission rate changes. Fifty-nine of 64 (92%) acute care hospitals and 9 of 10 (90%) hospital systems participated in collaborative events. Curricular engagement included: webinars and coaching calls (49/59, 83%), statewide in-person meetings (35/59, 59%), regional in-person meetings (44/59, 75%), and individualized consultations (46/59, 78%). Among 34 (58%) participating hospitals completing a survey at the completion of Year 1, respondents indicated complete implementation of multidisciplinary rounding (58%), post-discharge telephone calls (58%), and teach-back (32%), and implementation in process of high-quality transition records (52%), improved discharge summaries (45%), and timely follow-up appointments (39%). A higher proportion of hospitals had significant decreases (≥10% relative change) in all-cause readmission rates for acute myocardial infarction (55.6% vs. 30.4%, P=0.01), heart failure (54.2% vs. 31.7%, P=0.09), and chronic obstructive pulmonary disease (41.7% vs. 33.3%, P=0.83) between 2011–2013 compared to earlier (2009–2011) trends. Focus on reducing readmissions is driving numerous, sometimes competing, quality improvement initiatives. PART successfully engaged the majority of acute care facilities in one state to harmonize and accelerate adoption of evidence-based care transitions strategies. (Population Health Management 2016;19:4–10)
Introduction
T
A wide variety of national initiatives now focus on improving care transitions. For example, more than 100 Centers for Medicare & Medicaid Services (CMS)-sponsored Community-Based Care Transitions demonstration projects have been funded. 6 CMS also has stimulated care transitions work through its Partnership for Patients by engaging more than 3900 hospitals in 46 states participating in 26 Hospital Engagement Networks (HENs) nationwide. 7 Finally, CMS has sponsored care transitions quality improvement through its state-based quality improvement organizations (QIOs). 8 In addition, a myriad of state- and locally-based initiatives have arisen. 9,10
With limited resources and numerous quality measures to address beyond readmissions, individual hospitals must decide which care transitions improvement strategies to implement and which programs in which to participate. 11 –13 Outside of primarily single-center randomized controlled trials, 14 few published reports exist to guide best practices especially regarding collaboration across health care facilities and communities. 15 Additional information is needed on best practices to reduce hospital readmissions, optimal models for sponsorship of large-scale improvement efforts, and the optimal depth and scope for such initiatives. To address this gap in the literature, this article reports on the design and initial impact of a statewide quality improvement learning collaborative focused on preventing avoidable rehospitalizations.
Methods
Organizations and partnerships
In early 2012, three separate statewide programs related to care transitions were forming in South Carolina, including efforts by a statewide organization, the CMS-sponsored QIO, and several large HENs. Importantly, leaders of these 3 initiatives realized that collaboration and alignment would benefit the state more than working separately or in competition. After initial negotiations, the South Carolina Partnership for Health (SCPfH), an organization composed of the state's largest health insurance company (BlueCross BlueShield of South Carolina), a statewide health sciences research and health system improvement collaborative (Health Sciences South Carolina), and the South Carolina Hospital Association, partnered with the Carolinas Center for Medical Excellence, the CMS QIO for North and South Carolina, and the largest HEN in South Carolina. A memorandum of understanding was drafted outlining specific actions of each organization and divided duties.
Program design
The Preventing Avoidable Readmissions Together (PART) Collaborative was based on principles devised by Batalden and Berwick for Breakthrough Series Collaboratives conducted by the Institute for Healthcare Improvement (IHI). 16 A leadership team composed of representatives from member organizations and hospitals drove program design and learning topics. The SCPfH also contracted with the Society of Hospital Medicine (SHM) for additional content expertise and resources. The SHM-directed Project BOOST (Better Outcomes to Optimize Safe Transitions) is an evidence-based, multicomponent, mentored quality improvement program previously implemented by multiple hospitals to reduce readmissions. 17 PART recruitment targeted acute care hospitals and other interested organizations with a statewide announcement, through e-mail listservs, face-to-face meetings, and one-on-one connections.
PART program activities were divided into 5 distinct periods of learning, planning, and action over a 2-year time frame. After an initial statewide learning session, hospitals engaged in a 3-month planning phase dedicated to forming multidisciplinary teams, mapping hospital discharge processes, and performing root cause analyses using tools and techniques provided by PART experts. The subsequent 6-month action period focused on implementing transitional records and patient education. A second action phase focused on discharge summary timeliness and quality, and the third focused on improving timely hospital discharge follow-up appointments and post-discharge patient contact. Each subsequent phase included the addition of further care transitions strategies. Participants could select which, if any, tools and resources to implement, as well as the timing of this engagement. The continuation/consolidation period in progress has focused on the further implementation of existing evidence-based innovations, and on sustainability. In each action period, program content and consultations focused on targeting high-risk conditions for hospital readmission including acute myocardial infarction (AMI), pneumonia, congestive heart failure (CHF), and chronic obstructive pulmonary disease (COPD).
Learning activities
Webinars and group coaching teleconferences focused on topics including basic quality improvement skills, patient-centered education methods such as teach-back, 18 –21 systems design issues such as systems to ensure timely follow-up appointments, and disease-specific education strategies. In-person learning sessions included statewide meetings and regional meetings. Annual statewide meetings hosted nationally recognized care transitions experts addressing topics of broad interest. Regional meetings extended educational efforts, enabling hospitals to present their quality improvement efforts to emphasize sharing of best practices. Collaborative-based learning was reinforced with peer contacts available for informal mentoring, emphasizing regional context and knowledge. PART also sponsored a statewide e-mail listserv, and participating facilities also were granted access to a national care transitions listserv sponsored by Project BOOST. Individualized consultations with nurse and physician care transitions experts were offered by e-mail, telephone, and in-person upon request.
Resource guide
To facilitate quality improvement activities, the PART leadership team developed and freely distributed a resource guide to all interested organizations. 22 This 55-page document described the PART program and its objectives, covered key concepts for care transitions quality improvement, outlined core program components, and included a variety of data collection tools and resources. This resource guide supplemented information in the Project BOOST implementation guide, which also was provided to participants.
Progress reports
Individualized reports combining self-reported and publicly available data were provided to all hospitals. First, participating hospitals were encouraged to collect and submit data regarding process of care measures to a secure database through a Web portal developed by the collaborative. In partnership with the South Carolina Revenue and Fiscal Affairs Office (SC RFA) a report was developed with individualized hospital readmission data based on comprehensive records of emergency department (ED) visits and inpatient hospitalizations maintained by that agency. Specific readmission data included all-cause 7-day and 30-day readmission rates to the same hospital or any hospital in South Carolina, readmission rates by payer and diagnosis (ie, AMI, CHF, pneumonia, COPD), and reports of ED visit rates and observation admissions. All hospitals also were surveyed to ascertain which care transitions improvement tactics had been adopted and the stage of implementation of these projects. Readmissions data were provided biannually, and comprehensive reports were provided annually.
Outcomes analysis
As part of the program evaluation to assess preliminary impacts of the PART collaborative, the research team analyzed aggregated data compiled by the SC RFA for submission to the Healthcare Cost and Utilization Project and other purposes. This data set was derived from uniform billing claims data submitted by all South Carolina hospitals. The team analyzed unadjusted 30-day all-cause hospital readmission rates from calendar year 2011, the final full year before PART, to 2013, the first full year of PART. For comparison across time periods, rate changes from an earlier time period, 2009–2011, also were analyzed. The latter rate change analysis was restricted to facilities with ≥10% differences, which were considered to be clinically relevant.
A 2X2 McNemar test was run to test the difference between actual paired hospital proportions for hospitals with a 10% or greater improvement in readmission rates with all diagnoses. The test determined whether the 2011–2013 proportions, when the PART interventions were implemented, were significantly different from the 2009–2011 proportions of hospitals, when no interventions were implemented. A paired-sample t test also was used to compare the hospital overall means from 2 different time periods by overall cause and by hospitalization for hospitals with a 10% or greater improvement in readmission rates with all diagnoses. A percent readmission rate difference variable between 2009 and 2011 and a percent readmission rate difference variable between 2011 and 2013 were created; these 2 variables were tested to determine whether the means were significantly different from one another.
Results
Reported here are results for the first 18 months of the PART program (September 2012 to February 2014). The PART learning collaborative enjoyed broad statewide participation by a variety of organizations including hospitals, long-term care facilities, hospice organizations, and other health care companies (Fig. 1). In addition to acute care hospitals, 3 long-term hospitals, 12 rehabilitation facilities, and 40 skilled nursing facilities participated in the collaborative. Because PART focused initially on quality improvement and educational efforts for acute care hospitals, this report primarily describes hospital participation and activities. Fifty-nine of the 64 (92%) acute care hospitals in the state of South Carolina participated in some aspect of this learning collaborative, and 9 of the 10 multihospital systems participated (Table 1). Approximately one third of participating facilities were located in rural settings, and most were not-for-profit. Bed size of facilities was distributed from <50 to ≥400 total beds. Forty-nine hospitals (86%) participated in at least 1 PART webinar or group coaching call, with 34 (58%) participating in ≥3 of these events. Statewide meetings were attended by approximately 61% of all participating hospitals, and regional meetings had similar attendance levels. Based on observation, regional meetings offered the ability for larger delegations from regional participating hospitals to attend together. Multiple hospitals also engaged in individualized consultations by telephone, e-mail, or in-person visits.
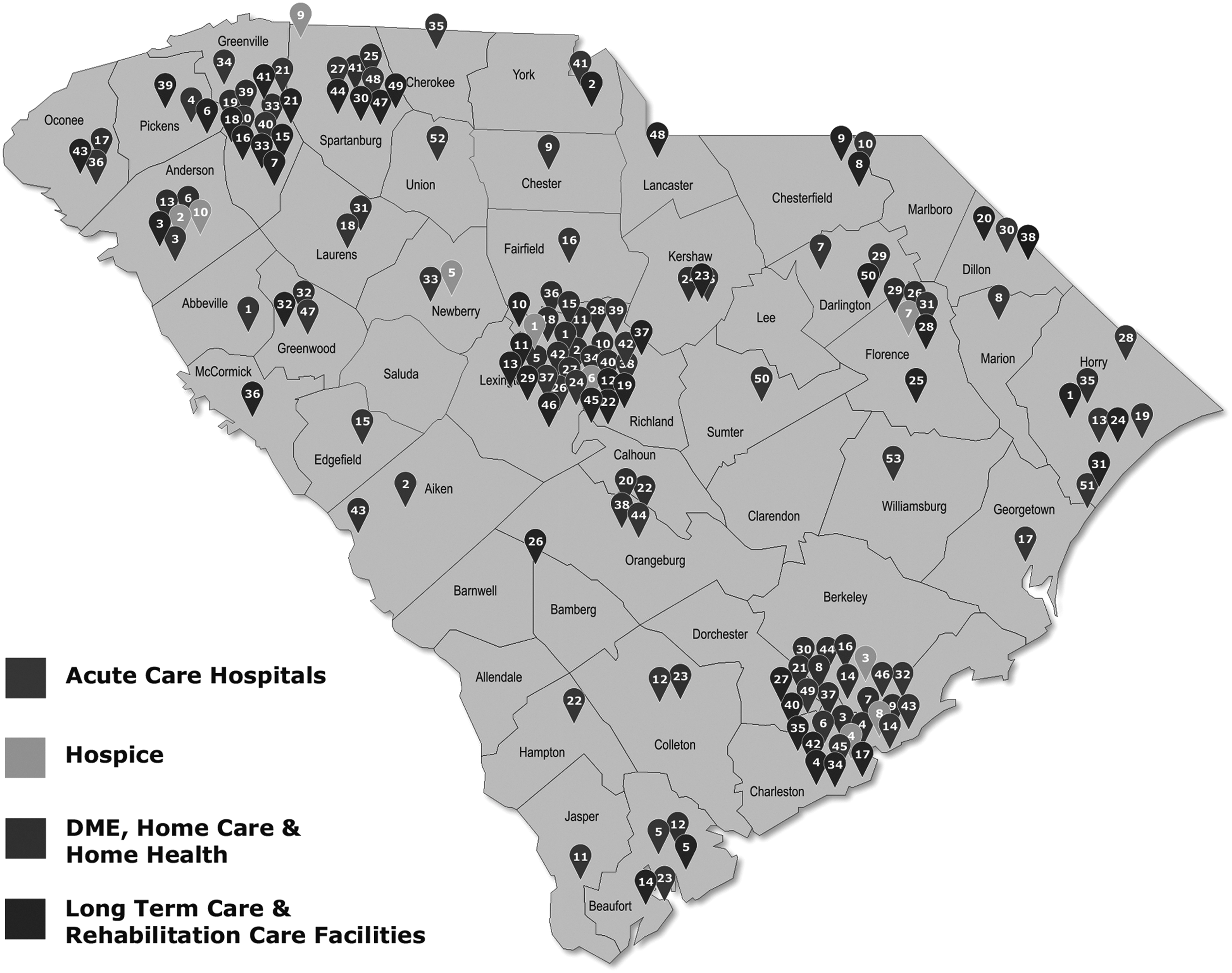
Type and geographic distribution of PART participating organizations. DME, durable medical equipment; PART, Preventing Avoidable Readmissions Together.
Overall, 92% (59 of 64) of statewide acute care hospitals and 90% (9 of 10) of multihospital systems participated in the PART program.
†Among 21 total webinars/group coaching calls.
‡Thirty-seven hospitals participated in one of 3 regional meetings in Year 1, and 24 hospitals participated in one of 3 regional meetings in year 2. Forty-four unique hospitals participated overall.
PART, Preventing Avoidable Readmissions Together.
As depicted in Figure 2, surveyed hospitals contemplated and implemented a variety of different care transitions quality improvements during the PART collaborative period. Respondents most commonly described fully implementing multidisciplinary rounds to address care transitions needs of inpatients and post-discharge telephone calls (58% for each). Teach-back techniques and strategies for timely follow-up appointments were fully implemented in more than a quarter of respondents as well (32% and 26%, respectively). More than half of respondents were in the process of implementing improved high-quality transition records (52%), strategies to improve discharge summaries (45%), and timely follow-up appointments (39%). Finally, a large proportion of respondents (48%) indicated that dedicating personnel as transitions coaches was not a current focus of their quality improvement efforts. The survey had 3 open-ended questions concerning barriers and successes within their institution and which pieces of the PART program were most helpful.
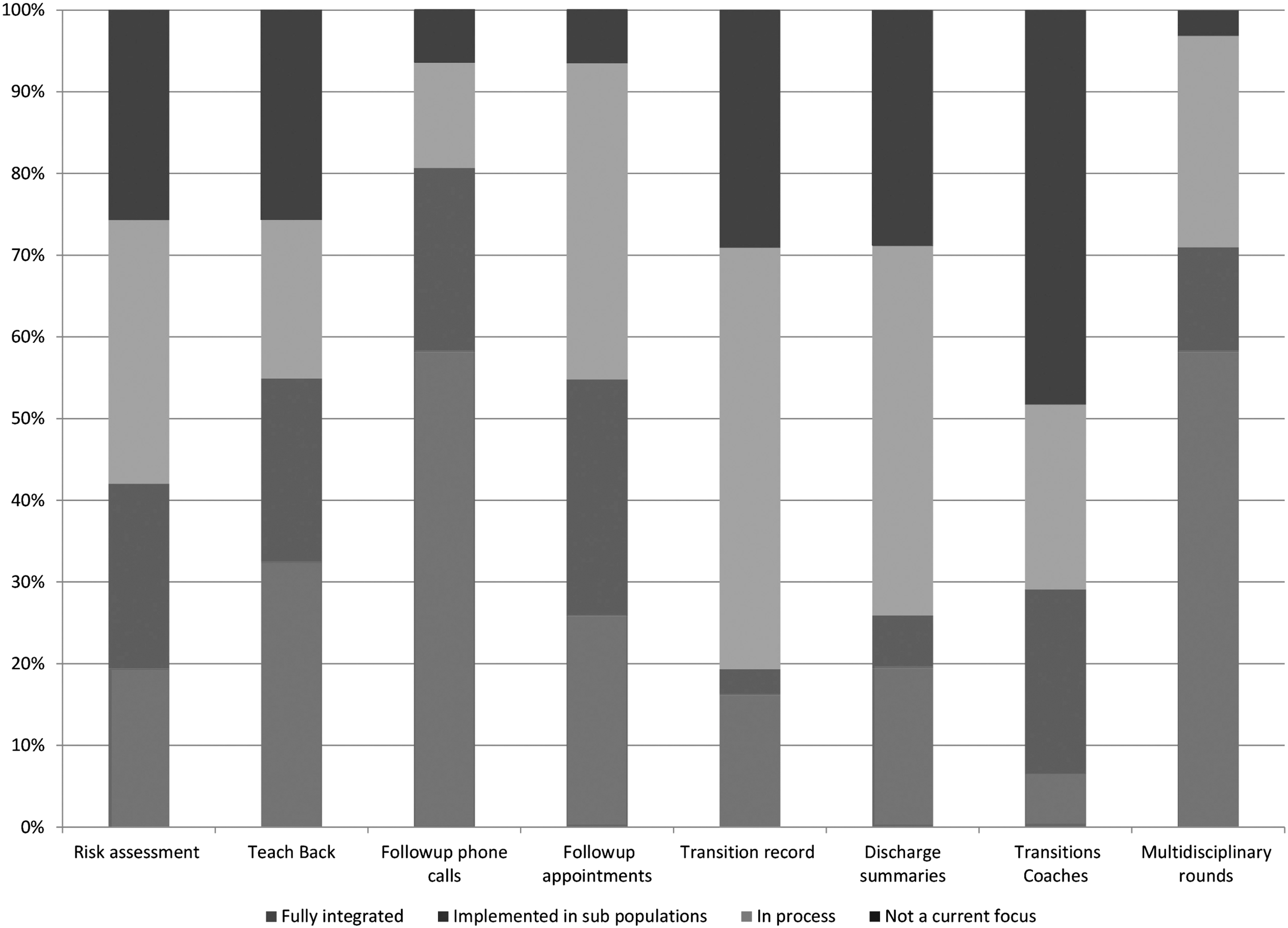
Care transitions improvement strategies and levels of implementation (n=34).
Based on survey responses and informal feedback, PART participants cited common themes related to hospital barriers to quality improvement, including lack of resources (staffing time and competing priorities), communication and buy-in from departments within the hospital (physicians, ED, information technology), and lack of primary care access. The most common themes cited for successes within the collaborative were stronger community partnerships, increased multidisciplinary involvement, improved discharge summary completion time, identification of high-risk patients, implementation of follow-up phone calls, and increased awareness about readmissions at an institutional level. Some hospitals indicated that the networking and examples from other facilities were most helpful, specifically referring to listservs, face-to-face meetings, and webinars. Others indicated that online tools, resources, and access to subject matter experts were most helpful.
As depicted in Table 2 (left portion), the all-cause 30-day hospital readmission rate for all diagnoses at acute care hospitals in South Carolina decreased (improved) from calendar year 2011, the final full year before PART initiation, to 2013, the first full year of PART as did readmission rates for COPD, AMI, and CHF. Readmission rates did not decrease for pneumonia. No statistical significance was shown in the rates from baseline to remeasurement.
Aggregate unadjusted data on 30-day all-cause hospital readmission rates from calendar year 2011, the final full year before PART, to 2013, the first full year of PART. For comparison across time periods, rate changes also are displayed from an earlier time period, 2009–2011. The total number of hospitals submitting data for any diagnosis in each time period was 61. The number of hospitals reporting discharges for eligible index diagnoses varied in each time period as follows: (2009–2011—All diagnoses 61, AMI 46, PNA 60, CHF 60, COPD 60; 2011–2013—All diagnoses 61, AMI 45, PNA 60, CHF 59, COPD 60). Data source: South Carolina Office of Revenue and Fiscal Affairs.
†Statistical significance determined by paired t test. NS=not statistically significant
‡Statistical significance determined by McNemar test (test of 2 proportions) NS=not statistically significant.
PART, Preventing Avoidable Readmissions Together.
Table 2 (right hand portion) depicts the proportion of South Carolina hospitals experiencing relative decreases (improvements) in unadjusted 30-day hospital readmission rates of ≥10% between (2011–2013) than the earlier time period (2009–2011). A higher proportion of hospitals had decreases in all-cause readmission rates for AMI in the later time period of 2011–2013, (P=0.03) and the proportion trended favorably for CHF and COPD. Overall, the proportion of hospitals with a 10% or greater improvement in readmission rates for all diagnoses actually diminished (21.3% vs. 16.4%, NS) but did not change for pneumonia. These results show that there was a significant difference between the 2 proportions for AMI and that the difference approached significance for CHF. Results of paired-sample t tests illustrate a significant mean difference in the scores for AMI 30-day readmission rates of 2009–2011 and 30-day readmission rates of 2011 to 2013; t(28)=−2.28, P=0.03. Results also show that there was a near significant mean difference in the scores for CHF 30-day readmission rates of 2009–2011 and 30-day readmission rates of 2011 to 2013; t(29)=−1.84, P=0.07.
In addition, during the PART time period between 2011–2013, the proportion of hospitals experiencing a 10% or greater relative reduction in 30-day all-cause hospital readmission rates was better than the proportion experiencing significantly worse rates over the same period for several conditions specifically targeted by PART. These included AMI (22.2% vs. 55.6%), CHF (18.6% vs. 54.2), and COPD (26.7% vs. 41.7%). The proportion of hospitals with changes in readmission rates for all diagnoses and for pneumonia did not differ between 2011 and 2013 and the earlier time period.
Discussion and Conclusions
This report describes the design, implementation, and early results of a harmonized, multi-stakeholder statewide collaborative to reduce readmissions and improve hospital care transitions. This approach has resulted in sustained engagement and continued progress regarding interventions implemented or in process at a diverse group of hospitals with varying resources. Ninety-two percent of South Carolina's acute care hospitals have participated in some aspect of the collaborative. Facilities report having completed or begun implementation of a variety of care transitions improvement strategies. Initial data seem to indicate aggregate improvement for selected conditions and increasing pace of change in readmission rates at a statewide level.
The PART program has borrowed from the IHI STAAR (State Action on Avoidable Rehospitalizations) program model's 2-part strategy to reduce hospitalizations, which is: (1) To improve transitions of care by cultivating a cross-continuum learning collaborative, and (2) To engage state-level leadership to understand and mitigate systemic barriers to change. 23 PART provided participating hospitals with tools and educational materials, in-person and virtual learning, and targeted technical assistance. These results and those of initiatives such as STAAR highlight the feasibility of broad reach through learning collaboratives. However, there may be a trade-off in effectiveness given that PART did not advocate or require any specific care transitions program. Thus, organizations planning large-scale collaboratives must balance considerations of cost, reach, intervention intensity, and intervention flexibility.
The PART collaborative has learned important lessons. First, participating organizations had widely varying degrees of quality improvement knowledge, expertise, and experience. Teams at some facilities had no prior training in lean methods or quality improvement, whereas one participating community was awarded a Community-Based Care Transitions Program demonstration project from CMS, recognizing their advanced performance. This variability forced the addition of content in learning sessions and in the resource guide describing basic quality improvement techniques, and these topics were heavily emphasized during individual consultations. Second, facilities described widely varying levels of leadership engagement, which has been described as a critical success factor for care transitions and other translational efforts. 24 Third, participating hospitals expressed multiple concerns related to the collection and sharing of process data. Hospitals were not required to sign or commit to the program in order to participate in any activities or receive reports. Only 44% (26 of 59) of participating hospitals signed a data use agreement with the PART collaborative for the purpose of evaluating processes of care, and only 1 hospital consistently uploaded their process measure data, despite this being offered at no cost, and having an expected time requirement of less than 120 minutes per month. When it became clear that reporting process measures would not be successful, our program focused on enhanced and timely outcome reporting. Finally, the leadership group recognized that flexibility was paramount to enabling the engagement of hospitals.
This report should also be evaluated in light of certain limitations. First, this is a descriptive report of a statewide quality improvement collaborative to reduce readmissions across a single state, and these experiences may not be generalizable to other states or topics of healthcare improvement. Second, the research team captured data at the hospital level. Without information on the number of individual participants from a given organization in each learning activity, the team is unable to make specific statements regarding levels of individual activity. Finally, the program survey found in Figure 2 had a response rate of 58% among participating hospitals. These observations regarding care transitions improvement tactics may not represent the full range of tactics implemented; however, they do provide valuable insight into the current ecology of such efforts in the state.
Though encouraging, readmission rate data presented in this report should be interpreted with caution. First, the research team was not able to make statistical adjustments for patient- or facility-level variables in these aggregate observations. Thus, the temporal association between participation in the PART program and readmission rate improvements may not be causal. Second, emerging evidence suggests modest national improvements in 30-day hospital readmission rates. 25 Based on comparison of calendar year 2012 to 2007–2011, Gerhardt and colleagues reported that the all-cause 30-day hospital readmission rate for hospitalized Medicare patients decreased from 19% to 18.4%. 26 In addition, the present study data indicate ongoing implementation of various care transitions improvement strategies among participating PART facilities. Thus, the full effects of participation in this collaborative likely are as yet unrealized. In the future, the research team plans robust analyses using appropriate adjustment for patient- and facility-level variables to assess readmission rate outcomes. Additional qualitative and quantitative analyses will focus on specific organizational and programmatic characteristics of high-performing facilities.
In sum, the current health care atmosphere features increasing scrutiny of hospital readmissions, and most hospitals and other health care organizations are currently working on or contemplating care transitions quality improvement efforts to address this problem. Organizations face an increasing array of choices for quality improvement programs, and it may be desirable to coordinate these programs in order to accelerated learning and foster peer engagement through a collaborative, rather than competitive, model. The South Carolina PART learning collaborative has successfully engaged key partners in care transitions efforts on a statewide level while garnering high participation rates from different health care organizations.
Footnotes
Author Disclosure Statement
Drs. Axon, Moonan, Foster, Cawley, Long, and Turley, and Ms. Cole declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for the research, authorship, and/or publication of this article.
Acknowledgment
The authors would like to thank Hrishikesh Chakraborty, DrPH of the University of South Carolina for his technical assistance and advice in performing our analysis.