
Abstract
Despite patient-centered medical home implementation by the Veterans Health Administration (VHA), delivery of patient-centered care varies across VHA facilities. Facility characteristics underlying this variation are not fully understood. This study used administrative data from 908 VHA outpatient facilities to examine the association of racial and ethnic minority patient concentration and other facility characteristics with facility ratings of patient-centered care. The primary finding was that patient-centered ratings were lower for facilities with medium or high concentrations of Hispanic patients (medium: estimate [Est] = −0.40, standard error [SE] = 0.20, P = 0.046; high: Est = −0.99, SE = 0.23, P < 0.001). In addition, patient-centered ratings decreased as patient panel sizes increased, especially among facilities with higher concentrations of black patients. This study indicates that efforts to improve patient-centered care may be needed at VHA facilities that serve Hispanic and VHA facilities with large panel sizes of high concentrations of black patients.
Introduction
T
Of particular interest is whether facilities serving high concentrations of racial and ethnic minorities are achieving PCMH goals. Within and outside of VHA, health care facilities with higher concentrations of racial and ethnic minority patients tend to deliver lower quality care on multiple measures. 8 –15 Pertaining to the PCMH goal of delivering patient-centered care, studies conducted before VHA PACT implementation reported significant racial and ethnic differences in patient-reported experiences with VHA care that were driven largely by interfacility variation. 16,17 Patterns of racial/ethnic differences in patient experiences were unique for black or African American (subsequently referred to as black), Hispanic, and other racial/ethnic minorities, underscoring the need to focus on the patient-reported components of Pi2 and to disaggregate racial/ethnic groups when possible.
Focusing specifically on the patient-reported components of Pi2, the primary objective of this study was to assess the unique associations of VHA facilities’ concentrations of black, Hispanic, and other racial and ethnic minority patients with facility ratings of patient-reported patient-centered care. In an effort to identify potential ways to ensure equitable delivery of patient-centered care across facilities, this study also examined the extent to which a broad range of facility characteristics explain differences in patient-centered care between facilities with high and low concentrations of black, Hispanic, and other racial/ethnic minority patients. This study represents a critical step in this area.
Methods
A cross-sectional analysis was conducted using facility-level administrative data on VHA outpatient facilities from fiscal year 2013 (FY13: October 1, 2012–September 30, 2013). All evaluation activities were reviewed and approved as quality improvement by the Corporal Michael J. Crescenz Veterans Affairs Medical Center Institutional Review Board.
Sample
The sample included VHA outpatient facilities that (1) were located in the 50 states and Washington, DC, (2) offered primary care services during FY13, (3) had data available on the study outcome of interest, and (4) remained open through FY13.
Study measures and data sources
Study outcome
The study outcome was facility-level delivery of patient-centered care measured using the patient-centered care domains of the Pi2. The full Pi2 was developed by the National Evaluation Team at the VHA PACT Demonstration Laboratory Initiative Coordinating Center to assess the VHA transition to a PCMH model of primary care. 6 Pi2 is calculated from 53 components from patient and provider surveys and administrative data sources that pertain to key PACT initiative goals, including delivery of care that is accessible, continuous, coordinated, team based, and patient centered. The patient-centered component includes care comprehensiveness (ie, attention to mental health issues), self-management support, patient-centered communication, and shared decision making.
As described elsewhere, 6 Pi2 scores are constructed by first calculating a facility score for each of the 53 components. Component scores are standardized across facilities and averaged within 8 domains of care. Facilities are rank ordered for each domain, then assigned a 1 or −1 for every domain for which they are in the top or bottom quartile, respectively, and assigned 0 otherwise. A facility's Pi2 value is the sum of its ranked scores across all domains.
For this analysis, a patient-centered Pi2 score was constructed based on the 4 patient-centered Pi2 domains (Table 1). Data for these domains are from the FY13 PCMH Survey of Healthcare Experiences of Patients, an ongoing survey conducted by the VHA Office of Analytics and Business Intelligence to assess veteran experiences with the VA Healthcare System using the Consumer Assessment of Healthcare Providers and Systems (CAHPS) PCMH survey. 18,19 Previous work has demonstrated adequate internal reliability for CAHPS multi-item scales assessing comprehensiveness (3 items, α = 0.80), communication with providers (6 items, α = 0.93), self-management support (2 items, α = 0.61), and shared decision making about medications (3 items, α = 0.67). 20 The mail-based survey was administered using CAHPS guidelines to a random sample of veterans from all VHA outpatient facilities who received outpatient care from an assigned PACT provider from October 1, 2012, through September 30, 2013. Patient-centered Pi2 was calculated by applying specifications for calculating the full Pi2 to the 4 patient-centered domains. 6 The resulting 9-point scale ranged from −4 to 4, with higher scores reflecting more patient-centered care based on patient surveys at that facility.
Pi2, Patient Aligned Care Team implementation progress index.
Primary predictors
The predictor variables were the concentration of outpatients from non-Hispanic black, Hispanic, and non-Hispanic other racial/ethnic minority groups at each facility. The VHA MedSAS outpatient file from the National Patient Care Database was used to calculate the percent of patients in each group at each facility with at least 1 outpatient visit during FY13 and race/ethnicity data on file. Because of the positively skewed distribution of each minority group, facilities were categorized into tertiles based on their percent of black, Hispanic, and other racial/ethnic patients. The lowest tertile was used as the reference group for each minority group in analyses, comparing facilities with relatively medium or high percentages of each minority group with those with a relatively low percentage.
Additional facility characteristics
This study examined several facility characteristics that could be associated with patient-centered care ratings and/or explain the association between patient racial/ethnic concentration and delivery of patient-centered care. Following Glasgow et al's analytic framework of organizational factors, 21 indicators of 2 broad dimensions of organizational context were selected: facility structure and staffing/culture (Table 2). Facility structure variables included basic, unmodifiable structural characteristics, whereas staffing/culture variables included more modifiable characteristics that may affect the success of a facility's quality improvement efforts. All facility characteristics were drawn from VHA administrative data sources (Table 2).
Facility characteristics were classified according to an analytical framework of factors that determine organizational context. 21 Facility structure includes basic structural characteristics that are generally unmodifiable. Staffing and culture includes more modifiable structural characteristics that may affect the success of quality improvement efforts.
Characteristics were aggregated at the level of parent stations or substations. A parent station is an administrative unit that usually includes a medical center and 2 or more CBOCs. A substation is a component of a station and can be a medical center or a CBOC. Characteristics were aggregated at the substation level whenever possible. For characteristics only available at the parent station level, the parent station value was assigned to all substations within that parent station.
VHA PACT Compass is an electronic dashboard of metrics that reflect the extent to which facilities are successful in providing team-based, continuous, and coordinated care.
CBOC, community-based outpatient clinic; DCG, diagnostic cost group; FY, fiscal year; IOC, independent outpatient clinic; IQR, interquartile range; MD, medical doctor; MOC, mobile outpatient clinic; PACT, Patient Aligned Care Team; SD, standard deviation; VAMC, Veterans Affairs Medical Center; VHA, Veterans Health Administration; VSSC, Veterans Support Service Center.
Statistical analyses
Preliminary analyses were conducted to inform the analytic approach. Specifically, variables were examined for out-of-range values, sparse categories, and high correlations that would indicate multicollinearity. As a result, average patient panel size across providers for each facility was calculated using months with panel sizes within the expected range (500–2000). In addition, because of small numbers, independent outpatient clinics (IOCs, n = 5) were combined with Veterans Affairs Medical Centers (VAMCs, n = 148), and mobile outpatient clinics (MOCs, n = 4) were combined with community-based outpatient clinics (CBOCs, n = 750). For pairs of variables with correlations ≥0.50, only the variable that was more highly correlated with patient-centered Pi2 was included. To aid interpretation of model coefficients, panel size was scaled by 100, patient severity was scaled by 0.10, and all variables were centered before running multivariable models. A likelihood ratio test was conducted to determine whether the study needed to account for the fact that individual VHA facilities are organized into administrative units called parent stations. This test indicated that 21.6% of the variance of patient-centered Pi2 was accounted for by variation between parent stations. Therefore, mixed-effects linear regression models with a random effect for parent station were used for subsequent analyses.
The multivariable analyses proceeded in 3 steps. First, separate mixed-effect models were run to examine associations of each facility characteristic with patient-centered Pi2 scores. This began with a base model containing only the minority concentration variables and random effect for parent station, then other facility characteristics were added that were associated with patient-centered Pi2 scores at P < 0.10 when tested individually. Second, a final multivariable model was constructed that retained the minority concentration variables and other facility characteristics that were associated with patient-centered Pi2 scores at P < 0.05 in the fully adjusted model. The final step was to test for interactions between all minority concentration variables and facility characteristics retained in the final model.
Results
Facility characteristics
Of the 1049 VHA facilities with outpatient activity in FY13, the following were excluded: 11 (1.0%) in outlying areas (San Juan, Manila, Guam, and American Samoa), 96 (9.2%) that did not offer primary care services, 32 (3.1%) without Pi2 scores, and 2 (0.2%) that closed before the end of FY13. Analyses included 908 facilities clustered within 139 administrative parent stations.
Median percentages of black, Hispanic, and other minority patients across facilities were 5.1, 1.6, and 3.4, respectively. Facilities were categorized as having low, medium, or high concentrations of patients from each minority group using the 33rd and 66th percentiles of black (low: <2.3% and high: >10%), Hispanic (low: <0.9% and high: >3%), and other minority (low: <2.6% and high: >4.5%) patient concentration. As shown in Table 3, higher concentrations of black, Hispanic, or other minority patients were significantly associated with higher percentages of female patients and lower percentages of white nurses. Patterns for all other facility characteristics depended on which racial/ethnic group was being considered. For example, employee satisfaction was significantly higher at facilities with greater concentrations of black or other minority patients, but was significantly lower at facilities with greater concentrations of Hispanic patients. Percentage of VAMC and IOC facilities (vs. CBOC and MOC) increased across the low, medium, and high black tertiles, but peaked in the medium tertiles of Hispanic and other minority concentrations. Patient clinical severity increased across the low, medium, and high black tertiles, but was not associated with concentration of Hispanic or other minority patients.
There were 3 variables with missing cases: panel size (n = 11, 1.2%), patient severity (n = 18, 2.0%), and primary care staffing ratio (n = 15, 1.7%). P values are based on comparisons across facilities with low, medium, and high concentrations of each minority group. Analysis of Variance was used to compare means, Kruskal–Wallis tests were used to compare medians, and chi-square tests were used to compare categorical variables.
P < 0.001.
P < 0.05.
P < 0.01.
CBOC, community-based outpatient clinic; DCG, diagnostic cost group; IOC, independent outpatient clinic; IQR, interquartile range; MD, medical doctor; MOC, mobile outpatient clinic; Pi2, patient aligned care team implementation progress; Q1, first quartile (<5990.5 visits); Q2, second quartile (≥5990.5 and <11051visits); Q3, third quartile (≥11051 and <24170.5 visits); Q4, fourth quartile (≥24170.5 visits); SD, standard deviation; VAMC, Veterans Affairs Medical Center; VHA, Veterans Health Administration.
Patient-centered Pi2
Patient-centered Pi2 ranged from −4 to 4, with a mean of −0.01 (standard deviation = 2.29). Patient-centered Pi2 was significantly different across facilities in the low, medium, and high tertiles for each racial/ethnic minority concentration, with facilities in the lowest tertile of each minority group having the highest patient-centered Pi2 (Table 3). The largest difference was observed when facilities were categorized based on Hispanic patient concentration, with mean patient-centered Pi2 scores of 0.57, 0.06, and −0.66 (P < 0.001) in facilities with low, medium, and high Hispanic patient concentrations, respectively. Somewhat smaller differences were observed when facilities were categorized based on concentration of other minority patients (means = 0.42, −0.15, and −0.29 for low, medium, and high facilities, respectively; P < 0.001) or black patients (means = 0.32, −0.17, and −0.18 for low, medium, and high facilities, respectively; P = 0.009).
Modeled associations of black, Hispanic, and other minority patient concentration with patient-centered Pi2
In the multilevel base model, the medium and high tertiles of Hispanic patient concentration were significantly associated with lower patient-centered Pi2 scores (medium: estimate [Est] = −0.40, standard error [SE] = 0.20, P = 0.046; high: Est = −0.99, SE = 0.23, P < 0.001). Black and other minority patient indicators were not associated with patient-centered Pi2 scores in this model (Table 4, Base Model).
Models included a random effect for parent station to account for the clustering of facilities.
P < 0.05.
P < 0.001.
P < 0.01.
Q1, first quartile (<5990.5 visits); Q2, second quartile (≥5990.5 and <11051visits); Q3, third quartile (≥11051 and <24170.5 visits); Q4, fourth quartile (≥24170.5 visits); Pi2, Patient Aligned Care Team implementation progress index; SE, standard error.
Based on preliminary analyses, the following variables were added to the base model to determine whether they explained the association of Hispanic patient concentration with patient-centered Pi2 scores: percentage of female patients, number of primary care visits, patient panel size, patient severity, percentage of white medical doctors, and employee job satisfaction (data not shown). Of these, patient panel size, patient severity, and number of annual primary care visits were retained in the final model as these remained significantly (P < 0.05) associated with patient-centered Pi2 scores in the fully adjusted model.
In the final model (Table 4, Final Model), the medium and high Hispanic tertiles remained significant predictors of patient-centered Pi2 scores (medium: Est = −0.40, SE = 0.19, P = 0.040; high: Est = −0.95, SE = 0.23, P < 0.001). In other words, facilities in the medium and high tertiles of Hispanic patient concentration had patient-centered Pi2 scores that were 0.40 and 0.95 points lower than facilities with the lowest concentration of Hispanic patients. Facilities with larger panel sizes also exhibited worse patient-centered Pi2 scores than facilities with lower panel sizes, such that patient-centered Pi2 was reduced by 0.12 points for every increase of 100 patients in average patient panel size among primary care providers. However, patient-centered Pi2 scores increased by 0.26 for every 0.10 increase in the average clinical severity of patients. Finally, facilities in the second smallest volume quartile had patient-centered Pi2 scores that were 0.54 points higher than facilities in the lowest quartile of primary care visits.
Interactions between minority patient concentration and other facility characteristics
This study explored all potential 2-way interactions between each minority patient concentration indicator and patient panel size, patient severity, and annual number of primary care visits (data not shown). There were significant interactions between panel size and the medium and high black tertiles (medium: Est = −0.15, SE = 0.07, P = 0.046; high: Est = −0.19, SE = 0.08, P = 0.015). To interpret these interactions, the predicted patient-centered Pi2 scores were plotted for facilities with low, medium, and high concentrations of black patients at the mean patient panel size and at 1 standard deviation above and below the mean (Fig. 1). The figure illustrates that among facilities with low percentages of black patients, patient-centered Pi2 scores are slightly lower (−0.15 points) in facilities with patient panel sizes 1 standard deviation below (vs. above) the mean. The difference is much larger among facilities with medium (−0.85 points) or high percentages (−1.03 points) of black patients.
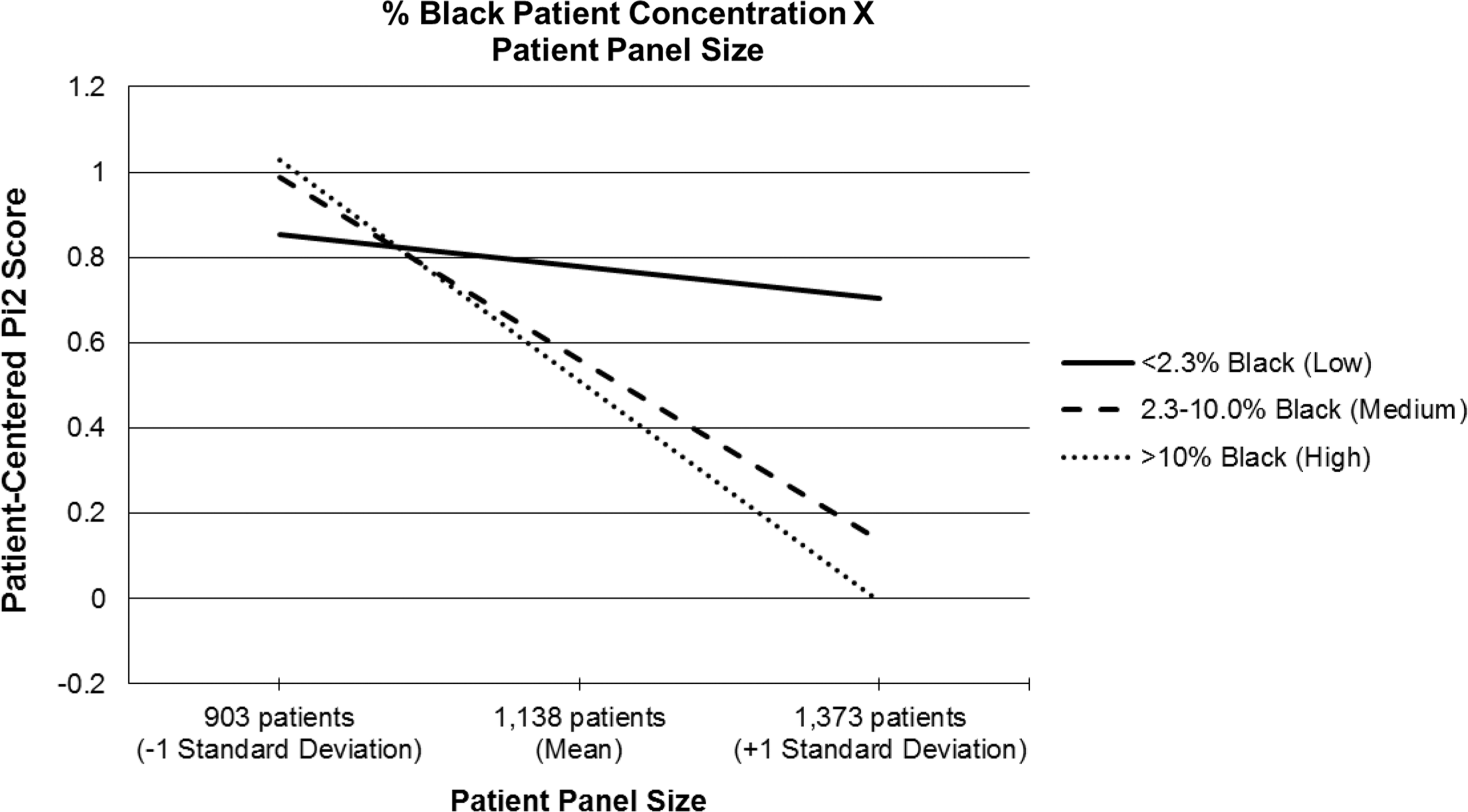
Patient-centered Pi2 scores for facilities with low, medium, and high concentrations of black patients at the mean patient panel size (1138 patients), as well as at 1 standard deviation above (1373 patients) and below (903 patients) the mean. Pi2, Patient Aligned Care Team implementation progress index.
Discussion
In this study of VHA facilities that have undergone primary care transformations to implement the PCMH model, ratings of patient-centered care were ∼0.5–1 point lower on a 9-point scale at facilities serving higher concentrations of Hispanic patients and at facilities with a combination of higher concentrations of black patients and larger panel sizes. Although many factors contribute to racial and ethnic disparities in health care, 22,23 this study contributes to a body of work showing that segregation of racial and ethnic minority patients in relatively low-performing facilities may underlie and perpetuate disparities. 8 –17,24,25
Most prior studies showing that racial and ethnic disparities in health care occur because of differences in facilities where minority and nonminority patients get care have focused on quality of care metrics in inpatient settings. 8 –15,24,25 Fewer studies have examined the association of patient racial and ethnic concentration with patient-reported experiences in the outpatient setting, as was the focus of the present study. 16,26 –28 Addressing this gap is important given that access to high-quality outpatient primary care is recognized as essential for maintaining health and health equity 29 and there continue to be racial and ethnic disparities in primary care access and utilization. 30
The PCMH model is thought to be a potential mechanism to reduce racial and ethnic disparities. 31 –33 For the PCMH model to meet the needs of racial and ethnic minority patients, however, it must be well implemented in facilities serving high concentrations of minority patients. Outside the VHA, some racial and ethnic minority groups remain less likely than whites to receive care from providers with PCMH characteristics. 34,35 Within VHA, one study using Pi2 scores from 2012 found that facilities serving a higher percentage of non-white veterans were struggling with PACT implementation overall. 36
Focusing on the patient-reported components of Pi2 from 2013, and disaggregating the racial/ethnic groups, the present study shows that a facility's concentration of Hispanic, but not black or other minority, patients is associated with patient-centered Pi2. This study was unable to identify any facility characteristics that explained differences in patient-centered care between high, medium, and low-Hispanic VHA facilities, despite examining a broad range of variables pertaining to facility structure, staffing, and culture. These results suggest that targeted efforts are likely needed to improve patient-centered care at VHA facilities with relatively high proportions of Hispanic patients. To identify specific strategies to improve patient-centered care at Hispanic-serving facilities, it may be necessary to go beyond what can be ascertained from administrative data by conducting site visits or interviewing patients and providers at those facilities. One factor that could be explored is the presence and impact of language barriers. On the same survey used to calculate this study's facility-level rating of patient-centered care, it was found that 15% of Hispanic veteran respondents reported that they spoke a language other than English at home (vs. <2% of veterans in the sample overall). The higher prevalence of non-English speakers among the Hispanic veteran population calls for additional research on whether language barriers interfere with the delivery of patient-centered care at facilities that serve Hispanics.
This study identified additional facility characteristics that were independently associated with patient-centered care, one of which may provide a modifiable target to improve patient-centered care overall. In particular, patient-centered scores were lower at facilities with larger patient panel sizes, especially at facilities with higher concentrations of black patients. Taking steps to decrease the average patient panel size of providers (eg, by increasing staffing levels) may increase patient-centered care, with the greatest potential benefits likely being at facilities serving more black patients. Other facility characteristics associated with patient-centered care in this study (ie, clinical severity of patients, overall primary care volume) would be more difficult to modify.
This study has limitations. The main predictor was the racial and ethnic concentration of patients at facilities as documented in electronic medical records. This may have undercounted Hispanic and other minority patients. 37,38 By relying on administrative data, the study also was limited in the facility characteristics that could be included in the analyses. Finally, no conclusions could be drawn about causal relationships because of the cross-sectional nature of this analysis.
Conclusion
Although the PCMH model has been seen as having potential to reduce disparities, a reduction of disparities has not been an explicit target or a routinely monitored outcome in PCMH initiatives. 39 This study demonstrates that patient-centered care in VHA facilities where the PCMH model has been implemented is lower among facilities that serve more Hispanic patients and in facilities with large panel sizes that serve large numbers of black patients. Moving forward, steps are needed to ensure that the PCMH goal of delivering patient-centered care is being achieved successfully across all VHA facilities, regardless of the racial and ethnic composition of their patient populations.
Footnotes
Acknowledgments
This work was undertaken as part of the Veterans Administration's PACT Demonstration Laboratory initiative, supporting and evaluating Veterans Affairs transition to a patient-centered medical home. The views expressed here are those of the authors and do not represent those of the Department of Veterans Affairs or the US Government. Preliminary findings from this work were presented at the VA HSR&D/QUERI National Conference in 2016.
Author Disclosure Statement
Drs. Hausmann, Gao, Jones, Long, and Werner, Ms. Canamucio, and Ms. Keddern declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received financial support from the VA Office of Patient Care Services (XVA 72-065; Coprincipal Investigators Drs. Werner and Long).