
Abstract
Thirty-seven percent of US adults have prediabetes. Various interventions can delay diabetes progression; however, the optimum target group for risk reduction is uncertain. This study estimated rate of progression to diabetes at 1 and 5 years among a cohort of patients from 3 primary care clinics and modeled the potential magnitude in diabetes incidence risk reduction of an intervention program among specific subgroups. Records of 106,821 empaneled patients in 2005 were reviewed. Generalized population attributable risk (PAR) statistics were calculated to estimate the impact of reducing fasting blood glucose on diabetes progression. Multiple intervention effects (varying levels of glucose reduction along with multiple adherence rates) were examined for those with baseline glucose from 110 to 119 mg/dL and ≥120 mg/dL. Ten percent of patients (n = 10,796) met criteria for prediabetes. The 1- and 5-year diabetes incidence rate was 38.6 and 40.24 per 1000 person-years, respectively. Age and obesity were independent predictors of increased progression rate. The generalized PAR for a 10-point reduction in the 110–119 mg/dL subgroup with 25% adherence was 7.6%. The generalized PAR for similar percent reduction and adherence level in patients with baseline glucose of ≥120 mg/dL was only 3.0%. Rate of progression to diabetes increased over time and with associated independent risk factors. Greater risk reduction in diabetes progression within the target population can be achieved when the intervention is successful in those with baseline glucose of 110–119 mg/dL. Modeling an optimum target group for a diabetes prevention intervention offers a novel and useful guide to planning and allocating resources in population health management.
Background
I
Regardless of what diagnostic criteria are used to define prediabetes, it remains universally recognized as a high-risk state for diabetes development. Observational studies also have shown associations between prediabetes and the development of chronic kidney disease, small fiber neuropathy, and macrovascular diseases. 5 –8 However, progression to diabetes can be delayed by various interventions 9 and regression to normal glucose regulation is even attainable with lifestyle interventions. The US Diabetes Prevention Program (DPP), a large study aimed at preventing or delaying type 2 diabetes onset in high-risk adults with both impaired glucose tolerance and elevated fasting glucose, reported a 58% cardiovascular disease risk reduction after interventions aimed at weight loss, dietary change, and increased physical activity. 10 –12 Evidence from DPP indicated that preventive interventions are effective in groups of people with HbA1c levels both below and above 5.9%. 11
From a population health standpoint, much debate still exists about whom to target with diabetes prevention interventions and what parameter best predicts the progression to diabetes. Most programs have targeted high-risk individuals based on HbA1c; however, recent publications have shown impaired fasting glucose—and not HbA1c—to be associated with a higher risk for progression to diabetes. 13,14 In a meta-analysis of 70 studies, Morris et al suggested that an HbA1c range of 6.0%–6.4% tends to identify people who are at a lower diabetes risk and that other prediabetes definitions might better identify high-risk individuals. 15 Relying solely on HbA1c also may underestimate prediabetes prevalence in certain ethnic populations. 16 A recent systematic review concluded that treatment based on impaired fasting glucose rather than HbA1c was associated with delayed progression to diabetes. 9 Hence, the question of where to direct diabetes prevention interventions within this high-risk population group to potentially achieve its optimum effect in risk reduction remains unanswered.
As the focus of primary care shifts toward population health, it is essential to characterize patients with prediabetes and the rate of progression to diabetes. More importantly, it is crucial to identify specific subgroups that can be targeted for diabetes prevention interventions to maximize the benefit within a population served and to allocate resources appropriately. To this end, the present study was conducted to determine the prevalence of prediabetes among patients served by primary care practice clinics of an academic institution in the Midwestern United States, to estimate the rate of progression to diabetes at 1 and 5 years among these patients, and to estimate the potential magnitude in diabetes incidence risk reduction of a hypothetical intervention program.
Methods
A retrospective cohort study was conducted using data from patients empaneled to a primary care provider in 2005. Three primary care sites were included in this study: primary care internal medicine, family medicine, and general internal medicine (known as area general internal medicine in 2005). Eligibility criteria included all empaneled patients aged 20 years or older and considered to have prediabetes in 2004 or 2005. Prediabetes has been diagnosed in adults as young as age 20 years 5 and is defined by the American Diabetes Association as either having a fasting glucose level between 100 and <126 mg/dL or an HbA1c level between 5.7% and 6.4%. 17 For this study, an HbA1c cutoff of between 6.1% and 6.4% was chosen because the laboratory's reference range for normal HbA1c in 2004–2005 was up to 6.0%. Patients were excluded if they did not provide permission for their records to be used for research, did not have any laboratory measurements during 2004–2005, or if they had prevalent diabetes. Prevalent diabetes was defined as receiving at least 2 International Classification of Diseases, Ninth Revision (ICD-9), codes for diabetes at least 30 days apart between 2000 and 2004, having a fasting glucose level of 126 mg/dL or higher, or an HbA1c ≥6.5. Laboratory result values that were not obtained in the outpatient setting or occurred during a pregnancy also were excluded.
Study population/data collection
A total of 106,821 patients were empaneled to one of the 3 primary care practices in 2005. Of the 99,994 (93.6%) patients who gave research authorization, 65,782 had glucose or HbA1c measurements within the time period. A total of 7139 patients with prevalent diabetes were excluded. The study cohort consisted of 10,796 patients with prediabetes, 5595 of whom had prevalent (preexisting) prediabetes in 2005 and 5201 of whom had incident prediabetes in 2005 (Fig. 1). Demographic and clinical characteristics were captured at baseline (January 1, 2005) and included age, sex, race, clinic affiliation, body mass index, and baseline glucose laboratory values. Patients were followed from their date of laboratory measurement that defined prediabetes or January 1, 2005, whichever was later, until last follow-up in December 2014 or receipt of a laboratory value indicating diabetes.
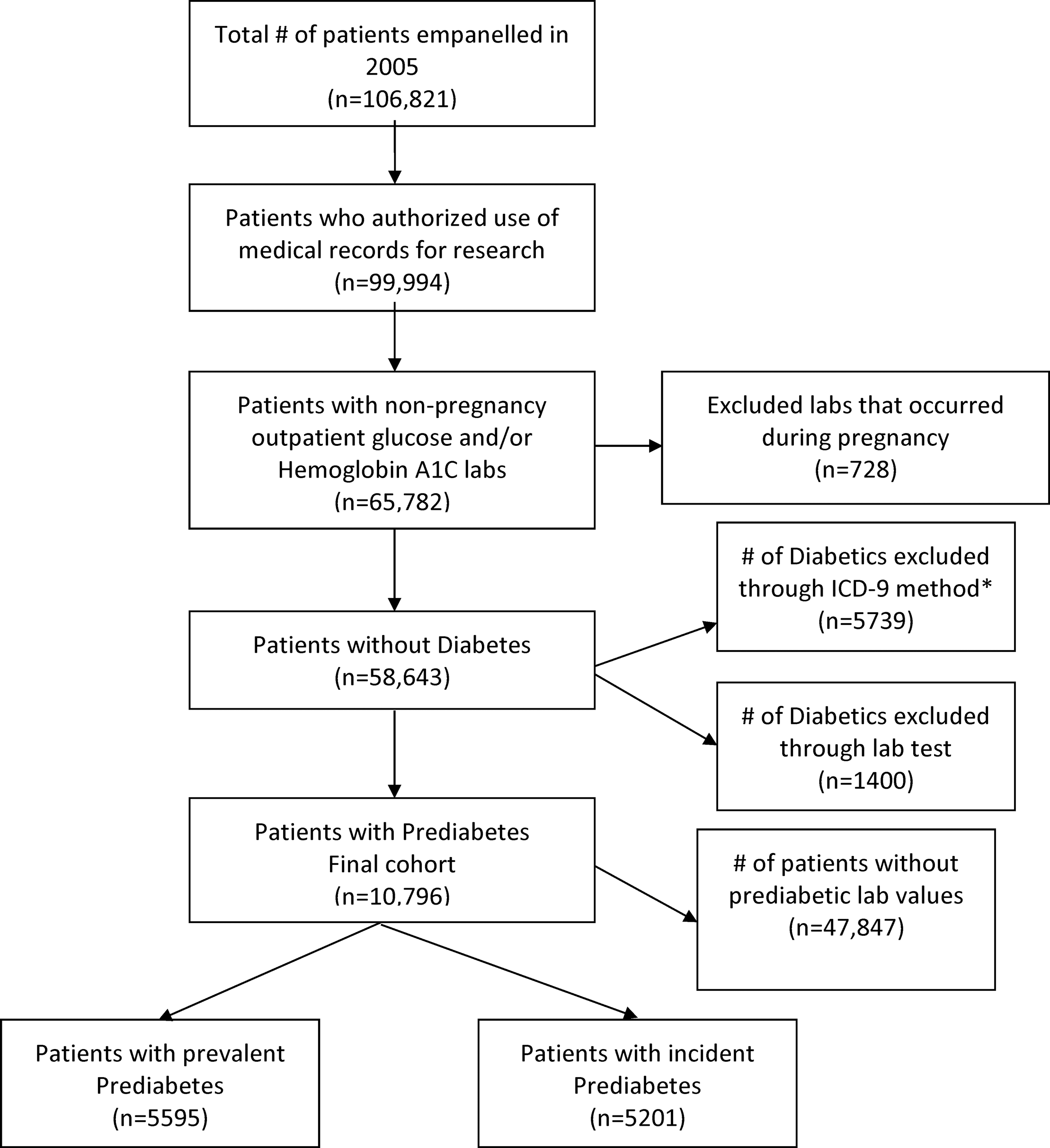
Flow diagram of prediabetes cohort. ICD-9, International Classification of Diseases, Ninth Revision.
Statistical analyses
Baseline characteristics of patients with prediabetes were described using estimates of frequencies for categorical variables and medians and interquartile ranges for continuous variables. The international classification of adult underweight, overweight, and obesity according to body mass index was used. 18 Rates of progression to diabetes (counts per 1000 person-years) were calculated for 1 and 5 years of follow-up. Poisson regression models were used to compare rates of progression across levels of age, race, sex, body mass index, and baseline glucose laboratory value, and results are presented as incidence rate ratios (IRRs) 19 along with 95% confidence intervals (CIs). Multivariable Poisson regression models were used to adjust for all variables. Generalized population attributable risk (PAR) statistics were calculated to estimate the impact of reducing fasting blood glucose on the progression from prediabetes to diabetes in this cohort. PAR, which is defined as the reduction in incidence that would be achieved if the population had been completely unexposed, 20 has important population health implication because it assesses thresholds for policy interventions by taking into account the relative risk of progression to disease as well as the prevalence of the exposure in the population. It has been used in population health research to quantify the contribution of risk factors to disease burden. 21 However, requiring complete removal of the exposure is unrealistic and limits the usefulness of the PAR; therefore, a generalized PAR was assessed, also referred to as the impact fraction. 22 A generalized PAR can provide realistic expectations of the effect on reduced progression to diabetes related to interventions that lead to a reduction in blood glucose level in persons with prediabetes.
All generalized PAR statistics were computed using the Attribrisk Package (version 0.1, Schenck et al 2014, Rochester, MN), with a modification to use Poisson models with person-years as an offset. Briefly, a target data set reflecting each hypothetical intervention was created. Incidence of diabetes (progression) was modeled using Poisson regression. Poisson model estimates were then applied to each target data set to reflect the difference between the observed incidence in the population and the expected incidence had the intervention occurred. Multiple intervention effects (reduction of glucose level by 5, 10, 15, and 20 units mg/dL) along with multiple rates of adherence (10%, 25%, and 50% of the population) were examined for those with baseline glucose levels from 110 to 119 and ≥120 mg/dL. Variance and 95% CIs were calculated using the nonparametric bootstrap. All analyses were performed using SAS 9.4 (SAS Institute. Inc., Cary, NC) and R 3.0.2 (R Foundation, Vienna, Austria).
Results
Ten percent of patients (n = 10,796) who were empaneled in one of 3 primary care sites were determined to have prediabetes on January 1, 2005, based on laboratory values. Of those patients, the prevalence of patients with baseline glucose of 110–119 mg/dL was 2743 (25.8%); only 6.0% (n = 633) of patients had a baseline glucose of ≥120 mg/dL. The median fasting glucose was 106 mg/dL. More than 50% of the cohort was male and more than 40% were aged 65 years and older. The majority of the cohort (96.4%) was white and 83.5% were either overweight or obese. Baseline characteristics of the study population are presented in Table 1.
At 1 year of follow-up, 404 (3.7%) of those who had prediabetes had progressed to have diabetes. By 5 years, with a median (Q1, Q3) follow-up of 5.0 (4.3, 5.0) years, 1845 (17.1%) had progressed to have diabetes. Similarly, the 1-year estimated incidence rate of progression to diabetes was 38.6 per 1000 person-years and increased to 40.24 per 1000 person-years at 5 years.
Older age and being overweight or obese were independent predictors of an increased rate of progression to diabetes (Table 2). Among the nonwhite patients, Asians had the highest risk of progressing to diabetes and were nearly 2 times more likely (IRR = 1.75; 95% CI, 1.18–2.59) to develop diabetes at 5 years than whites after adjusting for body mass index and other demographic characteristics. Baseline glucose was likewise an independent predictor of progression; each unit increment increase in baseline glucose was significantly associated with a 12% increased risk of progression (Fig. 2). Similar results were seen using categorized levels of baseline glucose.
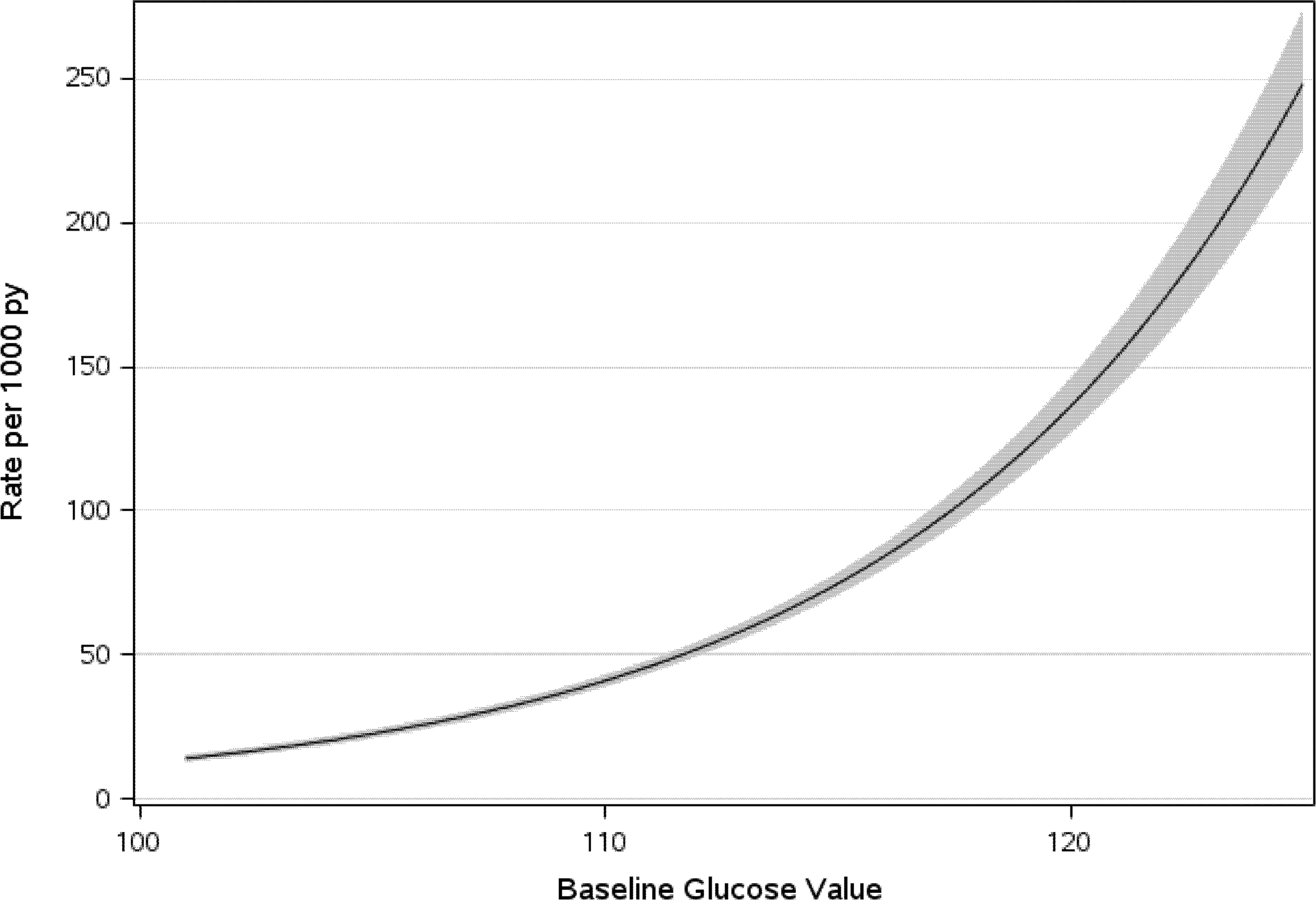
Progression rate per 1000 person-years estimated from Poisson regression model with 95% confidence intervals per unit increase in baseline blood glucose. py, person-years.
Adjusted for all other variables in the model.
BMI, body mass index; CI, confidence interval; IRR, incidence rate ratio; py, person-years; SE, standard error.
Generalized PAR statistics were estimated for 2 target groups: patients with baseline glucose levels from 110 to 119 mg/dL and those with levels ≥120 mg/dL. These subgroups were chosen as a steep rise in diabetes progression rate was observed among individuals with a baseline blood glucose level of 110 and higher. Outcomes based on percent reduction from baseline glucose and levels of adherence to a theoretical intervention are shown in Figure 3. The PAR for a 10-point reduction in glucose for patients in the 110–119 mg/dL group and assuming 25% adherence was 7.6% (95% CI = 6.5%–8.7%). In other words, if 687 (25%) patients with baseline glucose between 110 and 119 mg/dL adhere to an intervention that results in a 10-point reduction in their glucose level, this study estimates that the incidence of diabetes in the population (cohort) will be reduced by 7.6%. PAR for a similar percent reduction and adherence level in the target group of patients with baseline glucose of ≥120 mg/dL was 3.0% (ie, if 177 [25%] patients in this subgroup engaged in an intervention and achieved a 10-point glucose reduction, the estimated incidence of diabetes in the population will be reduced by only 3.0%).
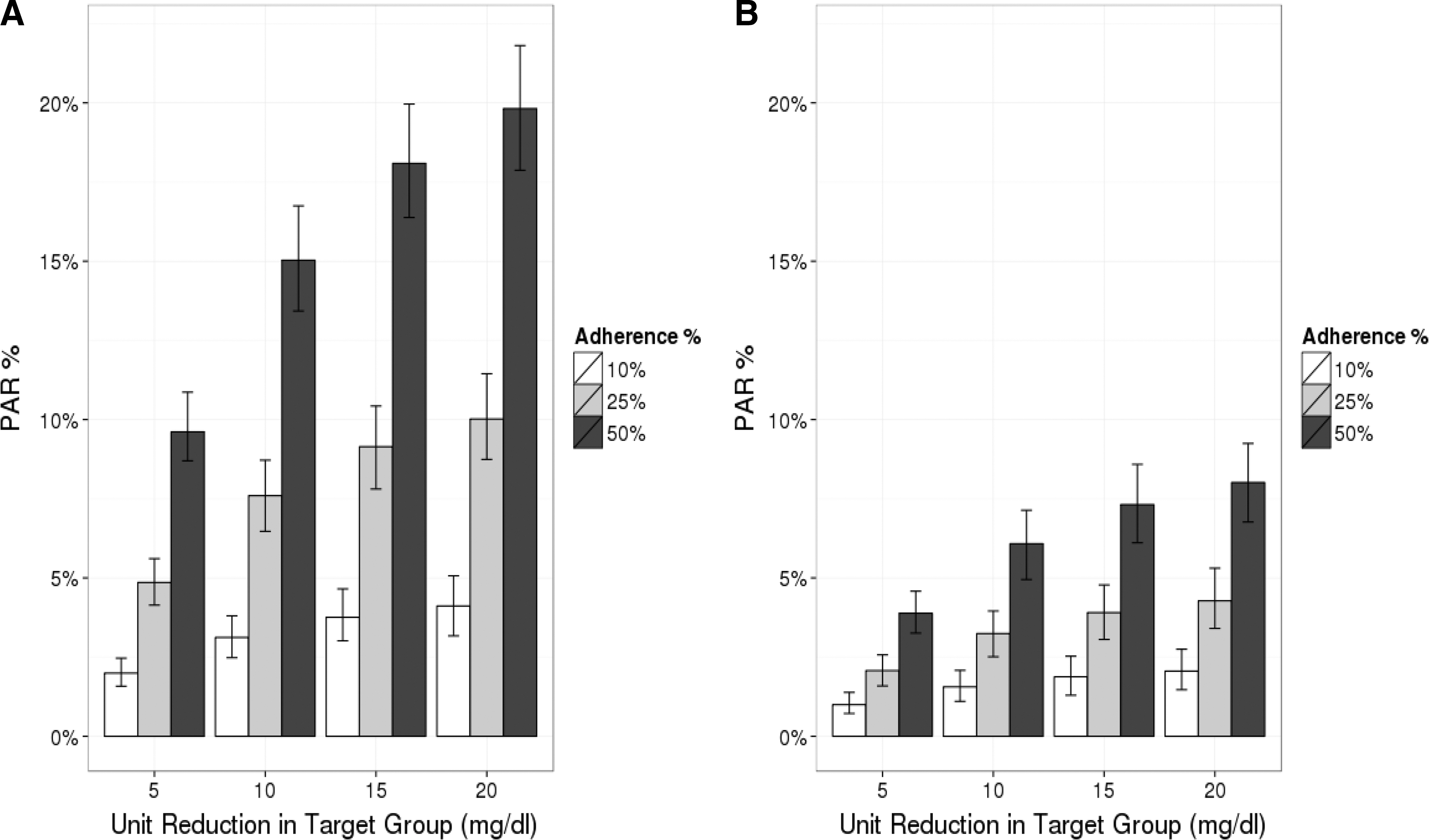
Percent reduction in PAR with baseline glucose decline by adherence status. The figure shows the target group patients with baseline glucose 110–119 mg/dL
The generalized PAR for a 10-point reduction in glucose for patients in the 110–119 mg/dL group, assuming 50% adherence, was 15.0%. This means that if 1371 (50%) patients with glucose in the range of 110–119 mg/dL adhere to an intervention and achieve a 10-unit glucose reduction, the incidence of diabetes in the population (cohort) is estimated to be decreased by 15.0%. In contrast, the estimated reduction in diabetes incidence given a similar 10-point glucose reduction and adherence level (50%) in the group with baseline glucose of ≥120 was only 6.0%.
Discussion
What was seen in this study and has consistently been described in the literature is the higher prevalence of prediabetes relative to diabetes (and its high likelihood of progression to diabetes), which nonlinearly increased over time and with a higher baseline blood sugar. At 1 year, the incidence rate was 38.6 per 1000 person-years and increased to 40.24 per 1000 person-years at 5 years. This finding is not far from a reported pooled incidence rate of 35.6 per 1000 person-years that was obtained after a meta-analysis of 70 studies. 15 The increased progression rate with higher baseline blood sugar also is not surprising. Prediabetes is associated with simultaneous presence of insulin resistance and beta islet cell dysfunction abnormalities that start before overt diabetes is seen and is a continuum state. 23 These results, thus, reinforced the need for early intervention.
Older age, overweight, and obesity were identified to be independent predictors of an increased rate of progression to diabetes within 5 years. Again, this observation is well aligned with previously reported data. 24 –26 Being Asian or Hispanic also was an independent risk factor, a finding consistent with other published data. 16,27,28 Although the underlying cause of this excess risk in these population groups is still not completely understood, several possibilities have been suggested, including innate biological susceptibilities, lifestyle behaviors, and environmental triggers. 29 –31 It is likewise well established that baseline glucose level is significantly associated with an increased risk of progression to diabetes 13,32 ; however, the present study results demonstrated that the risk of progression did not vary linearly with the baseline glucose level. Instead the risk appeared to be lower in those with baseline glucose of 100–110 mg/dL, but increased substantially among those with baseline glucose of 111 mg/dL or higher. Because each unit rise in glucose was associated with an increased risk, it would imply that the entire cohort of individuals with prediabetes would need to be targeted with interventions to prevent progression to diabetes. This approach is neither resource nor cost-efficient, particularly from a population health perspective. The present study proposed modeling an optimum target group for intervention that would potentially result in the largest effect on the overall population.
Using generalized PAR statistics to assess the potential effect of a hypothetical intervention that results in reduced blood glucose levels among persons with prediabetes, this study found that a greater risk reduction in diabetes progression can be achieved when the group with baseline glucose in the range of 110–119 mg/dL is adherent to an intervention with resultant reduction in glucose levels. The PAR is dependent on both relative risk and prevalence. Hence, even though the group with higher blood glucose levels had higher risk for progression, a greater overall risk reduction in the total population is seen in the mid-risk group, with glucose levels between 110 and 120 mg/dL. This is because more patients are in that group compared with the higher glucose level group (prevalence of 25.8% vs. 6.0%). Moreover, while individuals with prediabetes whose glucose levels fall above 120 mg/dL may inherently be more motivated to participate and adhere to an intervention, these results showed that programs focused on motivating those with lower glucose levels to make lifestyle changes may achieve greater overall risk reduction in diabetes 5-year progression among this population group.
The prevalence of prediabetes in this population, while closely parallel with those of other reported data across different population groups, 26,33 –35 is notably lower when compared with the prevalence rate of prediabetes in the United States, which was estimated to be ∼30% in 2005–2006. 36 Prevalence rates of prediabetes increase with advancing age; more than a third of the study cohort were adults, aged 20–55 years, which could account for the lower prevalence when compared with predominantly older population groups. The present study had stringent inclusion parameters and excluded results from laboratory tests obtained during hospitalization or during pregnancy as well as laboratory test results falling within the prediabetes range, but associated with an ICD-9 code of diabetes. There is less heterogeneity in the distribution of ethnic groups in the present study cohort, with a majority being white; this also could have lowered the prevalence. Several studies have shown that the epidemiology of prediabetes depends on the diagnostic methods used. Using HbA1c has been associated with lower prevalence rate; combining both fasting glucose and HbA1c may provide a more accurate figure. 14,37,38 This study identified prediabetes based on either fasting glucose or HbA1c results, which could account for some differences in findings when compared with studies that used other epidemiologic bases to determine prediabetes prevalence. The bottom line is that there continues to be no consensus on what defines prediabetes as several diagnostic criteria for its identification exist and confirmation of the optimal reporting method remains to be achieved.
This study has several strengths. To the authors' knowledge, no previous study has published data on PAR in a cohort with prediabetes; therefore, this reflects an important contribution for planning interventions. Robust data already exist that confirmed the effectiveness of lifestyle modification in diabetes prevention. 39 –41 This study intervention is hypothetical, but any of these well-reported lifestyle measures can be adopted when implementing interventions among patients with prediabetes in clinical practice. This work provides guidance regarding which subgroups have the potential to benefit the most from these interventions and suggests that more research is needed that prospectively compares intervention effects in various subgroups of patients with prediabetes. Such work will shed more light on who would optimally benefit from a population standpoint and guide decisions as to where intervention measures are best allocated.
This study relied on clinical data to identify the cohort; thus, eliminating bias related to self-report. A cross-check was performed for any ICD-9 diagnosis of diabetes as some patients with well-controlled disease may have fasting glucose or HbA1c within the prediabetes range. Although these measures may have accounted for the lower prevalence of prediabetes seen in the study cohort, it also resulted in a more accurate estimation of prevalence and added strength to the study.
The PAR calculation assumes causality and it should be recognized that the reductions in glucose are hypothetical, model dependent, and untested in a clinical setting. Although multiple regression models have consistently shown prediabetes to be an independent risk factor for the development of diabetes, the elimination of exposure to other risk factors that likewise influence disease risk may not always be feasible and should be taken into account when interpreting results. 42
The majority of the cohort comprised whites who reside in the Midwestern region of the United States; hence, the findings may not be generalized to other more diverse population groups. Similarly, all are community-dwelling adults with regular access to physicians in primary care clinics situated within an academic institution; these results may not represent other community-based practices. Despite these limitations, this study clearly showed that given the progressive trend in diabetes development among members of these primary care empaneled cohorts with prediabetes, integrating preventive interventions within primary care practice settings targeted toward these subgroups of patients could reduce its rate of progression to diabetes, a step toward improving population health.
Conclusion
Prediabetes is present in 10% of community dwellers served by primary care clinics in the Midwestern United States with a 1- and 5-year diabetes incidence rate of 38.6 and 40.2 per 1000 person-years, respectively. Using generalized PAR statistics among subgroups of individuals with prediabetes, optimum risk reduction in diabetes progression within the entire target population can be achieved when an intervention is successful in those with baseline glucose in the range of 110–119 mg/dL. Identifying optimum subgroups on whom to focus interventions is essential when planning and allocating resources for DPPs from a population health perspective.
Footnotes
Author Disclosure Statement
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received the following financial support for the research, authorship, and/or publication of this article: this project was supported by funding from the Population Health Scholar Program of the Robert D. and Patricia E. Kern Center of the Science of Health Care Delivery. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the Robert D. and Patricia E. Kern Center of the Science of Health Care Delivery.