
Abstract
The purpose of this study was to assess the impact of a program to prevent the development of type 2 diabetes among participants with prediabetes. The program focused on a healthy eating style, behavior modification, daily physical activity, and achieving a healthy weight. This was a retrospective observational analysis of a pilot program designed to prevent diabetes among employees with prediabetes. This intervention involved 12–16 weeks of nutrition counseling with the registered dietitian and participation in physical activity of at least 150 min/week. The primary outcome for this study was the prevention of type 2 diabetes. Secondary outcome measures included changes in the following biometrics: body mass index (BMI), systolic blood pressure (SBP), diastolic blood press (DBP), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total cholesterol, waist circumference, and triglyceride levels. The diabetes prevention intervention was associated with significant improvements in glucose (−6.6%), A1c (−2.9%), weight (−5.5%), BMI (−5.5%), SBP (−4.9%), DBP (−3.9%), total cholesterol (−5.0%), LDL-C (−7.0%), and triglycerides (−13.9%). After the 12–16-week intervention, the prevalence of prediabetes was reduced by 31% by fasting blood glucose or A1c levels. Baseline A1c, baseline glucose level, age, and number of sessions attended were all significant predictors of the odds of transitioning out of the prediabetes stage, controlling for all other covariates in the model. This pilot study suggests that the implementation of a worksite diabetes prevention intervention can help employees transition from a prediabetes status to no risk of diabetes.
Introduction
I
The Diabetes Prevention Program was a large prevention study of people at high risk for diabetes. In the lifestyle intervention, the goal was to reduce 7% of initial bodyweight and to exercise for 150 min/week. Participants attended 16 one-on-one personalized sessions with a curriculum focusing on diet, exercise, and behavior modifications over a 24-week period. The study showed that lifestyle intervention that resulted in weight loss and increased physical activity in the population can prevent or delay type 2 diabetes and in some cases return blood glucose levels to within the normal range. The incidence of diabetes was reduced by 58% with the lifestyle intervention and by 31% with metformin, as compared with placebo, reported over an average of 2.8 years after the original intervention. 6
Several studies, modeled after the large-scale Diabetes Prevention Program, have shown the benefits of a program focusing on intensive lifestyle modification. 7 –14 One study, in which participants were randomized to an intensive lifestyle modification, showed that meeting the 7% weight loss goal through a hypocaloric low-fat diet and 150 min/week of moderate-intensity physical activity was strongly correlated with the prevention of diabetes in both sexes. 13 In an educational intervention on achieving diabetes control, the intervention group reported a trend toward achieving a significant mean reduction in A1c with 49% (P = 0.06) higher odds of reaching glycemic control and a 0.12 (P = 0.06) greater absolute percentage point drop in A1c compared with the no education group. 11 In another study of a population at high risk for developing type 2 diabetes who underwent intensive lifestyle change, 6-month weight loss predicted lower 3-year diabetes risk in a graded manner. 12 Furthermore, a lifestyle intervention study showed that changes in nutrient uptake were maintained for up to 9 years. 10 A systematic review showed that multicomponent lifestyle interventions in adult populations with prediabetes were effective at modest weight loss and small improvements in glycemic control along with improvements in physical activity and diet. 7 In another systematic review and meta-analysis, 16 and 24 sessions were as effective as programs of shorter duration, and attrition was unrelated to program length but rather was related to participants' perceptions of how likely they were to develop diabetes and the effectiveness of behavioral techniques. 8 A community-based 16-week diabetes prevention program showed weight loss maintained 6 months after the program. In this program, however, participants also felt a lengthy program was necessary to change habits. 9 In a diabetes prevention program among Native Americans that consisted of 16 education sessions plus lifestyle coaching, program participants increased their intake of healthy foods (ie, whole grains, low-fat meats, fruits, and vegetables) and significantly decreased their intake of unhealthy foods, most notably high-fat meats, baked goods and pastries, soft drinks, fried potatoes, and fast foods. 14 Diabetes prevention programs can not only reduce risk of diabetes but also can reduce risk of cardiovascular disease. 13
Worksite wellness programs offer convenience and accessibility, which is important in preventing attrition and improving effectiveness of disease prevention programs. Worksite programs also have the potential to reduce medical costs, absenteeism, and future costs. 15 A review found that almost all workplace lifestyle interventions achieved small but significant changes in physical activity, fitness, dietary behavior, or weight. Programs focusing on targeted goals (ie, weight management) were more successful. 16 In one community-based study, participants stressed the importance of accessibility in a diabetes prevention program. 17 Another study demonstrated that a 12-week, worksite, multicomponent, intensive lifestyle intervention conducted among high-risk employees was successful in improving the cardiometabolic profile of participants at the end of the intervention. In addition, many of these improvements including reduction in body mass index (BMI) were maintained at 1 year. 18 A 16-week group-based lifestyle intervention delivered at a university worksite facilitated reductions in body weight among employees with prediabetes. These results support the efficacy and benefits of worksite interventions for risk reduction. A group delivery format reduces personnel demands and increases employee cohesion and support. 19
The purpose of this study was to assess the impact of a worksite program to prevent the development of type 2 diabetes among participants with prediabetes (fasting blood glucose between 100 and 125 mg/dL and/or an A1c between 5.7% and 6.4%). The program focused on healthy eating style, behavior modification, daily physical activity, and achieving a healthy weight.
Methods
Study design and setting
This was a retrospective observational analysis of a pilot program designed to prevent diabetes among employees with prediabetes. The diabetes prevention intervention was conducted 3 times intermittently over the years 2012 and 2013. Two of these interventions were conducted in group sessions, and 1 was conducted in individual sessions where participants met one-on-one with the registered dietitian or diabetes educator. The pilot programs spanned 12–16 weeks and were offered to employees of a large utility company who had prediabetes. The goal of the diabetes prevention program was to encourage a healthy lifestyle change to prevent the development of type 2 diabetes. Lifestyle changes included promoting a healthy eating style, physical activity, and weight loss. During the time of this pilot study, there was no control group. This study was reviewed and approved by Quorum Institutional Review Board.
Screening and enrollment
The diabetes prevention program was available to the utility company employees, spouses, and dependents (16–26 years old) covered by the company's medical plan who had been identified to have prediabetes by a health care provider. Prediabetes was identified as either having a fasting blood glucose between 100 and 125 mg/dL and/or an A1c between 5.7% and 6.4%. Participants also could enroll in the program if they received a clinical recommendation by the on-site health and well-being medical staff. Interested employees responded to an advertisement by contacting the worksite health center to schedule a “screening” appointment with the registered dietitian. During this free consultation, the registered dietitian evaluated the employee's readiness and eligibility. A screening form was used to determine eligibility to join the diabetes prevention program and readiness for change. The screening tool also measured whether employees were willing to make a commitment to participate in activities, such as taking time for exercise at least 150 min/week, and to make healthy dietary changes for the long term. No distinction was made between high level and low level of readiness. Instead, the focus was on whether employees met the eligibility criteria (ie, a fasting blood glucose between 100 and 125 mg/dL or A1c between 5.7% and 6.4%). Participants also were eligible to join the program if their physician recommended them based on their medical history.
Intervention
Participants attended weekly sessions conducted by a registered dietitian (or diabetes educator) for 12–16 weeks. Sessions focused on a healthy eating style, behavior modification, and daily physical activity. More specifically, the program focused on (1) carbohydrate counting, (2) mindfulness, (3) avoidance of sugar-sweetened beverages, (4) wholesome meals, (5) fruits and vegetables, (6) regular physical activity (at least 150 min/week or 10,000 steps per day), and (7) the plate method. The plate method stresses eating balanced low-fat meals, eating less salt, and avoiding sugary foods. Participants who completed the program were offered monthly sessions with the registered dietitian for the following 3 months and then once a quarter for up to 1 year.
As a pilot study, this diabetes prevention program was offered at no cost to participants. Labs at the beginning and end of the program also were provided at no charge. The diabetes prevention intervention provided a comprehensive physical examination that included laboratory testing and biometric measurements. Active participants also received free fitness center memberships, pedometers, and other tools to assist with making healthy lifestyle changes.
Outcomes
The primary outcome for this study was the prevention of type 2 diabetes. Given that the main inclusion criterion for this study was prediabetes, the transition of patients out of this risk category was the desired outcome. Secondary outcome measures included change in the following biometrics: BMI, systolic blood pressure (SBP), diastolic blood press (DBP), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total cholesterol, waist circumference, and triglyceride levels. Blood draws were performed with the patient fasting. This study did not focus on measuring the effects of lipid-lowering drugs or blood pressure medications. However, anyone on hypoglycemic agents, such as metformin, was excluded from this population.
Statistical analysis
This analysis sought to determine the impact of the diabetes prevention intervention on the likelihood of transitioning from the prediabetes risk category to no risk. The covariates considered in the models were sex, age, number of diabetes educational sessions (a proxy for program duration), and type of program (individual vs. group). The influence of changes in weight, BMI, waist circumference, SBP, DBP, HDL-C, LDL-C, triglyceride levels, and total cholesterol levels also was assessed. In addition to the multivariable model explaining risk transition, univariate and bivariate statistics are also presented. Added focus was placed on the changes in biometric measures pre- and postintervention. Generalized linear models were used for these biometric evaluations and P values were adjusted because of multiple testing. Logistic regression was used to measure the influence of covariates, and repeated measures regression using generalized estimating equations was used to assess longitudinal changes in biometric measures. Hochberg's step-up method multiple testing was used. Missing data were imputed using multiple imputation missing data methods. 20,21 Data were analyzed using SAS/STAT software (SAS Institute, Inc., Cary, NC).
Results
A total of 81 employees participated in the diabetes prevention program, and 56% were female. Approximately 20% were between ages 20 and 39, 62% between ages 40 and 59, and 18% between ages 60 and 79. A third of the participants attended educational sessions ≤9 weeks, 42% attended 10–12 weeks, and 25% attended 13–16 weeks. Fifty-nine of the 81 participants (72.8%) completed the program.
Baseline biometrics of program participants are shown in Table 1. At completion of the program, the participants reduced both their weight and BMI by a relative mean of 5.5%, but waist circumference was reduced by only 1.5%. These and additional biometric improvements are shown in Figure 1.
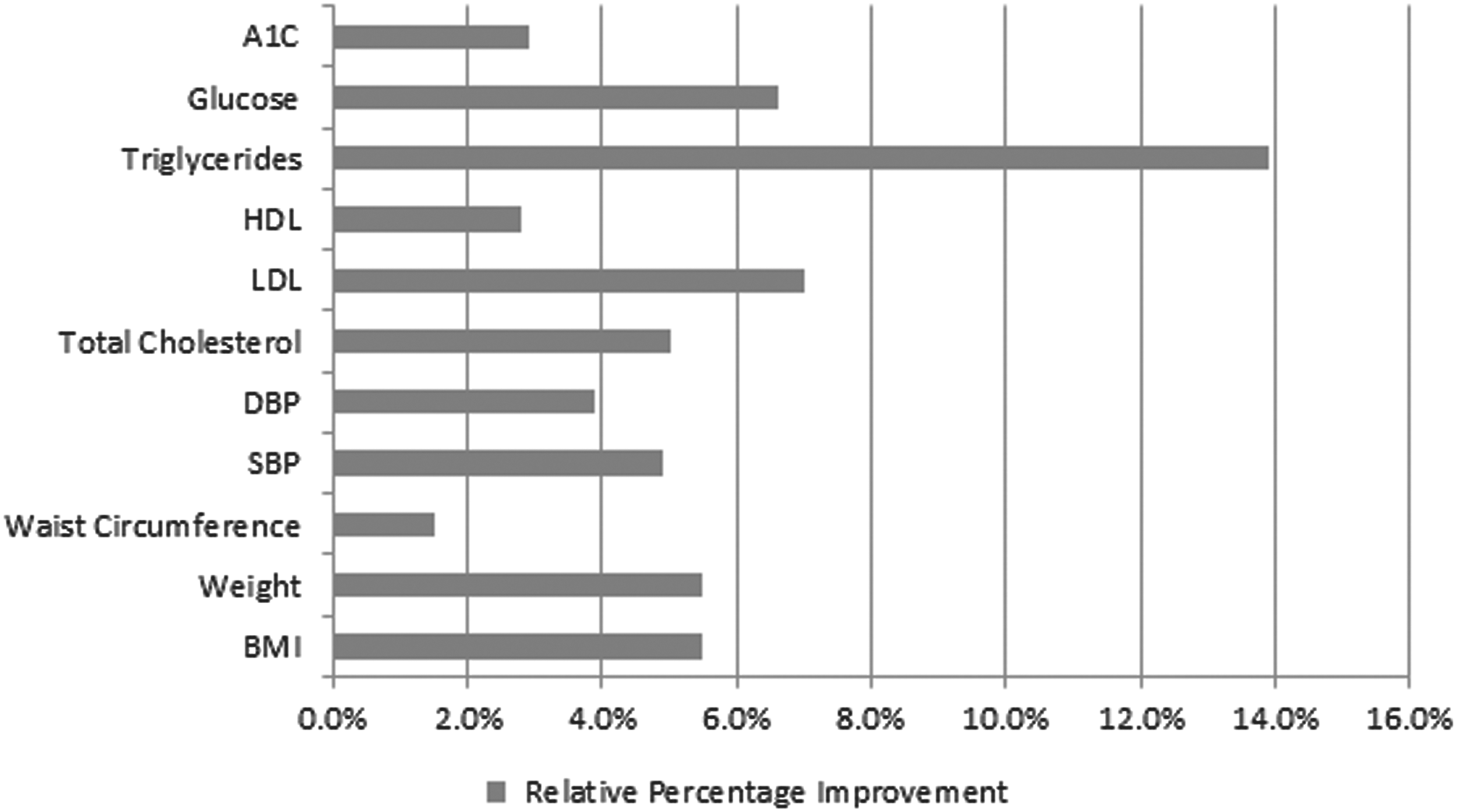
Improvement in biometrics after a diabetes prevention intervention. BMI, body mass index; DBP, diastolic blood pressure; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol; SBP, systolic blood pressure.
BMI, body mass index; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; TG, triglycerides.
Among the participants who had prediabetes and completed the study (59/81), 31% (18/59) improved and thus transitioned out of the prediabetes stage. Fifty-four percent of participants who transitioned out of the prediabetes stage attended 9–12 weekly sessions and 34% attended 13–16 weekly sessions. Sixty percent of these patients were between the ages of 40 and 59 and 25% were between ages 60 and 79.
In the univariate models used to further describe the data, all biometric measures showed statistically significant changes from baseline to post diabetes prevention intervention at the P < 0.05 significance level, except waist circumference and HDL-C (Table 2). Triglyceride levels, weight, and total cholesterol were most impacted by the diabetes prevention intervention.
Hochberg adjusted P values.
BMI, body mass index; CI, confidence interval; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; TG, triglycerides.
Multivariable regression models were used to assess the impact of all biometric measures on transitioning out of the prediabetes stage to the no-risk stage. Only baseline A1c displayed a significant impact on transitioning out of the prediabetes stage (Table 3, Model 1). Both the baseline measures of each biometric and the change in baseline measure were included in this model. A separate model assessed the impact of age, sex, type of diabetes prevention session (individual or group), and number of sessions attended, along with baseline A1c and baseline glucose (Table 3, Model 2). Of the 6 covariates, baseline A1c, age, and number of sessions were significant predictors of transitioning out of the prediabetes stage after the diabetes prevention intervention. A final model shows that age and number of sessions attended, along with baseline glucose and baseline A1c, are all significant predictors of transitioning out of the prediabetes stage after the diabetes prevention intervention (Table 3, Model 3). Participants of younger age and those who attended a greater number of sessions were associated with a greater likelihood of transitioning out of the prediabetes stage.
BMI, body mass index; CI, confidence interval; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; TChol, total cholesterol; TG, triglycerides. Numbers in italics are P < 0.05.
Discussion
The purpose of this analysis was to evaluate the effectiveness of this pilot worksite diabetes prevention program in transitioning employees with prediabetes to a no-risk diabetes stage. A secondary aim was to improve SBP, DBP, BMI, weight, waist circumference, LDL-C, HDL-C, triglycerides, total cholesterol, glucose, and A1c.
Primary findings
The primary findings from the current diabetes prevention pilot study showed that patients who enrolled in this program can reduce their risk for diabetes. Before the intervention, 94% of the participants had prediabetes (those participants who did not have prediabetes joined the program based on their medical history and a recommendation by their physician), but after the intervention only 69% (41/59) had prediabetes. The diabetes prevention intervention also was associated with significant improvements in glucose (−6.6%), A1c (−2.9%), weight (−5.5%), BMI (−5.5%), SBP (−4.9%), DBP (−3.9%), total cholesterol (−5.0%), LDL-C (−7.0%), and triglycerides (−13.9%). No patient's diabetes condition worsened; that is, progressed from prediabetes to the diabetes stage. Both baseline A1c and baseline glucose level were significant predictors of the odds of transitioning out of the prediabetes stage, controlling for all other covariates in the model. The age of the participant and the number of educational sessions attended also were significant predictors. Younger participants and those attending more sessions were more likely to transition out of the prediabetes range for fasting glucose and A1c.
Congruence with the literature
Akin to findings by the Diabetes Prevention Program Research Group that showed that lifestyle interventions had 58% fewer cases advance than the control group, the results of this study suggest that a lifestyle intervention can reduce the prevalence of prediabetes by 30% within a 16-week intervention period. 6
An analysis of a community diabetes prevention program by Kramer et al reported that body weight decreased by 5.5% at 1 year, BMI decreased by 5.5%, fasting glucose decreased by 4.6%, triglycerides decreased by 14.4%, SBP decreased by 6.1%, and DBP decreased by 8.2%. 22 A study by Dallam and Foust also showed mean improvements in BMI and weight. 23 However, unlike this study, Kramer et al showed significant improvements of 6% in waist circumference and 4.3% in HDL-C, but no significant improvements were evident for total cholesterol or LDL-C. 22 Unlike the Dallam and Foust study, the results of this study showed no differences between the implementation of a one-on-one intervention and a group intervention, controlling for biometric and demographic factors. 23
Limitations
This pilot study also suffered from a few notable limitations. The primary limitation was the lack of a control group to compare the results of the diabetes prevention intervention and thus to control for bias by doing a propensity score matching analysis. Yet, multivariable analysis was used to adjust for confounding factors, especially the baseline values of glucose level and A1c. Second, given that this was a pilot study, the sample size was relatively small. However, this sample size of 81 provided a rich data source and thus allowed for an adequate investigation. Third, a number of participants did not complete the program, yet the completion rate was 73% and higher than a similar published pilot study by Kramer et al (64%). 22 To account for the missing data, though, this study used multiple imputation analysis to predict the missing values. Finally, this study was not long term (3–4 years), but other studies have shown that weight and glucose at 6 and 12 months strongly predict lower subsequent diabetes risk with a lifestyle intervention. 10,12,18 In other words, early results are predictive of long-term results.
Because this sample was neither randomized nor randomly selected, the results are not generalizable. Nonetheless, this pilot study met its purpose by showing the potential implementation of a full-scale worksite diabetes prevention intervention.
Conclusion
Despite these limitations, this pilot study suggests that the implementation of a worksite diabetes prevention intervention focusing on lifestyle changes can help employees transition from a prediabetes status to no risk of diabetes.
Because it was observed that those who attended a greater number of sessions were more likely to transition out of the prediabetes stage, a worksite diabetes prevention program may be a convenient environment for employees to attend such programs because of ease of access. Additional benefits for the employee may include improvements in cardiovascular risk factors such as improvements in lipid levels and lower blood pressure. The benefit to the employer may include decreased absenteeism, improved productivity, and overall lower health care costs. 5,15
Footnotes
Author Disclosure Statement
Dr. Clark, Ms. Boghani, Ms. Grullon, and Ms. Batista declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received no financial support for this article.