
Abstract
Community health worker (CHW) programs are an increasingly popular strategy for patient-centered care. Many health care organizations are building CHW programs through trial and error, rather than implementing or adapting evidence-based interventions. This study used a qualitative design-mapping process to adapt an evidence-based CHW intervention, originally developed and tested in the hospital setting, for use among outpatients with multiple chronic conditions. The study involved qualitative in-depth, semi-structured interviews with chronically ill, uninsured, or Medicaid outpatients from low-income zip codes (n = 21) and their primary care practice staff (n = 30). Three key themes informed adaptation of the original intervention for outpatients with multiple conditions. First, outpatients were overwhelmed by their multiple conditions and wished they could focus on 1 at a time. Thus, the first major revision was to design a low-literacy decision aid that patients and providers could use to select a condition to focus on during the intervention. Second, motivation for health behavior change was a more prominent theme than in the original intervention. It was decided that in addition to providing tailored social support as in the original intervention, CHWs would help patients track progress toward their chronic disease management goals to motivate health behavior change. Third, patients were already connected to primary care; yet they still needed additional support to navigate their clinic once the intervention ended. The intervention was revised to include a weekly clinic-based support group. Structured adaptation using qualitative design mapping may allow for rapid adaptation and scale-up of evidence-based CHW interventions across new settings and populations.
Introduction
C
The process of scaling an EBI to new settings creates a tension between fidelity and fit. 2 On one hand, fidelity to an EBI is important for efficiencies of scale and adherence to core components of effectiveness. On the other hand, programs must be adapted to accommodate new settings and patient populations. The literature focuses on adaptations of EBIs to new cultural contexts (eg, adaptation of the Diabetes Prevention Program for a Latino population 3,4 ), but considerations are similar when adapting EBIs for new delivery settings (eg, adapting a hospital-based tuberculosis program for use in community settings 5 ) or diseases (eg, adapting a substance abuse behavioral intervention for use among smokers 6 ).
Historically, unplanned and often unstructured program adaptation has been widespread. 7 In recent years, the implementation science field has explored practical, yet scientific “planned adaptation” strategies to guide this process. Numerous published guidelines and frameworks 2,3,8,9,10 emphasize the importance of beginning with a “manualized” EBI whose core components, structure, and protocols are well described in an intervention manual. Building on this literature, Goldstein et al 11 recently described a stepwise process (Table 1) for adapting manualized EBIs, which has been applied to adapt an anger management intervention for juvenile offenders 12 and exposure therapy for post-traumatic stress disorder. 13 This process is grounded in participatory action research methodology in which researchers engage stakeholders—using qualitative interviews or focus groups—to better understand the new setting and inform adaptation. 14 –18 Yet, even when guided by this process, it can be difficult to know exactly how the results of participatory research should be translated into specific revisions of intervention manuals. In practice, these granular decisions are often made quite subjectively.
CHW, community health worker; RCT, randomized controlled trial
This paper describes adaptation of IMPaCT 19 —a manualized, evidence-based CHW intervention originally developed and tested in the hospital setting—for use among outpatients with multiple chronic conditions. Although IMPaCT was originally developed for the hospital setting, the study team was always interested in efficiently adapting and scaling the core model across settings and populations. This paper focuses on 2 critical, yet poorly described, steps of adaptation: the use of in-depth qualitative interviews to understand the new setting and population, and use of design mapping to translate interview findings into manual revisions.
Methods
IMPaCT transitions: a CHW intervention for improving post-hospital outcomes
IMPaCT was originally designed by a multidisciplinary team using participatory research. 20 The study team conducted in-depth qualitative interviews 21 –23 with low-income hospitalized patients, and designed core intervention components to address the main themes of these interviews (Fig. 1). First, patients felt that they were being “set up to fail” when providers set discharge goals that were unrealistic. 22 Therefore, the team developed the intervention based on goal-setting theory 24 to help patients set meaningful goals. Second, participants described a sense of disconnect from traditional health care personnel and wished for support from someone to whom they could relate. Therefore, the study team focused on using a workforce, CHWs, who came from a similar background. Finally, patients experienced many barriers to accessing post-hospital primary care and often felt compelled to return to the emergency room when they felt sick. 25 Therefore, the team decided that CHWs would end the intervention by connecting patients to high-quality primary care. A 3-stage structure was designed for the intervention based on these core components: goal setting, tailored support, and connection with primary care (Fig. 1).

Designing the original IMPaCT intervention
After determining core components and structure, the study team used design mapping to make decisions about granular program elements (Fig. 1). First, the team listed all 30 barriers described by patients in interviews. For each barrier, the team used logical problem solving—and patients' suggestions from the interviews—to answer the question: What intervention step would solve this problem? The team then asked: What traits and skills would someone need to have in order to deliver this intervention step? This iterative process was followed for each barrier until a detailed design map had been created. The Intervention column became the basis for intervention manuals, the Traits column informed CHW hiring guidelines, and the Skills column helped the study team to develop a training curriculum. 20
In the resulting IMPaCT Transitions intervention, CHWs meet eligible patients 20 on the day of hospital admission and ask: “What do you think you will need in order to stay healthy after discharge?” CHWs help patients to set their own goals and action plans for recovery. CHWs then provide 2 weeks of tailored support to help patients reach their goals. Finally, CHWs make sure patients are connected to primary care as a source of long-term support. IMPaCT Transitions include standardized program infrastructure, including hiring guidelines, training, and detailed manuals for work practice. 26 A randomized controlled trial (RCT; n = 446) 19 demonstrated that the 2-week intervention improved access to primary care, quality of discharge communication, mental health, and patient activation while reducing recurrent hospital readmission.
Adapting IMPaCT for outpatients with multiple chronic conditions: an overview
The goal was to adapt the intervention for outpatients with multiple chronic conditions, yet retain core components of effectiveness and allow for efficiencies of scale. The study team defined efficiencies of scale as the ability to cross-train CHWs and have a single manager supervise both interventions. Adaptation was led by a collaborative team including researchers, health system leaders, clinicians, and CHWs. The study team used the Goldstein framework as a guide during the adaptation process (Table 1); this paper focuses on the conduct of qualitative interviews and translation of interview findings into manual revisions.
In-depth qualitative interviews
Study design, setting, and participants
The qualitative interviews were part of a larger study; details and participant characteristics have been described elsewhere. 27,28 Briefly, between August of 2012 and March of 2013, interviews were conducted with 51 individuals (21 patients, 30 primary care staff) from 3 primary care clinics. Patients were: (1) diagnosed with ≥2 of the following: asthma/chronic obstructive pulmonary disease with tobacco dependence, hypertension, obesity, hyperlipidemia, diabetes; (2) uninsured or publicly insured; (3) residents of a high-poverty 5-zip code region of Philadelphia. Patients were excluded who: (1) had not been seen in study clinics for at least 1 year; (2) lacked decision-making capacity and a caregiver who could be interviewed as proxy. Clinic staff participants were employees of study clinics and purposively sampled in order to include a range of roles. The study was approved by the Institutional Review Board of the University of Pennsylvania.
Data collection and analysis
Patients were interviewed by a CHW trained in qualitative interviewing; clinic staff were interviewed by research assistants. Interview guides explored barriers patients faced in improving their health and ideas for improving care. All interviews were conducted in private clinic rooms, audio-taped, and transcribed. A modified grounded theory approach 29 was used for analysis: the study team developed a coding structure including major ideas that emerged from a close reading of the data, as well as a set of a priori codes from the conceptual framework. Using the constant comparison method, the study team analyzed transcripts synchronously with data collection, continuously refining and adapting the interview guide based on participant responses.
Design mapping to translate interview findings into manual revisions
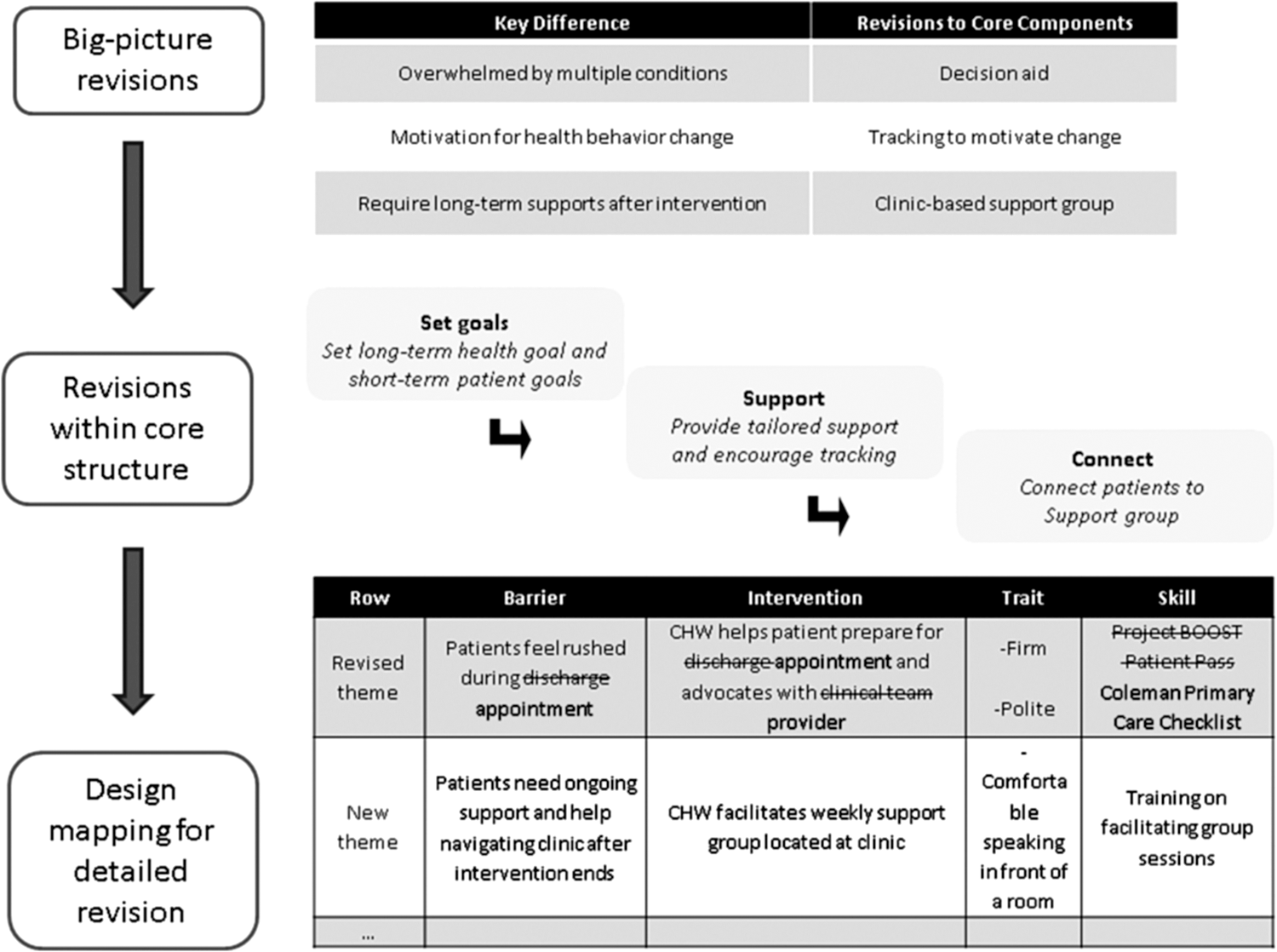
The team revised core intervention components to address the main themes that arose from the interviews (Fig. 2). Then design mapping was used to guide more detailed revisions: the study team started with the design map that arose from the IMPaCT Transitions study and then revised the Barriers to fit data from the current study of outpatients with multiple chronic conditions. The team then modified the Intervention, Skills, and Traits using logical problem solving and participants' suggestions. The revised design map was then presented to working group members for checking and validation, and subsequently used as the basis for manual revisions.
Adapting IMPaCT for outpatients
Results
The study team found that the IMPaCT Transitions design map was generally aligned with what had been learned from outpatients with multiple chronic conditions and their clinic staff. However, 3 key differences informed revisions of the intervention's core components (Fig. 2).
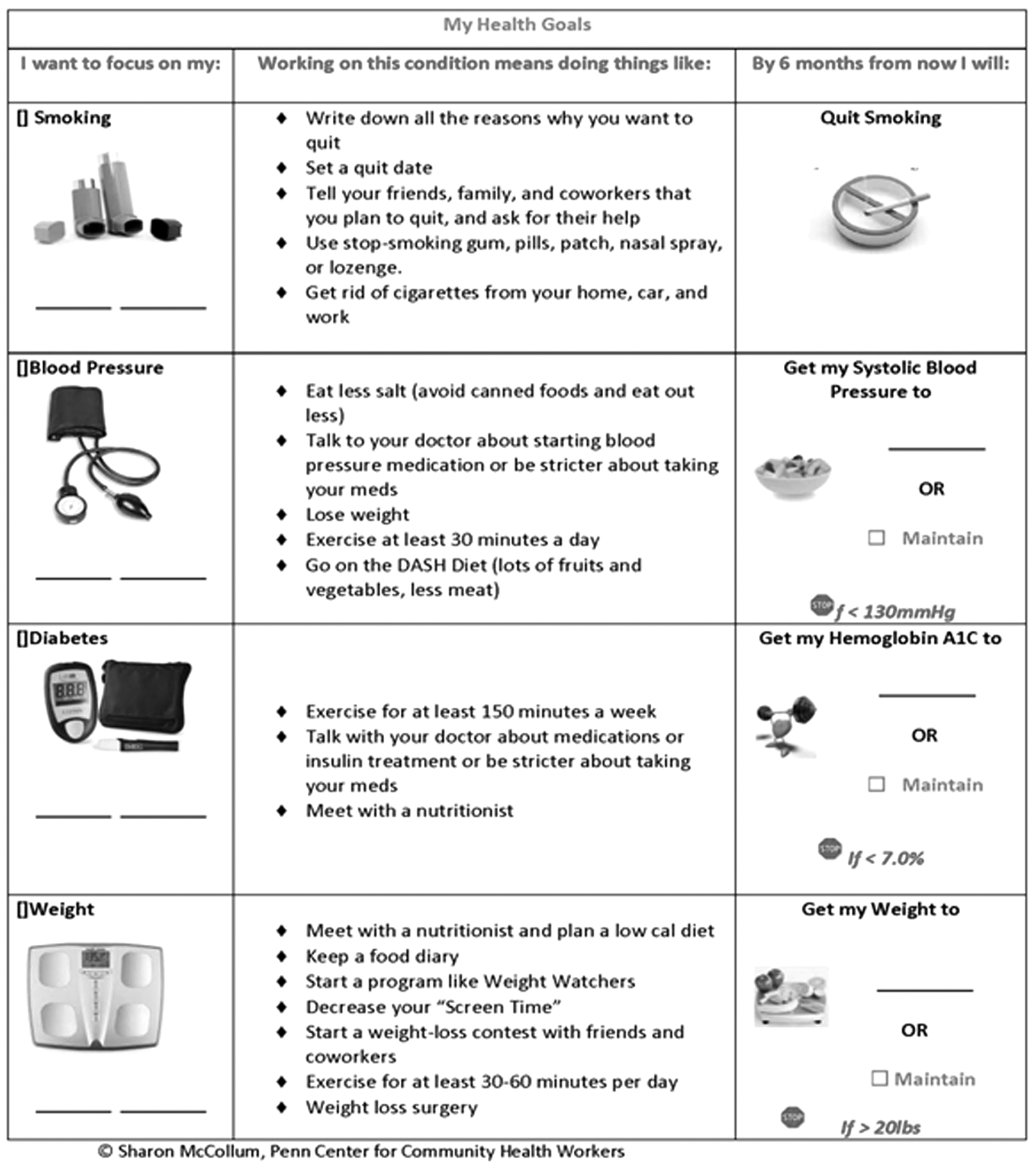
First, outpatients with multiple chronic conditions were overwhelmed by those conditions and wished they could focus on 1 at a time. Thus, the first major revision was to design a low-literacy decision aid that patients and providers could use to set a single chronic disease management goal to focus on during the intervention (Fig. 3). Second, motivation for health behavior change (eg, diet, physical activity) was a more prominent theme in this study than in the prior transitions study. The study team decided that in addition to providing tailored social support, CHWs would help patients to track progress toward their chronic disease management goal in order to motivate health behavior change. Third, patients were already connected to primary care; yet they still needed help navigating their clinic and wanted other sources of long-term support to sustain progress once the CHW intervention ended. The study team decided that CHWs would facilitate a weekly support group for patients at clinic sites to encourage patients to feel more comfortable within their clinic and to get longitudinal support once the program ended.
The Goal Card: a decision aid for patients with multiple chronic conditions
Detailed areas of overlap and tension between the IMPaCT Transitions study and new data from outpatients with multiple chronic conditions and their clinic staff will be described.
Establishing a relationship
As in the IMPaCT Transitions study, although most patients liked the staff generally, they described a social distance: “I've got to lift furniture all day. [Doctor] sits in his chair in front the computer all day, so he don't lift no heavy stuff. I'm blue collar, okay? He's a white collar. He doesn't understand me.” A few patients experienced a more extreme disconnect from staff, which they attributed to institutional racism or classism, “I been living in the suburbs, so I was used to [clinic staff] saying, ‘What can I do for you?’ Now, by this being—it's a poor neighborhood..they treat people like drug addicts.”
Clinic staff themselves acknowledged that they were not familiar enough with community resources (eg, food banks, shelters, childcare) to offer practical solutions to the socioeconomic barriers patients faced. “We work on the inside,” one case manager summarized. Another scheduler explained, “Sometimes patients…would rather talk to someone from the community. These are people that they see in the market, at the bus stop…. They feel connected.”
As in the IMPaCT Transitions study, patients said that in order to establish a trusting relationship with a CHW, they would want the CHW to be nonjudgmental: “I wouldn't want someone to be judgmental of who gets [addiction] treatment and who doesn't…. A lot of that goes on.” Patients also emphasized that CHWs should be reliable and easily available when patients needed them.
Patient goal setting
Patients described feeling overwhelmed with their multiple conditions, and wished they could “focus on one health condition at a time so I could really reach that goal.” They also explained that they thought about goals differently than providers, who either counseled patients to “fix everything all at once” or focus on the thing that would “kill them.” Patients preferred to set goals that were realistic, “[My doctor] tells me I need to lose weight by exercise. But my job is home care and that is 24/7. So it's difficult for me to leave her by herself and, you know, go for a walk or anything as I would like to for the exercise.”
As in the transitions study, patients also described the need for tailored strategies to reach their health goals: “Person is blind, you want to hook them up to a blind association. Needs education, hook them up to diabetes associations so they're getting information steadily. Everybody's different.” Another patient elaborated, “Listen to what my concerns and my problems are. And come up with some type of a solution for how to help [me] reach my goal.”
Based on this input, the study team modified the goal-setting stage of the IMPaCT Transitions intervention. First, providers would use a decision aid (Fig. 3) to help patients set a single chronic disease management goal: weight, blood pressure, glycosylated hemoglobin, or daily cigarettes. Next, CHWs would use the standard IMPaCT Transitions approach to deconstruct this long-term chronic disease management goal into patient-driven short-term goals by asking, “Mr. Jones, what do you think you'll need in order to reach that goal of lowering your blood pressure to 140/90?” Ultimately, this conversation would help patients create action plans to reach the short-term goals they believed necessary for chronic disease management (Fig. 4).

Community health worker and patient goal setting
Goal alignment
As in the IMPaCT Transitions study, health care staff often did not seem to understand patients' goals and priorities. One clinic's diabetes educator explained: “Patients [are] overwhelmed with other life issues…. We have to know this is going on and close this gap.” Patients explained that it was difficult to drive or even explain their agenda when they felt rushed and as if the clinic staff were “trying to ship me out.”
Both clinic staff and patients thought it would be useful for the CHW to play a bridging role and “get them on the same page.” Despite their interest in working alongside CHWs to better understand patients' perspectives, clinic staff had divergent opinions on how best to accomplish this. About half of the clinic staff suggested conversations either through telephone calls, impromptu meetings, or scheduled multidisciplinary team huddles. Other clinic staff worried that there would be no time for such meetings: “If you're meeting you are not seeing patients. Even a half an hour out of the day is a very expensive process.” These staff members suggested that CHWs communicate with key clinic staff via messages in the electronic medical record (EMR).
The study team decided to use EMR messages containing information about patients' short-term goals and action plans as the minimum form of communication from CHWs to clinic staff. CHWs also would call providers whenever clinical issues arose, and participate in multidisciplinary huddles when those existed within the practice infrastructure.
Goal support
Patients described needing tailored support to address many of the same types of barriers described in the IMPaCT transitions study: psychosocial, daily life resources, medical, neighborhood, and health behavior. 20 However, the relative importance of some barriers was different: health behavior change was a more salient barrier for outpatients with multiple chronic conditions than for hospitalized patients focused on the transition from hospital to primary care.
Some patients discussed difficulty with changing diet: “Eating is an experience and we eat for different reasons.” Others explained the challenges of exercise: “I have no cartilage in my right hip so I can't do no walking. So it's like whatever I do, it's defeating it. If I walk, then my leg hurts. If I don't, I don't lose weight.” Other patients described quitting smoking: “That cigarette has been there for 33 years…it's my friend.”
Despite talking about different behaviors, patients used a common language to describe the underlying process of behavior change: “It's a change of habits. And when you change habits and you don't have somebody there to constantly keep reminding you, you'll go back to your old habits. So [you need] somebody there that's gonna help you and then once you get it, everybody knows you got it.”
Patients had consistent descriptions of the type of support they would need in order to change health behaviors. “I want the person to not set goals that are so high that it becomes disappointing and frustrating, but to be moderate in working with that person and saying okay, let's regulate this.” Others suggested helping patients to track progress and provide empathic troubleshooting when things were not going well: “[The CHW] would be able to make adjustments, but won't be frustrated if I don't reach those adjustments.” As in the prior transitions study, patients again emphasized the importance of instrumental support, rather than just informational support, “Come along and maybe walk with me and encourage me to walk.”
The team decided that CHWs would need to work with patients for at least 6 months (with at least 1 weekly call or visit) in order to support habit change. As in the IMPaCT Transitions intervention, CHWs would provide tailored instrumental and emotional support to help patients reach the short-term goals (eg, housing, addiction treatment) that they identified during the initial meeting. CHWs also would provide hands-on support with health behavior change by being a “buddy” to patients (eg, going swimming with them at the local YMCA). In addition, during weekly encounters CHWs would encourage patients to self-monitor (weight, blood pressure, blood sugar, or daily cigarettes) to track progress toward their chronic disease management goal. If patients were not making progress, CHWs would troubleshoot and provide empathic motivational interviewing, and be careful not to appear judgmental.
Ongoing support
Unlike the IMPaCT Transitions study, outpatients in the present study sample had been going to the same practice for at least 1 year. However, despite being more “plugged in” to a primary care clinic, these patients described many of the same barriers that hospitalized patients had with accessing and navigating primary care. Patients thought that additional support structures would need to exist within the clinic in order for this to be an effective “hand-off” once the CHW intervention ended.
The study team decided that, as in the IMPaCT Transitions intervention, CHWs would offer to accompany patients to appointments or use 3-way phone calls in order to coach patients on how to navigate their clinics. In addition, CHWs would facilitate a weekly support group that would be located within the clinic. The support group could make patients feel more comfortable in their clinic and provide patients with ongoing peer support even after the 6-month CHW intervention ended.
Completing the adaptation process
After using design mapping to revise intervention manuals, the study team continued Goldstein's process (Table 1), piloting the adapted intervention, making additional manual revisions based on feedback from CHW focus groups, and creating a final IMPaCT Outpatient Care manual.
26
The entire adaptation process took 10 months (August 2012 through June 2013). During this time, the team grew from 2 to 6 CHWs and was able to achieve the efficiencies of scale intended at the outset of adaptation; all 6 CHWs were cross-trained in both the IMPaCT Transitions and Outpatient interventions, and a common manager could supervise a team consisting of a mix of Transitions and Outpatient CHWs. In July of 2013, the team launched a single-center RCT (
Interim data from these RCTs and low operating costs resulting from efficiencies of scale were used in a return on investment analysis for the parent health system, Penn Medicine ($1.80 return for every $1.00 invested in the program), and led to the creation of the Penn Center for CHWs. Between June 2013 and July 2014, the center grew from 6 to 24 CHWs, supported by Penn Medicine's operational dollars to deliver IMPaCT to 1500 patients annually.
Discussion
This paper builds on Goldstein's framework by describing the use of design mapping to translate the results of in-depth interviews into intervention manual revisions. This methodology encourages a systematic approach to revisions that incorporate stakeholder input. It is also efficient; focal adaptations address differences between intervention populations, while allowing retention of many common elements. The result was rapid adaptation of an EBI based on feedback from target users. Although the participatory design process increases the likelihood that the intervention will have the intended effect, ongoing RCTs ultimately will determine whether the adapted interventions are indeed effective.
This paper is relevant to the growing interest in CHW programs across the United States. 30 The shift toward accountable care incentivizes health care organizations to improve population health outcomes at low cost. Because many of the factors that influence the health of populations—particularly low-income patient populations—exist outside the traditional health care setting, organizations are increasingly interested in community-based approaches.
Despite the potential benefit of this trend, the process by which some CHW programs are being developed can lead to disappointing outcomes. 1 The concept of training laypeople to support high-risk patients has enough face validity that many payers and provider organizations are tempted to “just try it.” This trial-and-error approach has 3 problems. First, when thousands of practices, payers, and hospitals each try to design their own de novo CHW program, the result is fragmentation. Second, as in any other field, “reinventing the wheel” is costly, time-consuming, and leaves programs open to making well-described and remediable mistakes, ultimately threatening their long-term sustainability. Third, many trial-and-error CHW interventions lack formal evaluation. As a result, even when new interventions are effective, the results often are not published and shared.
It would be preferable to use a systematic process to adapt and retest existing EBIs for new contexts. This study demonstrates that the process can be efficient—less time-consuming than many trial-and-error approaches—but does require capacity for rigorous implementation science that smaller health care organizations may lack. Ideally, health care organizations interested in launching CHW programs would receive technical assistance from implementation scientists to guide them through a structured adaptation process.
In the future, the methodology described in this paper may allow for more widespread and varied adaptation of the IMPaCT model. The Penn Center for CHWs is currently exploring adaptation for new high-risk populations (eg, patients with sickle cell disease or high-risk pregnancy) and settings (eg, remote rural areas where there is limited access to traditional medical care). In addition, the design-mapping process can be used not only for adaptation of an EBI to new settings, but also during intervention refinement. Qualitative interviews are often part of process evaluations, yet it can be difficult to translate the results of these interviews into intervention refinements. Design mapping may be an effective approach for this process.
This article has limitations. First, because of the qualitative design, a relatively small number of in-depth interviews were conducted. As a result, interviews—and the revisions made based on these interviews—may not have reflected the perspectives of the broader patient population. Second, the study team focused on adaptation of the intervention to a small number of new clinics and, therefore, studied relatively few settings. When adapting the intervention to very different settings, such as rural communities or immigrant populations, a larger sample size encompassing multiple settings may be required in order to reach thematic saturation.
In conclusion, as policy makers consider ways to stimulate the scale-up of CHW programs across the country, it will be important to strengthen linkages between implementation scientists and health care organizations in order to efficiently adapt proven approaches.
Footnotes
Author Disclosure Statement
Drs. Kangovi, Glanz, Long, and Grande, and Ms. Carter, Ms. Charles, and Ms. Smith declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for this article.