
Abstract
As Medicare and Medicaid increasingly shift to alternative payment models focused on population-based payments, there is an urgent need to develop measures of population health that can drive health improvement. In response, an assessment and design project established a framework for developing population health measures from a payer perspective, conducted environmental scans of existing measures and available data infrastructure, and conducted a gap analysis informing measure development and infrastructure needs. The work, summarized here, makes recommendations for creating a set of core measures, demonstrates some of the key challenges in applying a traditional quality measure development framework to population health, and complements recent efforts by the National Academy of Medicine and others with a focus on a payer perspective.
Background
T
As a payer, CMS works primarily on health care delivery for beneficiaries and will not be able to cover the full range of needed services, particularly those that are more removed from the clinical care of enrolled individuals. CMS is able to serve as catalyst, helping to transform health care from a fee-for-service system to one that addresses the multiple areas that influence the health of a population. CMS can do this, in part, by directly supporting development of health system infrastructure and, in part, by pursuing partnerships with public health and social programs.
However, the main policy levers available to CMS and private sector payers to achieve these broader population health goals are value-based purchasing initiatives and alternative payment models. 8 Payment can incentivize delivery systems to make needed investments and to adopt population-based strategies. For example, current quality measures for Accountable Care Organizations and patient-centered medical homes already include outcomes that reflect a prevention emphasis, and future performance measures could require health care institutions to refer patients to a wider range of community services and work more closely with local organizations and public health agencies to improve the community's health.
Several well-known models that incorporate multiple determinants of health and multisector collaboration have successfully advanced the field of population health. 9 –13 However, these models may not address the unique needs of payers of clinical services. Payers represent one perspective in a complex, multisector, population health ecosystem and they have distinct requirements and opportunities that the existing public health and clinical quality measurement systems may not fully address.
Quality measurement is a critical tool used by payers to drive health system performance improvement, but current measures within the delivery system generally focus on cost, patient experience, and technical aspects of quality for individuals. A robust population health measure set would have the ability to (1) aggregate the data from individual clinical encounters into meaningful units of analysis such as panels, organizations, delivery systems, and communities; (2) incorporate the health status of individuals in the population who do not present for face-to-face encounters; (3) measure activities, processes, and services that occur between clinical encounters; (4) measure activities, processes, and services delivered outside the facility within community settings; (5) incorporate subjective measures of health status and health-related quality of life; and (6) measure the underlying conditions contributing to poor health that can be acted upon by delivery systems, such as behavioral and environmental factors.
Surveillance and other measurement activities within public health often take a societal perspective that includes individuals not served by a health system and social factors outside the scope of health care. Moreover, such measure sets are often dominated by distal outcomes that change slowly over time. These surveillance systems are useful to the clinical sector for assessment and planning, but often are unable to measure progress at a local level for either internal improvement or external accountability.
CMS seeks to reconcile the clinical and community perspectives by considering the various populations to which an individual belongs as a series of concentric expanding denominators: a panel of patients in a practice, patients receiving care within a delivery system, and larger geographically defined populations (Fig. 1). CMS is working in each of these domains to encourage incremental progress toward population health. Measures are needed to support the programs and policies that try to bridge the gap between public health and clinical quality improvement by looking at individuals within each of these denominators. Large payer organizations could use these measures to catalyze actions within clinical delivery systems and to hold those systems accountable for their role in improving population health.

Reconciling the clinical perspective with a broader community perspective by considering the various populations that an individual belongs to as a series of concentric expanding denominators. Source: Based on Kassler et al. 1
Methods
To create a shared understanding of the role of payers in population health measurement, facilitate communication of complex interactions, identify important processes, and justify choice of indicators, the research team identified a conceptual model to guide the process of developing population health measures. Building on the existing models, the team created a strategic framework to establish a theory, policy, and data-driven approach to developing a population health measurement strategy for CMS that can be generalized to other payers in the private sector.
The research team conducted an environmental scan of quality and population health measure databases and programs used within Department of Health and Human Services (HHS) initiatives. From this, the team compiled an inventory of existing measures pertaining to population health in the clinical and public health sectors (defining public health broadly to include social and environmental determinants such as housing, transit, and employment indicators). The team then examined data sources supporting those measures and conducted a gap analysis to help prioritize future measure development efforts.
To understand when measures may be adapted from other programs instead of through de novo development, measures were categorized as being established if they were currently in use by a CMS program, existing if the measure was not currently in use by a CMS program, and missing if it was not identified as in use by either CMS or other HHS agencies. To identify measures that could be scaled up with current infrastructure, as opposed to those requiring new investments, a companion analysis examined the data sources commonly used to support measures identified in the scan.
Finally, recommendations are presented for a plan to create a usable population health measurement set and to identify an initial group of core measures from existing and candidate measures that reflect where the clinical care sector is capable of having the most meaningful impact.
Results
Strategic framework
A framework adds value when it illustrates the conceptual foundation of a complex set of strategic objectives, incorporating critical concepts that might otherwise be lost, and highlights leverage points for action. A conceptual model (Fig. 2) was developed that focuses on the intersection of 3 sectors (clinical care, public health, and community and social services sectors) and how measurement and action within the clinical sector might improve population health, both for enrolled populations and for the broader population within a community. Measurement is shown to encompass more than the clinical sector alone, including individual and population risks, as well as where the clinical sector interacts with the public health and community sectors. The scope of CMS measurement impact is within the uppermost box, focused on the clinical care sector, but illustrating opportunities for multisector collaboration.
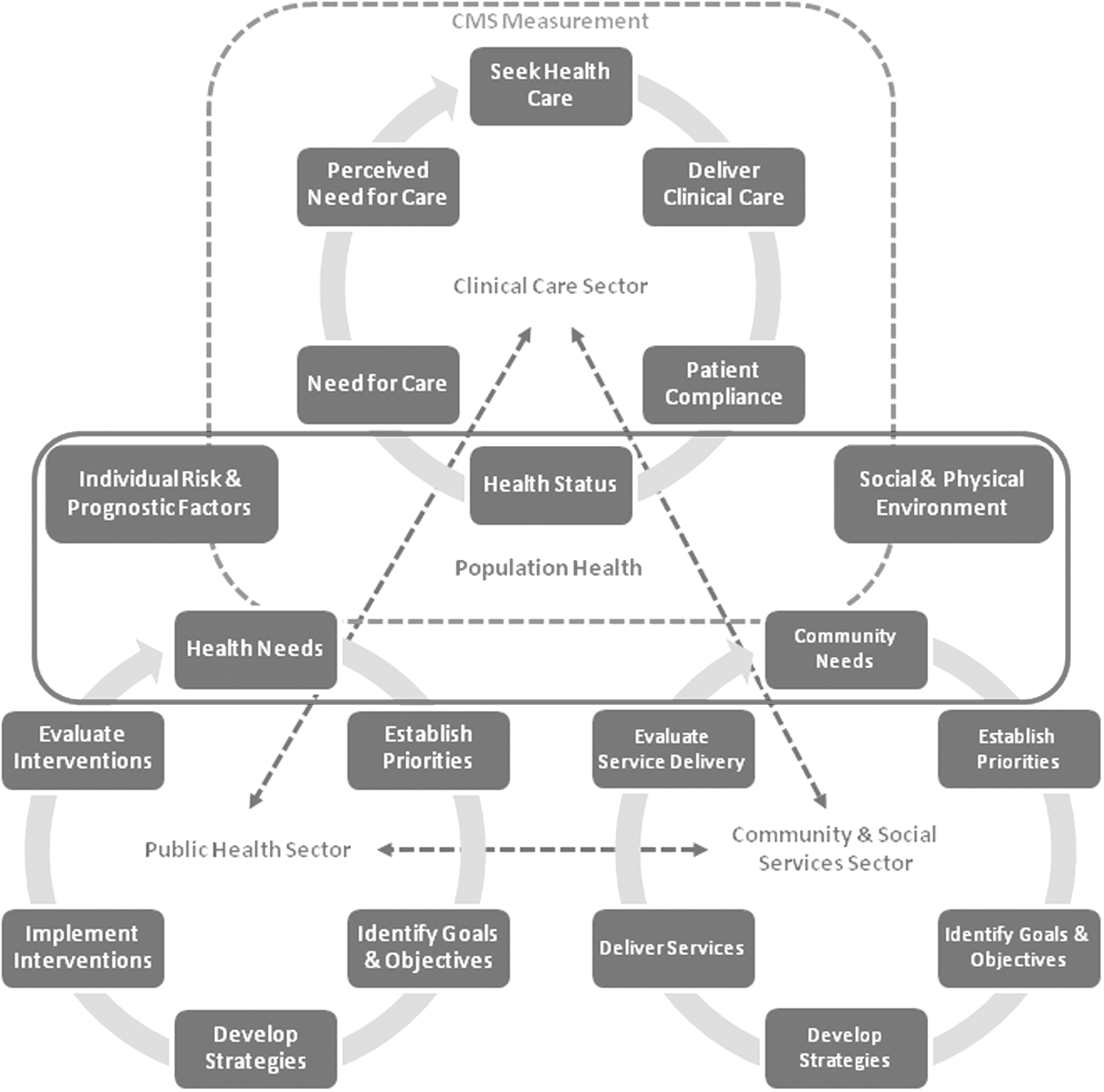
A conceptual model showing population health (center box) at the intersection of the clinical care, public health, and community sectors. The scope of CMS measurement impact is within the uppermost box, focused on the clinical care sector, but illustrating opportunities for multisector collaboration. The role of behavioral, social, and environmental determinants is shown. The dotted arrows between sectors signify collaborative actions, referral and payment for services, and coordinated investment in infrastructure support. CMS, Centers for Medicare & Medicaid Services.
As a step toward identifying priority areas, the framework also includes a driver diagram (Table 1). This diagram illustrates the theory of change, showing the high-level primary drivers of population health outcomes, which are closely aligned with other frameworks. 13,14 Secondary drivers represent the specific areas where payers could have the greatest impact.
Represents a suite of outcome measures, including mortality, intermediate outcomes, quality of life, and functional status.
Represents areas where Centers for Medicare & Medicaid Services already has extensive ongoing work.
The framework, consisting of both conceptual model and driver diagram, exemplifies 2 priority strategies for incentivizing population health approaches within the clinical care sector: (1) addressing the role of multiple health determinants that are modifiable within the context of the health care system and (2) highlighting the need for aligned multisector approaches to bridge the gap between health care delivery and services within community-based organizations and public health agencies.
Environmental scan and gap analysis
A total of 2211 quality measures were identified as potentially pertaining to population health. Measures were assigned to 22 population health topic areas in 6 broad domains: equitable access to care, quality of care, multisector collaboration, health behaviors, upstream determinants, and health outcomes. Table 2 summarizes the distribution of identified measures across topic areas and use status.
E, established; M, missing; X, existing.
Bold values reference row totals and column totals.
The distribution was not uniform across categories. Measures for health behaviors and quality of care were well represented, but relatively few measures were identified related to quality of life, cultural and linguistic appropriateness of services, and multisector collaboration. These are discussed by topic.
Equitable access to care
More than half of the 77 measures in this area dealt with access to appointments and referrals; more than three fourths of these measures were process measures (Table 2). Approximately one fourth of the access measures pertained to Standards for Culturally and Linguistically Appropriate Services. A dozen measures were identified with insurance coverage.
Quality of care
Preventive services had the most measures, with health screenings (n = 177) and immunizations (n = 121) comprising more than half of the preventive services measures (Table 2). The preponderance of existing measures in this area suggests that delivery of preventive services is a well-established topic area compared with other population health areas. Risk assessments of upstream determinants had 47 measures identified in the scan, most of which focused on screenings for environmental and social support.
Multisector collaboration
The scan identified 23 measures of multisector collaboration, all of which focused on clinic–community referrals. Of these, all the structural measures assessed the count of potential community partners, and most of the process measures centered on whether collaboration or referrals were recorded (Table 2). There were no measures related to community health needs assessments.
Health behaviors
This encompassed the largest number of measures, most of which were process measures (Table 2). Measures for physiologic markers (eg, blood glucose, blood pressure, body mass index, cholesterol) were well represented. One fifth of the health behavior measures were for smoking (n = 196) and most of these were found within the public health sector (Table 2). A substantial number of measures pertaining to diet, substance abuse, and physical activity also were collected and used by public health agencies.
Upstream determinants
The scan identified 140 upstream determinant measures, most related to social environmental factors, which included education, employment, income, family/social support, community safety, and food access. Measures of physical environmental factors included air quality, water quality, housing, and transit. Nearly all of the upstream determinant measures were housed in the public health sector (Table 2).
Health outcomes
The largest number of outcome measures was for mortality and functional status (Table 2). Most measures of functional status focused on specific conditions (n = 52), including dementia, joint replacement, and rheumatoid arthritis. Far fewer measures of health-related quality of life and healthy life expectancy were found.
Overview of data sources
To assess candidate measures that might be scaled up within the established infrastructure and those that might require new investments, the sources of data underlying existing measures were analyzed. The scan identified 3 categories that are commonly used in population health measurement: claims, medical records, and surveys.
Administrative data capturing health service utilization derived from reimbursement are in extensive use for quality reporting, but are inherently limited to an enrolled population accessing health care. All-payer claims databases (APCDs), which aggregate data from nearly all insured residents in a state, provide a more comprehensive picture of population health; however, only 12 states have active APCDs, with 5 additional states in the process of implementation, which limits their usability for national-scale population health measurement. 15
As interoperable health information systems become more widespread, health information exchanges and registries offer additional opportunities to aggregate clinical encounter data across multiple sources. Measures based on electronic health records have the potential to go beyond claims in capturing aspects of the clinical encounter, but will still be derived from face-to-face patient interactions and unable to measure the full range of relevant population-based strategies.
Surveys have an important advantage over claims and encounter data as they capture a wider range of patient-reported variables, including health determinants, behaviors, outcomes (both traditional health and patient-reported outcomes), and use of nonclinical community resources. The research team identified 53 existing surveys and databases commonly used for population health measures (see Supplementary Data; Supplementary Data are available in the online article at
Recommendations to guide the development and testing of measures
Recommendation 1
Population health measures should focus on actionable topic areas within the CMS mission and sphere of influence that will have a meaningful impact on health system transformation. Measure development should prioritize elements of population health in which the clinical care sector is capable of having the most meaningful impact, either independently or in collaboration with the public health and community sectors.
Recommendation 1a
New measures should build on rather than duplicate existing measures within the clinical and public health sectors. Thus, a core measure set should include 1–2 measures in each of 14 population health topic areas (these areas represent a subset of the 22 areas already outlined; the recommendation focuses on filling the gaps). Quality of care, patient experience, and cost are important drivers of population health outcomes, but these are areas with extensive measures already available within the clinical sector; new measures should address those secondary drivers that offer a new opportunity for payers to directly impact health behaviors and social and environmental factors.
Given the small number of existing measures in the clinical context assessing social determinants, measure development for risk assessments should be considered a higher priority. Given the strategic importance of catalyzing multisector collaboration, combined with the gap in existing measures, this area also should be a high priority. Development in these 2 areas could be aligned given that assessment of social determinants and multisector collaboration are closely linked in practice.
Recommendation 1b
A set of core measures should reflect a balance between structure, process, and outcomes, with a priority on using health outcome measures when available. Although there are many measures of health behavior currently being used, almost all reflect process of care rather than outcomes. Examples of outcomes would include weight loss in people with obesity or rates of tobacco use and smoking.
Recommendation 2
Measure development should occur on 2 fronts: established and formative areas. This strikes a balance between measures that can be adapted and incorporated into programs at an accelerated pace and those that (although critical to achieving strategic goals) will require time and investment to develop specifications and address methodological challenges. A key factor in whether existing candidate measures could be adapted or scaled up is the existence of an infrastructure supporting data collection, reporting, and analysis. Several CMS priority areas do not have readily available sources of data, and completing a core population health measure set will require investments in data infrastructure.
Recommendation 3
Separate measures should be developed for each of the target populations relevant to CMS programs and models, as illustrated in Figure 1: patient panels (eg, patients of individual providers), enrolled populations (eg, enrollees in health plans or coordinated care delivery systems), and geopolitically defined populations (eg, communities). To achieve maximum impact, when possible, the measure specifications for each topic should be aligned across the expanding denominators of each target population.
Recommendation 3a
Measures for which the population is a patient panel or enrolled population should leverage data collection platforms in use to support existing clinical quality measurement. New data elements should be added to these systems as necessary, but there are challenges in adapting measures from the public health sector. As the denominator changes from one that is geopolitically defined to one that is defined by association with a health system, the ability to use population-based surveys becomes more limited.
Recommendation 3b
Measures for which the population is geopolitically defined should leverage those existing large-scale federal health-related surveys wherein data are available for analysis at the regional level. These include the Behavioral Risk Factor Surveillance System, the National Health Interview Survey, and the American Communities Survey.
Recommendation 4
Develop use cases to illustrate how population health measures could be applied by CMS and other payers. Because the theory, logic, and practice of population health are not universally known throughout the clinical sector, use cases can provide concrete examples of how population-based strategies and associated measures can drive health improvement. Use case topics should include use of measures for patient panels, enrolled populations, and geopolitically defined populations, as well as measures for multisector collaboration at the individual and community levels.
Discussion
Development of a robust population health measure set has become a priority for payers, providers, and a broad set of stakeholders engaged in improving health outcomes and increasing the value of health spending. 13,16 This emphasis has grown in response to multiple factors, including (1) a recognition that health system measurement could be more effective and efficient through a focus on measures that reflect shared health system priorities and facilitate meaningful comparisons; (2) a shift toward value-based purchasing programs and alternative payment models that hold providers and systems accountable for better care; and (3) the understanding that population health improvement requires multisector and multilevel action, for which existing measurement systems are ill-equipped.
This article presents a foundation for developing a measure set for use by payers that begins to address these gaps. The strategic framework recognizes that the clinical care sector is one critical part of a broader ecosystem of population health that includes other sectors (ie, the public health and community service sectors) and drivers at the individual and community levels (including individual behavior and the social and physical environment). CMS measurement priorities are focused on how the clinical care system accounts for, responds to, and interfaces with this broader set of factors. Therefore, the focus of this article's recommendations is different from recent efforts that are not owned by a particular sector, such as the Robert Wood Johnson Foundation's Culture of Health metrics, which are explicitly focused on tracing upstream social, economic, and policy indicators and take a broader orientation to community health improvement. 12 Nonetheless, the work presented here complements recent measure sets by the Robert Wood Johnson Foundation and the National Academy of Medicine, with a particular focus on how the health care delivery system in general, and payers in particular, can contribute to and measure progress in population health improvement. 11,16
As CMS moves toward population-based payments, the corresponding measures should reflect the same move away from measurement triggered by service delivery and toward measures that reflect CMS interest in holding providers accountable for the health and care of people over an extended period of time. Leveraging the clinical care system to improve population health will require aligning incentives to catalyze new interventions and partnerships. Identifying the appropriate strategies and measuring progress are contingent on developing measurement capacity that does not currently exist in either the clinical or public health sectors.
Through application of its payment and policy levers, CMS has the opportunity to catalyze the formation of partnerships between clinical and other community-based sectors in pursuit of sustainable solutions tailored to the unique needs of each community. Assessing progress toward health system transformation would benefit not only from outcome measures of community well-being but also measures that can inform and evaluate the integration and alignment of services (eg, clinical care, behavioral health, child welfare, social services). In particular, it is helpful to distinguish between service-level and system-level collaboration. Service-level measures will be important for ensuring effective patient-centered care delivery and cross-sector service coordination at the individual level (eg, referrals, data feedback). System-level measures aim to evaluate community-centered program coordination and downstream societal impact by targeting populations. Given the sizable measurement gap in this area, there is opportunity for payers to incentivize a new paradigm of accountability that emphasizes mutually reinforcing measures across multiple levels within a community.
To be useful to payer organizations in driving actionable improvement, population health measures must bridge the gap between provider and facility-based technical measures of clinical quality and community-based measures of health status. Such a set of measures ideally would incorporate the various populations that an individual belongs to into concentrically expanding denominators that reflect meaningful units of analysis at the practice, system, and community levels. The component measures would contain outcomes that are sensitive to delivery system actions and also target populations with clear lines of attribution to the clinical care sector. Using tobacco as an example, Table 3 illustrates how a smoking prevalence measure could be crafted to reflect the percentage of patients who currently smoke within a clinical practice; the percentage of enrollees who currently smoke within an attributed population; and the percentage of the adult population who currently smoke within a geographically defined area such as a county.
This analysis provides a strategic framework for population health measure development and identifies opportunities to adapt existing measures and develop new ones. These results indicate that for measures pertaining to health behaviors, existing measures could serve as a starting point for development and implementation. However, existing measures pertaining to multisector collaboration and upstream determinants were sparse and more intensive de novo measure development work is necessary. The recommendations presented here are designed to contribute to development of a population health measure set that CMS and other payers can use to enhance the clinical delivery system's role in multisector population health improvement.
Footnotes
Acknowledgments
The authors gratefully acknowledge colleagues on the supporting project team led by Arbor Research Collaborative for Health (Arbor Research) in partnership with the University of Michigan School of Public Health (UM-SPH) and Healthcare Management Solutions, Inc. (HMS), those who served as key informants during the development phase, on a technical expert panel to review an early draft, and on a panel of federal partners; all of whom graciously provided valuable insight. Key informant interviews: Helen Burstin, MD, National Quality Forum; Alyna Chien, MD, Boston Children's Hospital; Jennifer DeVoe, MD, Oregon Health Science University; Patrice Holtz, MBA, Karen Llanos, MBA, Karen Murphy, PhD, Cheryl Powell, MPP, and James Poyer, Centers for Medicare & Medicaid Services; David Kindig, MD, University of Wisconsin‐Madison; and Chesley Richards, MD, Centers for Disease Control and Prevention. Technical expert panel: Amy Aronsky, DO, CareCentrix; Lawrence Busch, PhD, Michigan State University; Barbara Gage, PhD, Post-Acute Care Center for Research; Andrew Hertz, University Hospitals Rainbow Babies and Children's Hospital; Sanne Magnan, MD, Institute for Clinical Systems Improvement; Jean McGuire, PhD, Northeastern University; Amy Mullins, MD, American Academy of Family Physicians; Michael Stoto, PhD, Georgetown University; Andrew Suchocki, MD, Clackamas County Health Centers; and Steven Teutsch, MD, Public Health Institute. Federal partners: Agency for Healthcare Research and Quality (Nancy Wilson, MD). Centers for Disease Control and Prevention (John Auerbach, PhD, Peter Briss, MD, Gail Janes, PhD, Denise Koo, MD, Akaki Lekiachvili, MD, and Elizabeth Skillen, PhD). Centers for Medicare & Medicaid Services (Chisara Asomugha, MD, Noni Bodkin, Ashley Corbin, Jayne Hammen, Patrice Holtz, MBA, Jun Li, MSPH, and Shari Ling, MD). Office of the Assistant Secretary for Health (Peggy Honore, DHA, and Betsy Thompson, MD). Arbor Research: Aya Inoue, BA, Robert Merion, MD, Kaden Milkovich, MPA, Jeffrey Pearson, MS, Alyssa Pozniak, PhD, Amanda Szymanski, BA, Francesca Tentori, MD, and Marc Turenne, PhD. UM-SPH: Talha Ali, MS, Carlos Mendes de Leon, PhD, Hal Morgenstern, PhD, and Belinda Needham, PhD. HMS: Christina Compher, MHS, Tina Hammack, and William Ramsey, MD.
Author Disclosure Statement
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. This work was funded by the CMS.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.