
Abstract
Over the past decade, reimbursement in the US health care system has undergone rapid transformation. The Affordable Care Act and the Medicare Access and CHIP Reauthorization Act are some of the many changes challenging traditional modes of practice and raising concerns about practitioners' ability to adapt. Recently, physician satisfaction was proposed as an addition to the Triple Aim in acknowledgment of how the physician's attitude can affect outcomes. To understand how physicians perceive alternative payment models (APMs) and how those perceptions may vary by their organizational role, non-leader physicians (N = 31), physician leaders (N = 67), and health system leaders (N = 49) were surveyed using a mixed-methods approach. Respondents to the electronic survey, who were identified from a Jefferson College of Population Health program participant database, rated their organizations' responses to APMs and provided commentary. Analysis of the Likert scale quantitative data indicates a significant difference in ratings between the 3 groups, particularly between health system leaders and non-leader physicians. The aggregated Attitudes Toward APMs Scale indicates that health system leaders were statistically significantly more likely to rate themselves and their organizations as better prepared for APMs compared to non-leader physicians and physician leaders. Qualitative analysis of comments indicates that non-leader physicians are more negative of APMs, often expressing frustration at added administrative burdens, barriers to implementation, and inconsistent or unclear measurement requirements. These findings indicate that the negative feelings non-leader physicians and physician leaders, in particular, expressed could contribute to physician burnout and decreased professional satisfaction, and impede the effective implementation of APMs.
Introduction
T
Fee for service (FFS) is the predominant reimbursement model for health care in the United States, accounting for as much as 95% of office visits reimbursements. 2 Under FFS, health care providers are paid a predetermined amount for each billable service or procedure they provide the patient. 3,4 This system incentivizes the delivery of volumes of billable care while discouraging the provision of services that can reduce the aggregate demand for care by preventing disease or intervening earlier in the disease process. 5 Further, because traditional billing codes are not linked to the outcomes of those services, there is no financial incentive to provide higher quality care. 6 Even though clinical care accounts for only a small portion of a person's health status, 7 current FFS arrangements do not promote population health.
The ACA accelerated the movement from volume-based to value-based reimbursement through implementation of alternative payment models (APMs) in the Medicare program. The Centers for Medicare & Medicaid Services (CMS) has set a goal “…to have 85% of all Medicare fee-for-service payments tied to quality or value by 2016, and 90% by 2018.”
8
(p. 897) Private payers tend to follow Medicare's lead so it is expected that soon most payments for health care services will be based in some part on the service's value rather than just the fact it was delivered.
9
In 2015, the US Congress passed the Medicare Access and CHIP Reauthorization Act (MACRA).
10,11
CMS describes the key elements of the law as: • “Repeals the Sustainable Growth Rate Formula • Changes the way that Medicare rewards clinicians for value over volume • Streamlines multiple quality programs under the new Merit-Based Incentive Payments System • Provides bonus payments for participation in eligible alternative payment models (APMs)”
12
(p. 5)
MACRA and the subsequent regulations are more evidence of the move to APMs that encourage value-based clinical care. 13
ACA, MACRA, and related initiatives have introduced many new words, phrases, and acronyms to the lexicon of health care providers. Just keeping up with the new language of reimbursement is a challenge for some. In a 2016 Deloitte survey of US physicians, 50% of respondents stated they had never heard, “MACRA.” 14 Although detailing these terms is beyond the scope of this paper, it is important to note that, in aggregate, they describe a radical change in how health care will be delivered and paid for in the United States. Most importantly, accommodating to these changes will require significant transformation of the clinical workplace. Understanding clinician attitudes toward these changes is the focus of this research.
Previous work has sought to understand how reimbursement models have affected physician practices. The RAND Corporation 3 conducted a series of interviews with key stakeholders and found that many practices responded by promoting the use of team approaches to care, particularly in primary care practices. Resources also were channeled into data management capabilities, such as updating or purchasing new electronic health records (EHRs) and dedicating data entry staff and time. 3
Individual provider attitudes to changes in reimbursement are more difficult to assess yet they play a pivotal role in health reform. The Institute for Healthcare Improvement's Triple Aim organizes efforts to improve the quality of the US health care system into 3 categories: (1) improving the experience of care, (2) improving the health of populations, and (3) reducing per capita costs of health care. 15 Recently, a fourth aim was proposed: improving the provider experience. 16 Bodenheimer and Sinsky 16 argue that the Quadruple Aim acknowledges the important role clinicians play in achieving the other 3 aims. Lower physician satisfaction is significantly associated with diminished work effort. 17 Evidence suggests that burnt-out and overwhelmed physicians do not provide optimum care for their patients. 18 Although many factors are cited as a cause of physician burnout and difficulties in maintaining a satisfactory work–life balance, it is clear that understanding and adapting to a changing practice paradigm is a significant contributor. 3,17,19,20
In many practices, providers face inconsistent incentives. They are financially incentivized to increase revenues or provide more resource value units, while intrinsically motivated to improve patient care without cost considerations. 3 Friedberg et al 3 noted that the demand for physicians to complete added administrative work coupled with maintaining a high patient volume could be a potential source of physician burnout.
Because attitudes toward and knowledge of their institution's movement to APMs is likely to vary depending on the clinician's responsibilities within the organizational hierarchy, this study hypothesized that responses will vary by role: non-leader physician, physician leader, and health system leader. Research suggests that engaged frontline clinicians have a vital role to play in identifying and responding to health care quality issues, so it is likely that health systems with better informed frontline staff will adapt and respond more effectively to the changing reimbursement environment. 21 Further, Shanafelt et al 22 found that the leadership qualities of physician supervisors can affect burnout and satisfaction rates in their direct reports. In particular, being informed about system-wide changes was positively associated with overall satisfaction. 22
During their key stakeholder interviews, Friedberg et al 3 noted a deviation in attitudes between practicing physicians who had no leadership role and physician leaders; the former group was much less enthusiastic and more apprehensive about APMs compared to the latter. Non-leader physicians reported a higher level of discontent with increased documentation not associated with patient care. 3
Assessing providers' understanding of the current and future impact of APMs on the clinical setting is key to appreciating their readiness to adjust and embrace these new reimbursement paradigms. This study seeks to compare how non-leader physicians, physician leaders, and health system leaders perceive APMs and their organizations' responses to them. For the purposes of this paper, APMs are defined broadly to include the full range of reimbursement models that go beyond traditional FFS payments that lack quality or performance metrics.
Methods
Study design
A literature review of APMs and physician/health system responses to shifting reimbursement models assisted in the development of questions for an electronic survey (SurveyMonkey, Palo Alto, CA). The survey began with a question asking participants to self-identify as a practicing physician, health system leader, health payer administrator, none of the above, or other. The first 3 responses redirected participants to separate sets of questions based on their self-identified primary professional role. The “none” response thanked respondents for participating, as did the “other” response after they specified their primary professional role. The last option was added to gain further data about nonqualified respondents willing to provide additional information.
The 3 sets of questions (practicing physician, health system leader, health payer administrator) were designed for different levels of assumed knowledge though all had common themes. Each set began with a series of demographic questions. Practicing physicians received an additional branching question based on whether they identified as a physician or group leader. Each group of respondents was asked to identify the population health management vendor and reimbursement models that were in use in their organizations (data not included in this study).
A series of 5-point Likert scale questions, ranging from strongly disagree (1) to strongly agree (5) with N/A and I don't know options followed. Participants were asked to respond to a series of statements about their behavior or their organizations' responses under APMs. For example, practicing physicians (both leaders and non-leaders) were asked to rate their agreement with the statement “Under alternative payment models, my practice is benefitting financially.”
One to 2 additional Likert scale sections were included (dependent on self-identified group). Questions involved participants rating statements on FFS and population health. These data are not included in this study.
A comment box followed each Likert scale section to provide room for participants to voice their opinions. The survey was piloted with physicians and health system leaders, and revisions were made based on their input.
Sample
Participants were abstracted from an existing database of contacts from the College of Population Health at Thomas Jefferson University. The database contains individuals who have reported interest in population health-related topics. The database was crudely filtered to create a list of individuals believed to be practicing physicians, health system leaders and health payer administrators. The list was reviewed by hand to remove individuals who reside outside of the United States, work for government or military organizations, or are employed in a position other than the specified 3 groups.
An e-mail with a cover letter describing the project and a link to the survey was sent to 3303 potential respondents. Respondents were given 2.5 weeks to complete the survey with reminder e-mails at the halfway point and a few days before the deadline.
Statistical analysis
Descriptive statistics were performed on the demographic characteristics of non-leader physicians, physician leaders, and health system leaders. Responses of health payer administrators were removed because of lack of sufficient numbers. Analyses of variance (ANOVAs) with post hoc analyses were conducted for the 17 common “Under alternative payment models…” Likert scale questions. If a variable violated the homogeneity of variance assumption, Welch's t test was used. Independent samples t tests were conducted on the 5 additional Likert scale questions answered only by the practicing physicians (non-leader and leader). Both the ANOVAs and t tests were performed to determine if there was a difference in means between the groups. P < 0.05 was considered statistically significant.
A continuous variable was created using 16 of the 17 common Likert scale questions. These 16 were deemed representative of how prepared a respondent (and his/her organization) was for APMs. Three of the 16 variables were reverse coded to standardize the variable scales before an average of all variables was used to create the Attitudes Toward APMs (AAPM) Scale. Values were derived from only those respondents who answered at least 14 of the 16 Likert questions. The AAPM Scale ranges from 1 to 5 with 1 representing feelings of less preparedness for APMS and 5 representing feelings of more preparedness for APMs.
A qualitative analysis was conducted to analyze respondents' comments. A coding panel, consisting of the 2 authors (KP and DH) and 2 research assistants, hand coded the comments and classified the general tone of each comment as negative, neutral, or positive and identified common themes or messages. Coding decisions were made by unanimous agreement or through discussion until consensus was reached.
This study was deemed exempt from review by the Thomas Jefferson University Institutional Review Board.
Results
Demographics
Of the 3303 e-mail invitations sent, 242 responses were attempted. Of those, the following were excluded: not one of the 3 target groups, health payer administrators, respondents who did not answer any demographic questions, and duplicate attempts (Fig. 1). Approximately half of the self-identified health payer administrators did not complete any demographic questions and therefore the whole group was removed from the analysis. Several entries were removed as respondents completed the survey twice because of a link error in an e-mail reminder. Ultimately, the analysis included 31 non-leader physicians, 67 physician leaders, and 49 health system leaders.
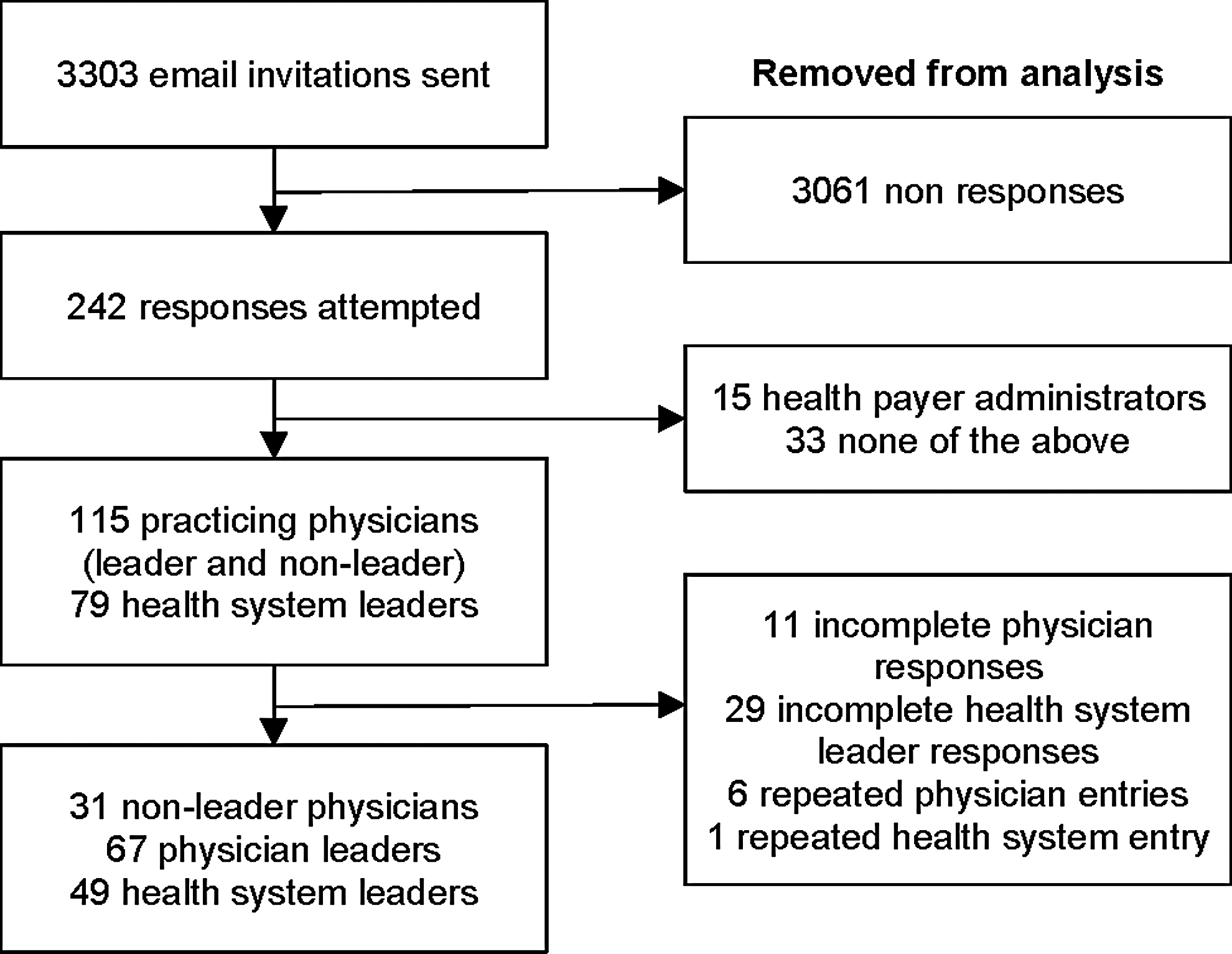
Identification of survey participants for analysis.
At least half of the respondents in the groups analyzed were from the northeast region of the United States, with Pennsylvania cited most often (Table 1). Non-leader physicians were much more likely to be practicing in an urban area compared to health system leaders and physician leaders. More than half reported that their organization was affiliated with an Accountable Care Organization or similar organization. There also was wide discrepancy among respondents as to which and how many population health management software vendors they used. Thirty-three respondents reported not using a vendor or not knowing compared to 114 who reported having at least 1 vendor (range 1 to 11).
ACO, accountable care organization.
Quantitative analysis
ANOVA and Welch's t test analyses identified differences in means between the 3 groups in 9 of the 17 common Likert questions (Table 2). Post hoc analyses revealed that most of the mean differences occurred between the health system leaders and the physician leaders and/or the health system leaders and the non-leader physicians. Generally, health system leaders were more accepting of APMs and reported that their systems were better prepared for the shifting reimbursement models compared to physician leaders and non-leader physicians. For example, health system leaders reported higher average agreement with the statement that the system's performance measures were used to improve patient care compared to physician leaders (P < 0.001) and non-leader physicians (P = 0.033). Health system leaders also rated their system's patients as more satisfied with the care they receive compared to non-leader physicians (P = 0.008). In contrast, physician leaders reported a lower professional satisfaction average compared to health system leaders (P = 0.02).
HS Leader–Physician Leader, P = 0.049; HS Leader–Non-Leader Physicians, P = 0.005.
Statements were averaged to form the AAPM scale.
Variables were reverse coded when averaged into the AAPM Scale.
HS Leader–Physician Leader, P = 0.009; HS Leader–Non-Leader Physician, P = 0.002.
HS Leader–Non-Leader Physician, P = 0.008.
Physician Leader–Non-Leader Physician, P = 0.047.
HS Leader–Physician Leader, P = 0.016; HS Leader–Non-Leader Physician, P = 0.047.
HS Leader–Physician Leader, P < 0.001; HS Leader–Non-Leader Physician, P = 0.033.
HS Leader–Non-Leader Physician, P = 0.011
Tukey's post hoc analysis did not identify any statistically significant differences between each pairing.
HS Leader–Physician Leader, P = 0.020.
HS Leader–Physician Leader, P = 0.004; HS Leader–Non-Leader Physician, P = 0.042.
EHR, electronic health record; HS, health system; ROI, return on investment.
In only 1 case, “Under alternative payment models, I expect the community my practice serves to be healthier in the next 3 to 5 years,” did Tukey's post hoc analysis reveal that there was a mean difference between physician leaders and non-leader physicians (P = 0.047). The non-leader physicians, on average, expected the community to be healthier in the future under APMs compared to physician leaders (Table 2).
Health system leaders also averaged higher on the AAPM scale compared to physician leaders (P = 0.004) and non-leader physicians (P = 0.042), indicating that they feel more prepared for the shifting reimbursement models (Table 2).
Qualitative analysis
The qualitative analysis revealed that most of the comments were written in a negative tone. Non-leader physicians expressed the most negative-toned comments (N = 13, 72%). Among physician leaders, just under half of the comments had a negative tone (N = 10, 42%). Health system leaders expressed the least number of negative comments (N = 2, 25%) though they also provided the fewest comments for analysis.
Many of the physician leaders' and non-leader physicians' negative-toned comments also expressed feelings of powerlessness, anger, frustration, and even hopelessness. One non-leader physician wrote: “I am in an academic practice. Central administration dictates everything. The faculty is completely disenfranchised.” Another non-leader physician wrote: “For the life of me I can't get cost data, even for tests we run in house. How am I supposed to control costs if I don't know how much things cost!?”
There was only 1 positive-toned comment in which the non-leader physician remarked that “there is still the possibility of moving beyond the current mess.”
The coding panel identified 6 themes: Measures; Influence of socioeconomic/community health factors; Lack of changes; Barriers; Future predictions; and Suggestions.
Measures
Both physician leaders and non-leader physicians commented on performance measures, usually negatively as in that they were inappropriate or unclear. Three physician leaders commented on the lack of adequate performance measures, particularly wanting outcome measures rather than process measures. One wrote:
It is good to have both structural and process outcomes, but they should be subordinate to the [health] outcomes with the exception that some basic structure and process is indespensible [sic], such as, for example, an emergency room having a defibrillator that works and providers who are trained well to use it properly.
Non-leader physicians also commented on measures, focusing on the patient-provider interaction as a more important performance measure. One non-leader physician wrote:
Yardsticks of quality measures currently used do not measure actual patient outcome and satisfaction. They miss the basic premise that a patient-doctor encounter is the one that generates the quality measures; the ones the bean counters are waiting to pounce on. A good clinician spots “the uncommon manifestations of common disorders and common manifestations of uncommon diseases.” What the mind does not know the eye does not see. How do you measure that? How do you encourage and reward that?
Another non-leader physician wrote that the community and individual outcome measures that were being captured did not reflect his patient panel and therefore were uninformative. No health system leaders made comments under this theme.
Influence of socioeconomic factors or community health factors
Physician leaders in particular commented on nonclinical factors, such as access, high co-pay costs, and behavior, that influence the health of their patients. One physician leader expressed frustration with his patients by writing:
There seems to be no patient responsibility on [sic] their own health and the majority of burden for health is on the health care providers. COPD's still smoke, diabetics still gaining weight. Patients come to the office unable to pay [for] Bactrim when they admit [to] drinking beer 4 bottles a day.
Not all factors are within the control of the patient. One non-leader physician wrote:
As a physician taking care of [an] inner city population, I am appalled at the prevalence and scourge of obesity, mental illness, homelessness, and violence in the community. Unless the elected representatives spend time in the clinic where they can meet this faceless population, Americans will continue to look the other way while the cancer within us grows.
Lack of changes
Comments from all 3 groups noted either the lack of payment reform or delivery redesign occurring within their organizations. One physician leader expressed frustration, writing:
Despite a lot of “talk” on quality and collaborative care, little has been done to move the cheese. It's basically all talk and clever billing and accounting practices. Meanwhile, the hospital's margin has tanked and there is literally an across-the-board hold on any new hiring. Do more with less but be held responsible for the outcomes.
Another physician leader remarked that his/her “almost 100% FFS” organization lacks commitment to population health, noting that “… there is no serious effort toward community health. The absolute foci are throughput, LOS [length of stays], and margin.”
Barriers
Monetary and nonfinancial barriers to APM (and population health management) implementation were expressed by all 3 groups. The coding panel identified 6 barrier subthemes: cost, organizational, clinical, time, data/technology, and systemic.
Both physician leaders and non-leader physicians expressed concerns over the inadequacy of reimbursement. One physician leader wrote:
We are currently being asked to do more with less. I do not see the health care economy changing. Our Medicare and Medicaid patient populations are rising, they are less healthy, and we are getting reimbursed less to take care of them. This is not a sustainable situation… period!
Organizational barriers were seen across all groups. In particular, both health system leaders and non-leader physicians pointed to organizational culture as an area where strong leadership and a clear mission are needed to move the organization toward success under APMs. One health system leader wrote:
Vision, alignment, and execution are critical elements of success. [Organizations] Need to be innovative and creative to survive; [they] need to be agile, adaptable, integrated, coordinate [sic], and collaborative.
As evidenced by one non-leader physician's comments, not all organizations have a clear direction: “Big disconnect between divisional leadership, their lofty goals, and huge discrepancy with hopes and aspirations of where we need to be in 5–10 years.”
Clinical barriers were identified by physician leaders and non-leader physicians. These comments noted that specialists are siloed along the continuum of care, resulting in poorer health outcomes for the patient. One non-leader physician remarked:
Everyone seems to be dumped into nursing home settings, which are fine for conditions needing rest and time but are really not set up to handle complex rehab issues. Patients tend to go home without adequate back-up, outpt [sic] follow-up, etc. I frequently see them bounce back into the acute care setting.
Two physician leaders' comments noted time barriers. One remarked: “My practice/me do not have the TIME to do any of this.” Another noted that time spent on data entry in EHRs was taken from patient-provider interactions and “careful thought processes.”
Professionals from all 3 groups identified data and technology-driven barriers. A health system leader and 2 physician leaders commented that any improvements in data management systems fell short of true progress in population health because of the lack of interoperability among EHRs and the inability to access meaningful data. A non-leader physician expressed concern over the lack of qualified analysts:
The whole process of analytics suffers in our organization, from asking the right questions, collecting the right data in a cost-effective and timely manner, correctly displaying the data in an effective way, and analyzing and making appropriate conclusions. We have too many middle level and upper echelon administrative personnel using statistics and making pronouncements for which they have little in background training.
The last barrier subtheme identified was systemic barriers. Both physician leaders and non-leader physicians noted issues involving the health care system at large. One non-leader physician wrote:
[The] Medical profession is the only one where professional experience is not valued nor cherished. A senior accountant, lawyer or an architect commands a much higher hourly wage than the younger ones. You are expected to pay for the service you get. There is an urgent need to replace the archaic CPT codes with something more dynamic, that…reflects physician's qualifications, expertise and skills. I have ideas, but I will be whistling in the dark!
Future predictions
All 3 groups made predictions about what to expect in the future—whether that prediction was specific or that the forecast was unclear. Several were concerned about their field/organization's ability to survive in an era of constrained funding. One non-leader physician wrote:
Because I am providing care at the end of the line and the system is geared to reimburse procedures and not follow-up and counseling, I don't understand how rehab services in general are going to be able to survive.
Several respondents noted that the changing payment reform was unsustainable. One physician leader wrote:
…The Medicare and Medicaid populations and subsidized ACA plans continue to grow, yet the reimbursement continues to drop. It's simply not a sustainable situation. Because I live in both worlds–frontline clinician and administrator–I empathesize [sic] with both sides. Sure, we have a foot in both canoes… the problem is that both canoes are taking on water quickly and I am afraid that many of us in health care have forgotten how to swim!
As noted above, the only positive-toned comment expressed hope for the future.
Suggestions
This last theme included comments in which respondents suggested improvements to the current health care system. Only 2 comments suggested the continued use of FFS. One physician leader recommended a single-payer model and another praised the existence of direct primary care. A non-leader physician recommended that:
…Payers have a responsibility to align incentive structures, to simplify them, to make performance more transparent, and to assure that payment levels are rational to support the care required.
Discussion
APMs use a variety of metrics to encourage providers to provide higher quality and more efficient care that will keep their patient populations healthier for longer. Clinical satisfaction also plays a role in the delivery of care so it is essential to understand clinician perspectives on APMs. This research indicates that physicians, particularly those not in leadership roles, are less optimistic about APMs. In general, they are more likely to perceive their organizations as having slower progress under APMs, and to express more negativity and frustration in their comments.
This study was an observational study with a convenience sample of participants who already self-identified as having population health-related interests. Additionally, the survey experienced low response rates and significant attrition. More than 20% of physician and health system leaders who started the survey did not respond after the first question, and of those who answered the demographic questions, 20% failed to finish the survey in its entirety. The self-selection bias among respondents suggests that the responding population may express views that are different than the general provider population. Respondents choosing not to complete the entire survey may have felt unprepared to answer the questions, skewing the overall response in favor of greater APM knowledge.
Given that this population may be more knowledgeable about population health and yet still has disparaging views on APMs, the results from this observational study paint a bleak image of how providers, particularly those with limited leadership responsibilities, are reacting to the shifting reimbursement paradigm. This research in combination with previous studies 17,18 suggests that the added burdens physicians face under APMs are having the opposite intended effect of improving patient care. Both leader and non-leader physicians rated 2 of the 4 tenets of the Quadruple Aim lower than health system leaders (professional satisfaction and patient satisfaction)—the opposite of Friedberg et al's 3 finding that quality did not diminish.
Potentially contributing to professional dissatisfaction among providers are the ever-changing regulations for reimbursement. For instance, MACRA is just the latest CMS initiative that is likely to radically change the professional lives of the respondents. Non-leader physicians know they will be affected by the effort but have neither the time nor expertise to fully appreciate its implications. Thus, they are more likely to express feelings of hopelessness and lower levels of satisfaction than their more empowered leaders, suggesting they are struggling in a continuously shifting field.
During the study, several respondents contacted the researchers with reluctance to complete a series of questions about which specific APMs were employed at their organizations (data not included in this paper). Given that participants had difficulty identifying APMs at their organizations and often an organization employs multiple APMs at any given time, participants responded to the umbrella statement “Under alternative payment models….” Therefore, none of the results can be attributed to a single APM. This difficulty some respondents have in differentiating among different types of APMs is further evidence in support of this study's conclusion that many providers are ill-prepared to respond to a changing health care reimbursement environment.
Survey respondents voiced concerns over inconsistent incentives. They faced increased administrative burdens (nonclinical) while being expected to focus on performance measures for the care they deliver. Physicians (leaders and non-leaders) expressed greater dissatisfaction with outcome measures and how they were unclear or inappropriate.
The clinical workplace is really no different than other institutional settings. Leaders, by virtue of their responsibilities, tend to have a better understanding of the big picture and future direction, while frontline workers often feel ill-informed and frustrated in their efforts to achieve organizational goals. Management guru Tom Peters said, “It is necessary to ‘dehumiliate’ work by eliminating the policies and procedures (almost always tiny) of the organization that demean and belittle human dignity.” 23 (p. 68) The complex task of transitioning organizations to APMs will be especially challenging in the coming years. Institutional leaders and health care policy makers should take care to address the concerns and attitudes of the clinicians who deliver the care. The Deloitte survey 14 also found that physicians were more likely to accept adoption of APMs when provided with a brief explanation, so specific education about these changes could be incorporated into professional continuing education programs.
Reimbursement models vary by provider specialty and region of the United States potentially affecting perceptions about the movement from FFS to APMs. This research did not analyze these separately. In addition to providers, other stakeholders, such as insurers and patients, are affected by APMs. This study attempted to include health payer administrators, but lack of response prohibits their inclusion in the analyses.
As noted, because of the limited and observational nature of this study, extrapolations to all US physicians should be done with care. The AAPM Scale developed for this survey is a useful tool that can be used to assess responses to more broad-based surveys.
Conclusion
This study demonstrates a statistically significant difference in attitudes among 3 groups of providers: non-leader physicians, physician leaders, and health system leaders. These groups have varying degrees of administrative responsibilities, and ability to understand and respond to APMs. Non-leader physicians clearly articulate less awareness and greater frustration with APMs than more empowered health system leaders. Understanding that physician satisfaction is directly linked to clinical outcomes, addressing the causes of provider frustration should be seen as an important quality improvement effort.
The transition from FFS to APMs, while laudable in the effort to improve health outcomes and control costs, is fraught with challenges for health care practitioners. If these goals are to be achieved, then care must be taken to ensure that all clinicians are fully engaged and empowered in the effort.
Footnotes
Acknowledgments
The authors thank their research assistants, Kathryn Tadduni and Rebecca Harris, and their colleagues at JCPH for assistance.
Author Disclosure Statement
Dr. Harris and Ms. Puskarz declared no conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors received the following financial support: This study was funded by Accenture.